










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkThe World Health Organization recognizes suicide as a major public health challenge (WHO, 2014). The latest figures estimate that there are around 800,000 suicide deaths worldwide each year: 1 every 40 seconds (WHO, 2021). In Spain, the Instituto Nacional de Estadística - i.e., the Spanish Statistical Office - reported 3,671 deaths by suicide in 2019, the leading external cause of death (INE, 2019). The statewide rate was 7.79 per 100,000 population, 12 in males and 3.75 in females. These data translate into an average of 10 suicides per day, 1 every 2.5 hours, and a sex distribution of 3:1 male/female.
In addition, reports issued during the pandemic period stated that 2020 was the year with the highest number of suicides recorded in the history of Spain since records began in 1906 (INE, 2020). Thus, 3,941 people took their own lives, 74.3% male, an increase of 7.4% over 2019. The national average reached 11 suicides per day. Women exceeded 1,000 deaths annually for the first time. Among the record highs, this phenomenon became the leading cause of death in young people aged 15-29 with 300 deaths (75.7% male), second only to tumor diseases. Added to this figure are 14 premature suicides in children under 15 years of age, 50% male/female.
In this scenario, it is worth noting that death by suicide is the last link in a chain of thoughts and behaviors of increasing severity and lethal intent: the suicide spectrum. It is a multidimensional construct whose phenotypic manifestation encompasses suicidal ideation, planning, communication, and acting (Anseán, 2014; O'Connor & Nock, 2014). Under this conceptualization, suicide risk would be determined by the conjunction of the type of suicidal indicator and its level of intensity, frequency, and functional interference (O'Connor & Pirkirs, 2016).
Recent studies provided epidemiological data on the suicide spectrum, focusing on Spanish adolescents as a target population. Thus, Fonseca-Pedrero et al. (2020) assessed the presence of suicide indicators among 3,454 adolescents aged 14-19 years. 26.7% stated that life was not worth living, 18.7% experienced death wishes, 17.8% thought about taking their own life, 5.9% acknowledged having a suicide plan, and 3.7% admitted to previous suicide attempts. Women obtained higher rates than men with a small effect size. Similarly, Miranda-Mendizabal et al. (2019) identified a higher number of suicide attempts in women and deaths in men, a divergence commonly associated with the lethality of the suicide method (Navarro-Gómez, 2017).
However, sex as a socio-demographic component is not the only influencing factor. Multiple biological, psychological, social, and environmental variables converge and interact in the complex etiology of suicide (Klonsky et al., 2016). Consequently, the conceptual delineation, assessment, treatment, and prevention of suicide require a holistic approach capable of integrating diverse sources of evidence, even when there are clinical and research discrepancies (O'Connor & Pirkis, 2016). Therefore, reliable detection of possible cases with high suicide risk is imperative for early preventive intervention (Díez-Gómez et al., 2020).
In this regard, numerous measures of suicidality are available based mostly on self-report techniques (Batterham et al., 2015), which quasi-inherently have social desirability, simulation, and response tendency biases that threaten their utility, validity, and reliability (Kimberlin & Winterstein, 2008). Nevertheless, the recent study by Nock et al. (2022) concludes that the combined use of self-report and electronic health records in psychiatric patients improves the prediction of suicide attempts during the subsequent 6 months. Thus, despite the shortcomings referred to above, the self-administered method is a useful form of clinical measurement. Knowing the sources of bias makes it possible to anticipate its occurrence and reduce its impact on the assessment of the psychological construct since it is not a systematic event (Louzán-Mariño, 2020).
Furthermore, previous research indicates that 75% of psychiatric patients who died by suicide denied experiencing suicidal tendencies the last time they were asked these questions by a health professional using dichotomous categories (no/yes) (Harmer et al., 2021). At this point, it is worth remembering that a large percentage of instruments traditionally used in the field of suicidology initially present such a dichotomous scale as a screening, which is translated in terms of the absence-presence of the suicide indicator; for instance, the Columbia-Suicide Severity Rating Scale (Posner et al., 2011), Self-Injurious Thoughts and Behaviors Interview (Nock et al., 2007) or Mini International Neuropsychiatric Interview for Suicidality Disorders (Sheehan & Giddens, 2016), among others.
