










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Implementing evidence-based oral health practices is essential to the general health and quality of life of patients. 1 Dentists are at the core of these practices; they are required to make tailored clinical decisions, combining surgical/operative interventions and medications to treat any condition affecting oral health. Their role is essential in providing high-quality dental care and personalized quality use of medicines, taking into account the clinical context and other medications patients take. Therefore, dentists should continuously improve their knowledge, competencies, and practice about medications, such as their side effects, contraindications, and interactions, to define the best treatment for each patient. 2 Studies around the world revealed numerous prescription errors (e.g., wrong molecules, doses, or treatment duration, inadequate prescriptions in special populations such as the elderly and children), leading to detrimental outcomes on patient care: misuse and abuse of opioids, antimicrobial resistance leading to complications and prolonged hospitalizations, potential harm and adverse drug reactions related to drug-drug interactions, increased unnecessary pharmaceutical expenditures and costs, especially in an already overburdened healthcare system such as in Lebanon. 3 - 12 Reports from Lebanon highlighted inappropriate drug prescribing, denoting the persistence of this problem throughout the years. 11 To our knowledge, studies assessing inappropriate prescribing practices among dental care providers in Lebanon are scarce, and the few studies available have focused on antibiotics, when the problem encompasses other medications. 11 , 13 Moreover, the lack of national treatment guidelines makes dentists rely on various international guidelines, which might be different sometimes, resulting in confusion among prescribers. 14
For all these reasons, identifying contributing factors to inappropriate drug prescribing in Lebanon would help us better shape the size of the problem and implement a clear strategic plan to improve prescription practice and raise awareness of dentists about the proper use of medications. The ultimate goal would be to establish policies to promote the critical role of dentists in medication safety.
Therefore, the primary objective of our study was to assess drug-prescribing perception, practices, in addition to drug-related educational needs among dental care providers in Lebanon. The secondary objective was to evaluate the need for further interprofessional collaboration between dentists and pharmacists regarding medications and oral health.
METHODS
Study design
The ethical committee at Saint-Joseph University approved the study protocol (USJ-2016-63). All participating dentists gave their consent by accepting to complete the online survey.
An exploratory cross-sectional study was carried out between November 1 st , 2016, and January 31 st , 2018, using an online questionnaire targeting a sample of dentists from all Lebanese districts (Beirut, Mount Lebanon, North, South, and Beqaa).
Sample size calculation
Since this study is exploratory, and in the absence of previous data about the Lebanese dentists' needs, except for general observations regarding insufficient pharmacological education in this population, the Epi Info™ software (Centers for Disease Control and Prevention, Epi Info™) calculated a minimum of 131 participants, considering an educational need of 50%, a confidence interval of 95%, and an alpha error of 8.5%.
Data collection process
Data were collected using the snowball technique. The questionnaire was developed on Surveytuner, and the link was sent to the Faculty of Dental Medicine at the Saint-Joseph University and the Lebanese Dental Association in North Lebanon, to be dispatched by e-mail to Lebanese dentists who were asked to share it with their colleagues. Reminders were sent every two weeks for a total of 3 reminders per contact.
The study objectives were stated on the first webpage of the survey, and participation was voluntary. A total of 137 dentists enrolled and completed the online questionnaire that required approximately 15-20 minutes to complete.
Questionnaire
The online questionnaire was available in French or English, the two languages of dental education in Lebanon, and the most commonly spoken languages by the Lebanese population in addition to Arabic.
The questionnaire consisted of mandatory closed-ended questions prepared according to previous surveys and adjusted for the Lebanese population. 15 , 16 It included four different sections: 1) Socio-demographic and work characteristics (age, gender, level of education, academic activity - being members of university staff, specialty, location of the dental office, years of practice, and working hours per week); 2) Questions about to drug-prescribing perception; 3) Questions related to drug-prescribing practice; and 4) Questions related to the collaboration with pharmacists regarding their respective roles in providing appropriate counseling to patients.
The questionnaire initially created in French was translated into English by a pharmacist, then back into French by another pharmacist to ensure translation accuracy. Both versions were pilot-tested on a sample of ten dentists before starting data collection. The few translation discrepancies detected were resolved by investigators (pharmacists and dentists) in agreement with the two translators. The final datasheet did not include the results of the sample.
Measurements
Two indexes were created for this study. The first evaluated self-confidence of dentists in prescribing medications, while the second assessed their confidence in pharmacists. Both indexes were measured on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). For each index, the total score was calculated by summing the answers to all questions.
The self-confidence index consisted of the following questions: "Dental care providers feel confident when prescribing drugs to a special group of patients such as children, the elderly and pregnant woman"; "Dental care providers feel confident when prescribing drugs to patients with special conditions such as Endocrine & Metabolic diseases, Gastrointestinal symptoms, Cardiovascular diseases, Respiratory diseases, Organ impairment, Cancer, Neurological disorders, Drug allergies & intolerances" (each of these conditions was considered as a different question).
The confidence in pharmacists was assessed by three questions: 1) Do you encourage patients to talk to pharmacists about their medications; 2) Do you consider that oral health advice should be provided in community pharmacies; and 3) Do you consider that your patients get enough counseling from their pharmacist about oral health.
Statistical analysis
The online system automatically generated datasheets allowing statistical analysis on SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp. A descriptive analysis was performed using frequencies and percentages for multinomial and dichotomous variables, while means and standard deviations were reported for continuous variables. Student t and ANOVA tests were used to compare two and three or more means, respectively. Since the normality and homoscedasticity assumptions were not met in the linear regressions, two logistic regressions were performed, taking the dichotomized dentist's self-confidence in prescribing drugs and dentist's confidence in pharmacists indexes as dependent variables, respectively. Dependent variables were divided based on each score's median. Variables that showed a p<0.2 in the bivariate analysis were taken as independent variables in the final model. We forced age and implication in academia into the models due to their importance. Significance was set at p<0.05.
RESULTS
A total of 137 dentists completed the online survey. The mean age of participants was 42.17 (SD 13.78) years, and 59% were females. Almost half of the sample had an academic activity (53.3%) and more than 12 years of experience (56.9%). Table 1 summarizes the socio-demographic and socioeconomic characteristics of the participants.
Table 1. Sociodemographic characteristics of the participants
| Gender; N (%) | |
| Male | 81 (59.1%) |
| Female | 56 (40.9%) |
| Educational level; N (%) | |
| Doctor in dentistry | 60 (43.8%) |
| Master's degree | 55 (40.1%) |
| PhD | 11 (8.05%) |
| Other degrees | 11 (8.05%) |
| Academia/Teaching; N (%) | |
| No | 64 (46.7%) |
| Yes | 73 (53.3%) |
| Specialties; N (%) | |
| Periodontics | 45 (32.8%) |
| Endodontics | 25 (18.3%) |
| Oral and maxillofacial surgery | 14 (10.2%) |
| Pediatric dentistry | 14 (10.2%) |
| Oral and maxillofacial pathology | 10 (7.3%) |
| Orthodontics | 9 (6.6%) |
| Other specialties | 20 (14.6%) |
| Years of practice; N (%) | |
| Up to 3 years | 35 (25.5%) |
| More than 3 years and less than 12 years | 24 (17.5%) |
| 12 years or more | 78 (56.9%) |
| Age in years; mean (SD) | 42.17 (13.78) |
The mean self-confidence in prescribing drugs index was 26.69 (SD 7.06) (median=27; minimum=9; maximum=42) and that of the confidence in pharmacists 9.40 (SD 2.39) (median=10; minimum=4; maximum=15).
Table 2 presents the results of the dentists' perception of prescribing practice. The majority of dental care providers considered that they have fair to good perceived knowledge in pharmacology and therapeutics (80.3%), but only 30.7% reported to be sufficiently equipped to prescribe safely (strongly agree/agree). Prescribing for older patients, dosing, medication use in pregnancy, avoiding drug interactions, and assessing adverse reactions (explore whether the side effect reported by the patients might be related to a prescribed drug and report it to the pharmacovigilance system), were associated with low percentages of perceived knowledge ( Table 2 ).