The sensitive and stigmatized nature of suicide requires a particular assessing approach to prevent underestimation through false negatives. Thus, recent studies have included a third alternative in their self-report protocol, "prefer not to say", to identify cases with covert suicidal risk among representative samples of war veterans (Stanley et al., 2022), emergency personnel (Kyron et al., 2020) and university students (Podlogar et al., 2016). In unison, the findings reveal symmetrical profiles in the disposition of risk and protective factors between groups of participants who stated experiencing suicidal ideation and behavior and groups who prefer not to answer.
Based on the literature described, it is considered that the selection of this type of response could be motivated by a double casuistry. Choosing "prefer not to say" could derive from a self-report response bias, or from a passive way of stating suicidality that, to the best of our knowledge, has not yet been explored in the adolescent community population. Consequently, the main aim of this study was to examine the self-reported presence of suicide spectrum indicators in a sample of Spanish adolescents, using a trichotomous response scale: no, yes, and prefer not to say. As specific objectives: a) determine the retrospective and current prevalence of suicidal thoughts and behavior; b) identify the age of onset; c) analyze the socio-demographic correlates; and d) explore the clinical implications of the trichotomous response scale by comparing the level of socioemotional strength, psychopathology and subjective well-being among adolescents.
Method
Participants
The non-probabilistic quota sampling technique was applied. The target universe (u) comprised 243,944 adolescents aged 12-18 (51.44% male), residing in two areas of southeastern Spain: Province of Alicante (u = 128,029; 51.49% male) and Region of Murcia (u = 115,915; 51.38% male) (INE, 2017). The stratification considered the representativeness of the geographical area: 9 and 21 comarcas in Alicante and Murcia, respectively. The probability of school selection was determined based on equity between the universe, the number of schools, ownership (70% public, 30% private or concerted), affiliation (15% Catholic, 85% non-denominational), and the number of students per school in each county.
Accordingly, the management and guidance teams of 100 secondary schools were contacted. This procedure showed a clear refusal on the part of the educational community to deal with suicide in the classroom. 48% declined to participate for this reason, while 18% cited organizational issues and lack of material resources. Initial recruitment reached a total of 5,741 students in Compulsory Secondary Education, Baccalaureate, and Vocational Training, according to the Spanish education system. 213 cases (3.7%) were excluded due to incomplete surveys. Thus, the final sample was composed of 5,528 adolescents aged 12-18 (M ± SD = 14.20 ± 1.53), 50.74% female, representing 2.27% of the target universe (Table 1).
Table 1. Socio-demographic data
| Variables | n | % | |
|---|---|---|---|
| Sex | Females | 2,805 | 50.74 |
| Males | 2,723 | 49.26 | |
| Age | 12 | 754 | 13.64 |
| 13 | 1,335 | 24.15 | |
| 14 | 1,226 | 22.18 | |
| 15 | 1,055 | 19.08 | |
| 16 | 739 | 13.37 | |
| 17 | 279 | 5.05 | |
| 18 | 140 | 2.53 | |
| Location | Province of Alicante | 2,224 | 40.23 |
| Region of Murcia | 3,304 | 59.77 | |
| Ownership | Public | 3,597 | 65.07 |
| Concerted | 1,623 | 29.36 | |
| Private | 308 | 5.57 | |
| Affiliation | Lay / Non-denominational | 4,802 | 86.87 |
| Catholic | 726 | 13.13 |
Note. n = 5,528.
Instruments
Self-Injurious Thoughts and Behaviors Interview (SITBI) (Nock et al., 2007) and Columbia-Suicide Severity Rating Scale (C-SSRS) (Posner et al., 2011). A selection of items from the Spanish version of the SITBI (García-Nieto et al., 2013) and the C-SSRS (Al-Halabí et al., 2016) was administered for the assessment of 5 indicators of the suicide spectrum in self-report mode, which is accurate in Spanish university students (Blasco et al., 2016). These indicators are death wishes, suicidal ideation, determination of a method of suicide, design of a detailed suicide plan, and previous suicide attempt. The items examine their lifetime occurrence and last 12 months using a dichotomous response scale: no/yes. If yes, data are collected on the age of onset of each self-reported suicide marker, allowing a numerical value of up to 18 years to be entered. Further, a third alternative response, “prefer not to say”, was included in this study due to the sensitive nature of the information examined and to analyze its clinical nature.