Table 2. Drug-prescribing perception questions
| Rate your perceived knowledge in clinical pharmacology & therapeutics | |
| Poor | 5 (3.6%) |
| Fair | 54 (39.4%) |
| Good | 56 (40.9%) |
| Very good | 20 (14.6%) |
| Excellent | 2 (1.5%) |
| Dentists are sufficiently equipped to prescribe safely | |
| Strongly agree | 6 (4.4%) |
| Agree | 36 (26.3%) |
| Nether agree nor disagree | 55 (40.1%) |
| Disagree | 34 (24.8%) |
| Strongly disagree | 2 (1.5%) |
| Don't know | 4 (2.9%) |
| Broadest drug perceived knowledge of dentists | |
| Prescribing in the elderly | 76 (55.5%) |
| Dosing | 56 (40.9%) |
| Drug use in pregnancy | 49 (35.8%) |
| Avoiding drug interactions | 44 (32.1%) |
| Assessing adverse drug reactions | 40 (29.2%) |
Figure 1 summarizes the level of confidence of dentists in prescribing. The highest level of confidence was noted for prescribing to patients with gastrointestinal symptoms, cardiovascular diseases, and endocrine/metabolic diseases (strongly agree/agree: 57.7%, 51.1%, and 44.5%, respectively), while the lowest level was expressed with patients with organ impairment, cancer, and neurological disorders (disagree/strongly disagree: 53.3%, 48.9%, and 46.7%, respectively).
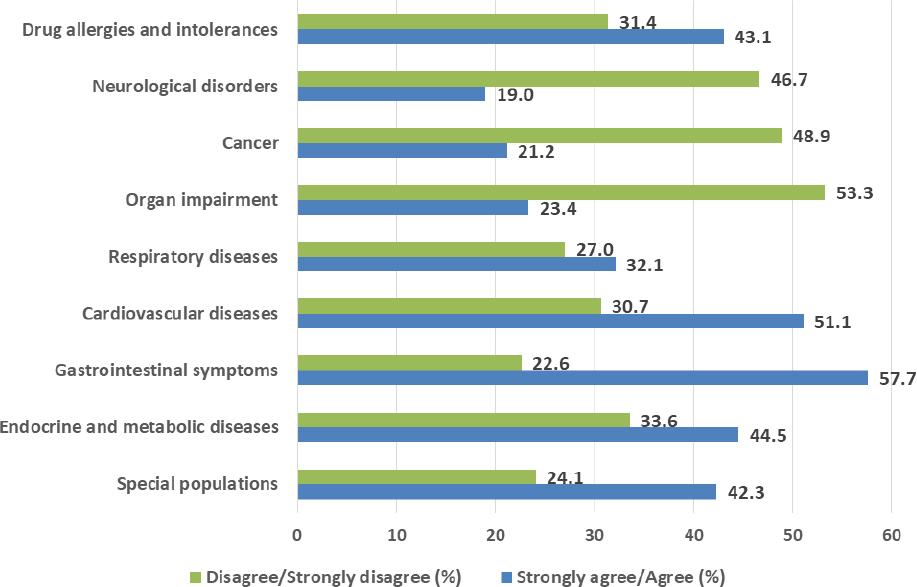
Figure 1. Level of confidence of dentists when prescribing to special populations or patients with particular diseases†Diseases as detailed in the questionnaires: Neurological disorders such as epilepsy, Parkinson's disease; Organ impairment such as impaired liver or renal functions; Respiratory diseases such as asthma and chronic obstructive pulmonary disease; Gastrointestinal symptoms such as gastric or duodenal ulcer; Endocrine & metabolic diseases such as hypothyroidism, diabetes, high blood pressure.
The most prescribed drug classes included mainly antibiotics (87.6%), analgesics (86.9%), and nonsteroidal anti-inflammatory drugs (NSAIDs) (82.5%). Most dentists turned to pharmaceutical companies and medical representatives (78.8% and 54.7%) to get information on medications; they also considered electronic references/databases, medical journals, and clinical pharmacists as reliable sources for information ( Table 3 ). The majority of dentists used drug information to manage their patients (78.1%), but only 64.3% reported routinely checking a reference before prescribing (strongly agree/agree), even though almost 61% disagreed on having difficulties getting any drug information (disagree/strongly disagree). The most common prescribing incidents were the lack of data regarding patients' allergies (54%) and wrong treatment duration (46.7%). Most dentists declared spending no more than 10 minutes explaining the drug regimen to patients ( Table 3 ).