Social Emotional Health Survey - Secondary (SEHS-S) (Furlong et al., 2014; Spanish version by Piqueras et al., 2019). It is a 36-item instrument designed to measure positive intra- and interpersonal self-schemas in adolescents, that presents a 4-point Likert scale according to the degree of identification with the statements (1 = Not at all true; 4 = Totally true). For this study, the overall score was used as an informant for the level of socioemotional strength or covitality (Cronbach's α = .91; McDonald's ꞷ = .91).
Pediatric Symptom Checklist - Youth Self-Report (PSC-17-Y) (Gardner et al., 1999; Spanish version by Piqueras et al., 2021). This instrument allows the screening of psychosocial problems in adolescents: internalizing, externalizing, and inattention-hyperactivity symptoms. It consists of 17 items and a 3-point Likert scale to indicate the frequency of occurrence of each psychopathological manifestation (0 = Never, 1 = Sometimes, 2 = Often). The total score was used as a report of the degree of psychopathology (Cronbach's α = .81; McDonald's ꞷ = .81).
Mental Health Continuum - Short Form (MHC-SF) (Keyes et al., 2008; Spanish version by Piqueras et al., 2022). This measure provides a multidimensional assessment of subjective well-being: emotional, psychological, and social. It is composed of 14 items and 6 response alternatives, reflecting the frequency of experiencing symptoms formulated positively (1=Never; 6=Always). For this study, the overall score was considered an indicator of the degree of subjective well-being (Cronbach's α = .92; McDonald's ꞷ = .93).
Procedure
This study presents an empirical design as follows a quantitative, observational, descriptive-correlational, and multicentric methodology (Montero & León, 2007). It is framed within a 2017 R+D+i project (PSI2017-88280-R) that has institutional approval at an ethical and legal level by the Office of Responsible Research of the Project Evaluation Body of the Miguel Hernández University of Elche (DPS.JPR.02.17).
After agreeing to collaborate with 34 secondary schools, the team of teachers disseminated the information material about the research project to parents - or legal guardians - and adolescents. Besides, they led the delivery and collection of informed consent forms for both collectives. Participation in the study required the fulfillment of 2 inclusion criteria: 1) providing double authorization or consent; and 2) presenting an optimal level of understanding of the Spanish language. Thus, the sample retention rate reached 85%. The assessment protocol was completed using the LimeSurvey© web platform on the school's premises, in groups, during school hours, and in an average time of 30 minutes.
Data collection took place between October 2018 and January 2019 and was supervised on-site by specialists in child and adolescent psychological treatment. Subsequently, the centers received a descriptive report of the results, that pretended to provide a general overview of mental health status, which served as a basis for the development of Tutorial Action Plans. A report was also issued to the Autonomous Secretariat for Education and Research of the Regional Ministry of Education, Research, Culture and Sport of Generalitat Valenciana, and to the Directorate General for Attention to Diversity and Educational Quality of the Regional Ministry of Education, Youth and Sport of Region of Murcia.
During the process, voluntariness, pseudo-anonymity, and confidentiality of the data were ensured, with a warning that the data would be used exclusively for research and suicide prevention purposes. An identification code was assigned to each participant whose correspondence with personal data was kept by the educational centers, in compliance with Spanish Organic Law 3/2018, 5 December, on Personal Data Protection and guarantees of digital rights (Cortes Generales de España, 2018).
The current legal, ethical, and deontological regulations on the detection and early care of minors at risk of suicide led to the adoption of a protocol for coordinated actions, and an interdisciplinary approach, between the management of the centers, parents or legal guardians, Regional Ministers of Education, Educational Therapeutic Units and research team. These actions were intended, as stipulated, to ensure the physical and psychological integrity of minors (Consejo General de Colegios Oficiales de Psicólogos de España, 2010; Conselleria de Educación, Investigación, Cultura y Deporte & Conselleria de Sanidad Universal y Salud Pública, 2017; Consejería de Educación, Juventud y Deportes de la Región de Murcia, 2017; Cortes Generales de España, 2021).
Data Analyses
Data processing was performed using IBM® SPSS® Statistics 27 software ( IBM Corp. Released, 2020), assuming statistical significance at p < .001 or 99% confidence interval (Allen & Bennett, 2008). Previously, reliability (Cronbach's Alpha and McDonald's Omega: > .70) and factorial invariance by sex and age of the measures were estimated for this sample. Since it was not the subject of the study, the results are available upon request. Preliminary cleaning of missing values was not necessary, as the software configuration of the online survey presented a mandatory response system that prevented the recording of blank items.
First, descriptive statistics and frequencies were calculated to determine the retrospective prevalence of each suicide spectrum indicator - i.e., no, yes, and prefer not to say -, to identify the age of onset, and to examine its manifestation during the last year. Hereafter suicidality reported will be referred to in terms of absence and presence of the indicator, and omission of response, respectively. To test for homogeneity in the distribution of frequencies by sex (male and female) and age (12-13, 14-15, and 16-18 years old), contingency tables were calculated, and the chi-square (χ 2 ) and Cramér's V statistics were informed. The magnitude of the V association was interpreted as a function of the degrees of freedom (df) between both nominal variables: a) 2 df for the association between sex and suicidality reported (2x3 analysis matrix): ≈ .07 weak, ≈ .21 medium, and ≈ .35 strong, and b) 4 df for the relation between age groups and suicidality reported (3x3 analysis matrix): ≈ .05 weak, ≈ .15 medium and ≈ .25 strong (Domínguez-Lara, 2018).
Second, a three-way ANOVA was conducted to analyze differences in levels of covitality, psychopathology, and subjective well-being - dependent variables entered in autonomous models - between the grouping of participants according to the current suicidality reported, sex, and age - fixed factors introduced in a single block -, and to investigate interaction effects (3x2x3 analysis matrix). The partial eta squared statistic (ηp 2 ) was used to calculate the effect size for intragroup differences of the fixed factors, thus determining the clinical relevance of the results: ≈ .01 small, ≈ .06 medium, and ≈ .14 large (Cohen, 1973).
Finally, post hoc tests based on the parametric HSD Tukey criterion were conducted to establish differences in covitality, psychopathology, and subjective well-being between groups of participants classified according to the suicidality reported. Cohen's d was used as a statistic for the magnitude of these differences: ≈ .20 small, ≈ .50 medium, and ≈ .80 large (Cohen, 1988). Further, marginal means and confidence intervals of adolescents with presence, absence, and omission of suicidal markers were estimated on bidimensional mental health and covitality indices. These data were illustrated using scatter plots.
Results
Let's Talk About Suicide Spectrum in Spanish Adolescents
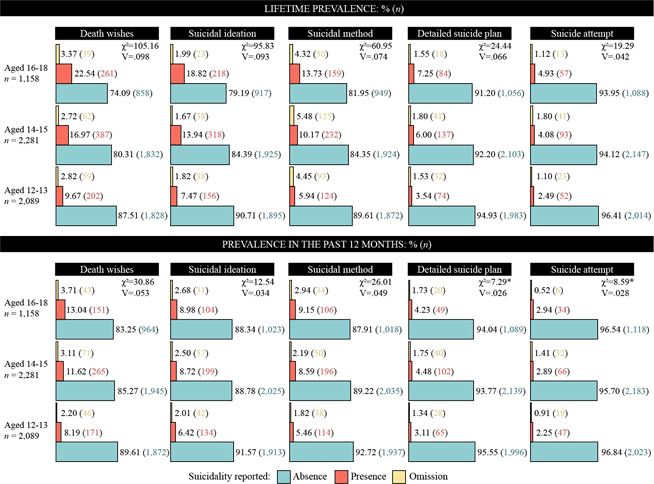
The lifetime prevalence of the suicide spectrum reached 15.38% for ideation, 9.32% for planning, and 3.65% for attempts; while the prevalence in the last year had values of up to 10.62%, 7.53%, and 2.66%, respectively (Figure 1). The age of onset of suicidal thoughts and behavior was mostly around 12 years old [M ± SD]: death wishes, 12.03 ± 2.04; suicidal ideation, 12.26 ± 2.16; choice of suicide method, 12.31 ± 2.01; devising a detailed suicide plan, 12.31 ± 1.94; and previous suicide attempts, 12.37 ± 1.82.