Table 3. Practice questions regarding drug prescriptions
| Provide examples of most prescribed drug classes in the dental office | |
| Antibiotics | 120 (87.6%) |
| Antifungals | 21 (15.3%) |
| Anesthetics | 40 (29.2%) |
| Muscle relaxants | 32 (23.4%) |
| Analgesics | 119 (86.9%) |
| Anxiolytics | 22 (16.1%) |
| Anti-inflammatory drugs | 113 (82.5%) |
| Drugs for xerostomia | 9 (6.6%) |
| Fluoride containing products | 61 (44.5%) |
| Chlorhexidine containing products | 86 (62.8%) |
| People who provide you with drug information | |
| Clinicians | 60 (43.8%) |
| Clinical pharmacists | 62 (45.3%) |
| Community pharmacies | 17 (12.4%) |
| Medical representatives | 75 (54.7%) |
| Lectures | 16 (11.7%) |
| Resources you rely on when seeking drug information | |
| Pharmacology courses | 78 (56.9%) |
| Internet sites | 48 (35%) |
| Electronic references and databases | 97 (70.8%) |
| Medical journals | 96 (70.1%) |
| Pharmaceutical companies | 108 (78.8%) |
| Other sources | 9 (6.6%) |
| Use of drug information for | |
| Managing current patients | 107 (78.1%) |
| Continuing professional development | 91 (66.4%) |
| Training and teaching | 37 (27%) |
| Use in research | 23 (16.8%) |
| Checking a reference source routinely before prescribing drugs | |
| Strongly agree | 39 (28.5%) |
| Agree | 49 (35.8%) |
| Neither agree nor disagree | 26 (19%) |
| Disagree | 9 (6.6%) |
| Strongly disagree | 7 (5.1%) |
| Not applicable/Don't know | 7 (5.1%) |
| Difficulty obtaining drug information | |
| Strongly agree | 5 (3.6%) |
| Agree | 18 (13.1%) |
| Neither agree nor disagree | 30 (21.9%) |
| Disagree | 53 (38.7%) |
| Strongly disagree | 30 (21.9%) |
| Not applicable/Don't know | 1 (0.7%) |
| Most common incidents during dental prescription | |
| Not asking for allergies | 74 (54%) |
| Wrong treatment duration | 64 (46.7%) |
| Wrong posology | 54 (39.4%) |
| Not knowing the brand names | 19 (13.9%) |
| Drug interactions | 48 (35%) |
| Time spent prescribing and explaining a drug regimen to your patient | |
| Less than 5 minutes | 61 (44.5%) |
| 5-10 minutes | 61 (44.5%) |
| 10-15 minutes | 10 (7.3%) |
| > 15 minutes | 1 (0.7%) |
| Lack of time to explain a drug regimen | 2 (1.5%) |
| Patient should counsel his pharmacist for more info | 2 (1.5%) |
The majority of dentists considered that seminars and close collaboration with pharmacists were the primary sources to update their information about medications, and 76.6% agreed on the importance of including pharmacology courses in the dental curriculum. The majority (61.3%) considered that oral health counseling should be provided in community pharmacies, but only 52.6% encouraged patients to talk to pharmacists about their medications ( Table 4 ). Moreover, only 15% of dentists thought that their patients got enough counseling from their pharmacist about oral health; the majority did not consider this to be the case or did not know.
Table 4. Attitude questions regarding prescribing practices role in oral health
| Procedures dentists consider necessary to stay updated about drugs | |
| Seminars | 105 (76.6%) |
| Training and lectures | 44 (32.1%) |
| Collaboration between dentists and pharmacists | 90 (65.7%) |
| Improving pharmacotherapy skills of dental students | 72 (52.6%) |
| Incorporate new modules related to pharmacology in the curriculum | |
| Strongly agree | 67 (48.9%) |
| Agree | 38 (27.7%) |
| Neither agree nor disagree | 16 (11.7%) |
| Disagree | 8 (5.8%) |
| Strongly disagree | 7 (5.1%) |
| Not applicable/Don't know | 1 (0.7%) |
| Oral health advice should be provided in community pharmacies | |
| Strongly agree | 27 (19.7%) |
| Agree | 57 (41.6%) |
| Neither agree nor disagree | 18 (13.1%) |
| Disagree | 22 (16.1%) |
| Strongly disagree | 13 (9.5%) |
| Encourage patients to talk to pharmacists about their medications | |
| Strongly agree | 32 (23.4%) |
| Agree | 40 (29.2%) |
| Neither agree nor disagree | 27 (19.7%) |
| Disagree | 27 (19.7%) |
| Strongly disagree | 10 (7.3%) |
| Not applicable/Don't know | 1 (0.7%) |
| My patients get enough counselling from their pharmacist about oral health | |
| Strongly agree | 2 (1.5%) |
| Agree | 18 (13.1%) |
| Neither agree nor disagree | 39 (28.5%) |
| Disagree | 55 (40.1%) |
| Strongly disagree | 16 (11.7%) |
| Not applicable/Don't know | 7 (5.1%) |
A higher mean self-confidence in prescribing and a higher mean confidence in pharmacists were found in dentists who did not specialize in periodontics compared to those who did (28.03 vs. 23.96 and 9.84 vs. 8.51, respectively) ( Table 5 ).
Table 5. Bivariate analyses of factors associated with the dentist's self-confidence in prescribing drugs and the confidence in pharmacists indexes
| Variable | Dentist's self-confidence in prescribing drugs | Dentist's confidence in pharmacists | ||
|---|---|---|---|---|
| Mean (SD) | p-value | Mean (SD) | p-value | |
| Gender | 0.753 | 0.744 | ||
| Male | 26.85 (6.88) | 9.35 (2.29) | ||
| Female | 26.46 (7.37) | 9.48 (2.54) | ||
| Educational level | 0.164 | 0.617 | ||
| Doctor in dentistry | 27.58 (8.39) | 9.67 (2.40) | ||
| Master's degree | 26.58 (5.54) | 9.27 (2.52) | ||
| PhD | 26.73 (7.46) | 8.73 (2.57) | ||
| Other degrees | 22.36 (3.93) | 9.27 (1.27) | ||
| Academia/Teaching | 0.070 | 0.792 | ||
| No | 27.86 (6.53) | 9.34 (2.47) | ||
| Yes | 25.67 (7.38) | 9.45 (2.33) | ||
| Periodontics | <0.001 | 0.002 | ||
| No | 28.03 (7.53) | 9.84 (2.35) | ||
| Yes | 23.96 (5.03) | 8.51 (2.23) | ||
| Endodontics | 0.308 | 0.231 | ||
| No | 26.40 (6.88) | 9.29 (2.45) | ||
| Yes | 28.00 (7.82) | 9.92 (2.06) | ||
| Oral and maxillofacial surgery | 0.058 | 0.385 | ||
| No | 26.31 (7.04) | 9.34 (2.35) | ||
| Yes | 30.07 (6.47) | 9.93 (2.73) | ||
| Pediatric dentistry | 0.330 | 0.682 | ||
| No | 26.88 (7.04) | 9.37 (2.32) | ||
| Yes | 25.07 (7.28) | 9.71 (3.02) | ||
| Oral and maxillofacial pathology | 0.485 | 0.683 | ||
| No | 26.57 (6.99) | 9.38 (2.38) | ||
| Yes | 28.20 (8.18) | 9.70 (2.54) | ||
| Orthodontics | 0.258 | 0.358 | ||
| No | 26.88 (6.95) | 9.35 (2.42) | ||
| Yes | 24.11 (8.48) | 10.11 (1.83) | ||
| Years of practice | 0.158 | 0.765 | ||
| Up to 3 years | 28.40 (5.45) | 9.66 (2.55) | ||
| More than 3 years and less than 12 years | 27.33 (7.04) | 9.29 (2.39) | ||
| 12 years or more | 25.73 (7.59) | 9.32 (2.33) | ||
The results of a first logistic regression, taking the dichotomous dentist's self-confidence in prescribing drugs score as the dependent variable, showed that specializing in periodontics was significantly associated with lower odds of having self-confidence in prescribing drugs (aOR=0.25) and having confidence in the pharmacist (aOR=0.45) ( Table 6 ).
Table 6. Multivariable analysis
| Variable | p-value | aOR | 95%CI | ||
|---|---|---|---|---|---|
| Model 1: Dichotomous dentist's self-confidence in prescribing drugs score as the dependent variable. Variables entered in the model: education level, specialty in periodontics, specialty in oral/maxillofacial surgery, Years of practice, age, involvement in academia teaching. | |||||
| Specialty in periodontics (yes vs. no*) | <0.001 | 0.25 | 0.12 | 0.54 | |
| Model 2: Dichotomous dentist's confidence in pharmacists score as the dependent variable. Variables entered in the model: specialty in periodontics, age, involvement in academia teaching. | |||||
| Specialty in periodontics (yes vs. no*) | 0.031 | 0.45 | 0.22 | 0.93 | |
DISCUSSION
This study assessed dentists' perception, practice, and confidence in prescribing drugs. Almost all participants considered they had fair to good perceived knowledge in pharmacology and therapeutics, but very few thought they had sufficient training to prescribe medications safely. This discrepancy might be related to the misleading information they might be getting from different sources. Indeed, in our study, pharmaceutical companies and medical representatives ranked first as sources of information on medications. Previous reports from Lebanon had highlighted the influence the pharmaceutical industry has on medical education activities, probably to promote a culture of acceptance. 11 However, dentists should not forget that the pharmaceutical industry can influence prescribing habits, sometimes leading to less rational and lower quality prescribing, with higher prescribing costs and risks since harmful effects of drugs are often missing in the promotional presentations. 11 , 17 This "bioethical" perspective on drug promotion should be implemented at the undergraduate level, and practitioners should be encouraged to seek information from more reliable sources. 11 Another explanation of this discrepancy could be related to the lack of training on translating pharmacological knowledge into clinical practice. A recent study exploring the effect of a multimodal intervention on prescribing practices showed that targeted education and the use of educational prescribing websites would improve knowledge and confidence among practitioners. 18 Such an approach, along with the integration of more pharmacology courses in the dental curriculum, as suggested by the vast majority of our sample, would enhance their trust in drug prescription, particularly in antibiotics and analgesics, the most reported prescribed drugs in our study.
Regarding antibiotics, the lack of confidence and low perceived knowledge identified in our study was similar to previous national and international findings in terms of adherence to antibiotic stewardship. 3 , 13 , 14 , 19 The lowest level of confidence among dentists specialized in periodontics was also described previously. 7
Inappropriate antibiotic prescriptions can lead to detrimental consequences, such as increased resistance, development of multidrug-resistant organisms, waste in healthcare resources and expenditures, and a higher number of adverse events, including the emergence of C. difficile . 3 , 14 Unfortunately, in Lebanon, national guidelines for antibiotic prescription in dentistry are lacking, and the National Antibiotic Resistance Committee at the Ministry of Public Health failed at establishing a clear strategic plan to curb antibiotic resistance. 14 Moreover, this committee does not include dental care practitioners among its members. Therefore, in such a complex environment, educational interventions (whether at the pre-graduate or post-graduate levels) are crucial to help dentists understand and apply the latest guidelines to improve antibiotic selection practices. 3 , 20 - 22
As for analgesics, while pain management is essential in dental practice, dentists, periodontists, in particular, should be aware of the risks of opioid misuse and abuse. Indeed, implants and periodontal procedures were among the four dental procedures that require the highest doses of opioids after adjusting for patients' characteristics. 7 Periodontists should know when to use them in case of persistent or severe pain or look for other therapeutic options, such as non-narcotic analgesics recommended as a first-line treatment, with guidelines agreeing on their better safety and efficacy than opioids. 7 , 23 , 24 Specific data on opioid abuse/misuse related to dental prescription lacks in Lebanon. However, acknowledging their inherent risks, weak opioids such as codeine and tramadol were classified as controlled drugs and cannot be dispensed by pharmacists without a doctor's prescription, including dentists. 25 , 26 Despite this restriction in Lebanon, local data from a pharmacist's perspective expressed the need for better supervision on sales and better governmental regulations to limit possible misuse or abuse. 26 In addition to opioids, clinicians should acknowledge the toxicity of NSAIDs and their potential interactions and adverse effects, especially that, in Lebanon, these medications are available over-the-counter. Therefore, dentists should advise their patients to avoid self-medication and should be extremely cautious when prescribing this class of analgesics in older patients, in patients with gastrointestinal problems, or taking aspirin, oral anticoagulants (vitamin K antagonists), or corticosteroids, due to the risk of gastric bleeding and peptic ulcer disease. 4 , 9
Besides the specific drug classes, dentists exhibited low perceived knowledge about prescribing in elderly patients, dosing, medication use in pregnancy, drug interactions, and adverse reactions. Moreover, their confidence in prescribing was the lowest in patients with organ impairment, cancer, and neurological disorders. This point is problematic, as several physiological changes can occur, whether in pharmacokinetics or pharmacodynamics of drugs, in these specific populations, with complex medical conditions and taking multiple medications. 4 , 27 A study using the Beers criteria to identify potentially age-inappropriate medications among elderly dental patients had found that 56.9% of prescriptions had at least 1 Beers Criteria medication, and 28.3% involved two or more Beers Criteria medications, including drugs negatively affecting patient safety and oral health care. 4
Drug-induced oral adverse effects are manifold and include xerostomia (opioids, anticholinergic antidepressants, first-generation anti-histamine, benzodiazepine), taste alteration (amitriptyline, aripiprazole, olanzapine, quetiapine), bruxism (quetiapine and paroxetine), gingival overgrowth (nifedipine and phenytoin), higher risk of bleeding (oral anticoagulants), and osteonecrosis of the jaw (bisphosphonates, denosumab, antiangiogenic agents). 10 , 28 , 29 In our study, the majority of participants admitted spending no more than 5-10 minutes to prescribe/explain a drug regimen, a relatively short time to also check for drug interactions with medications the patient is taking.
Collaboration with pharmacists and implications for practice
Our study finally assessed the relationship between dentists and pharmacists. While 61% considered that pharmacists should provide advice regarding oral care, only half of them encouraged their patients to talk to their pharmacists about their medications. Interestingly, only 15% considered that patients are getting enough counseling from the pharmacist, and the global index of dentist's confidence in pharmacists is below the median value, especially for periodontists who exhibited the lowest confidence in pharmacists. All these results suggest a reticence felt by both professions regarding collaboration and the need to be more open to this perspective. 30 Partnership with pharmacists would improve prescribing practices, whether in a shared space or at a community level. Joint seminars, congresses, and interdisciplinary meetings will foster professional relationships and improve patient care and prescribing skills. Implementing innovative learning techniques in a dental curriculum, such as interactive sessions with pharmacists, can be a good alternative. 31 , 32
Such interprofessional education would promote communication between professionals while helping students to manage medication allergies, interactions, and adverse effects. In that context, the Saint-Joseph University of Beirut added interactive pharmacology sessions to the pathology modules, provided the dental care center with a drug interaction checker, and trained dental students on how to handle the most frequently encountered drug prescription issues and communicate with the physician or the pharmacist.
Limitations and strengths
Our study has some limitations, particularly related to the small sample size. Selection bias is possible due to the low number of questionnaires returned, and we couldn't calculate the exact response rate since the snowball technique was used for data collection. Information bias is possible due to the potential misunderstanding of questions, the non-use of validated scales, or the inclusion of specialists who do not use prescriptions as others, such as orthodontists or public health dentists. Further validation of the suggested indexes is warranted to confirm our findings. Additionally, although we conducted a multivariable analysis, residual confounding cannot be ruled out since we could not assess all potential confounders, such as the university of graduation, continuing education related to pharmacology, and other factors not measured. Finally, the described patterns among dentists may not be representative of all dental practices in the country; further studies with larger samples using validated scales are warranted to confirm our results.
Nevertheless, to the best of our knowledge, this study is the first to evaluate the drug-prescribing perception and practice among dentists; it has a hypothesis-generating potential for both research and education fields.
CONCLUSIONS
Lebanese dentists reported some lack of knowledge and confidence in prescribing, particularly to specific populations. Education, training, and close collaboration between pharmacists and dental healthcare professionals are essential to overcome these problems and avoid potentially harmful effects due to prescribing errors, medication misuse, or drug interactions.