Note. % (n). V: ≈ .07 weak, ≈ .21 medium, and ≈ .35 strong. Significance level: p < .001
Figure 1. Prevalence of the Suicide Spectrum: sex differences
Analysis of sex differences revealed that women significantly doubled the figures of men on all suicide indicators, irrespective of time frame. Omission of response showed the same comparative trend, finding that women tripled the rates of men. In this sense, it should be noted that the association between the nominal variables sex and suicidality reported was significant in all combinations, but of weak to medium magnitude.
Concerning age differences in suicide indicators, lifetime prevalence showed a significant trend to increase their presence, in percentage terms, from younger to older age groups (see Figure 2). Participants aged 14 to 15 years doubled the report of suicidal ideation and behavior compared to those aged 12 to 13 years; while adolescents aged 16 to 18 years had slightly higher prevalence values than the middle-aged group, especially in death wishes and suicidal ideation. The current prevalence of suicidal markers also showed a tendency to increase towards older ages, although to a lesser extent. No differences were observed in the omission of response. Again, the association between the nominal variables age and suicidality reported was significant in most comparisons, but of weak magnitude.
“Prefer not to say”: Missing Value or Clinical Data?
The three-way ANOVA provided homogeneous results for the three dependent variables analyzed in autonomous models: covitality, psychopathology, and subjective well-being (Table 2). A statistically and clinically significant effect was only found for the variable of grouping participants by suicidality reported - i.e., presence, absence, and omission - with a medium to a large magnitude. This effect was observed for all dimensions of the suicide spectrum and all dependent variables. Sex had no influence in any model tested and age was significant for covitality with a negligible effect. No interaction effects were obtained from the possible combinations of the three fixed factors.
Table 2. Three-way ANOVA for the Covitality, Psychopathology, and Subjective Well-Being indices
| Effects | df | Covitality | Psychopathology | Subjective Well-Being | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p | ηp 2 | F | p | ηp 2 | F | p | ηp 2 | |||
| Death wishes | Suicidality reported | 2 | 287.44 | <.001 | .094 | 392.55 | <.001 | .126 | 415.26 | <.001 | .131 |
| Sex | 1 | .01 | .972 | <.001 | .42 | .517 | <.001 | .22 | .643 | <.001 | |
| Age | 2 | 7.06 | <.001 | .003 | 5.68 | .003 | .002 | 2.62 | .073 | .001 | |
| SR*Sex | 2 | .23 | .797 | <.001 | 1.96 | .142 | .001 | .35 | .706 | <.001 | |
| SR*Age | 4 | 1.29 | .272 | .001 | 1.82 | .123 | .001 | .76 | .552 | .001 | |
| Sex*Age | 2 | .02 | .976 | <.001 | 1.28 | .279 | <.001 | .19 | .827 | <.001 | |
| SR*Sex*Age | 4 | .47 | .761 | <.001 | .86 | .485 | .001 | 1.42 | .223 | .001 | |
| Suicidal ideation | Suicidality reported | 2 | 237.11 | <.001 | .079 | 321.27 | <.001 | .105 | 362.67 | <.001 | .116 |
| Sex | 1 | .90 | .344 | <.001 | .12 | .734 | <.001 | .49 | .483 | <.001 | |
| Age | 2 | 9.42 | <.001 | .003 | 3.96 | .019 | .001 | 6.20 | .002 | .002 | |
| SR*Sex | 2 | .10 | .907 | <.001 | 2.71 | .067 | .001 | .08 | .927 | <.001 | |
| SR*Age | 4 | .52 | .724 | <.001 | 3.65 | .006 | .003 | .61 | .659 | <.001 | |
| Sex*Age | 2 | .06 | .939 | <.001 | 1.92 | .147 | .001 | .94 | .389 | <.001 | |
| SR*Sex*Age | 4 | 3.28 | .011 | .002 | 3.31 | .010 | .002 | 5.13 | .002 | .002 | |
| Suicide method | Suicidality reported | 2 | 199.18 | <.001 | .067 | 320.22 | <.001 | .105 | 319.17 | <.001 | .104 |
| Sex | 1 | 2.47 | .116 | <.001 | .31 | .578 | <.001 | .93 | .334 | <.001 | |
| Age | 2 | 7.78 | <.001 | .003 | 2.17 | .114 | .001 | 1.64 | .194 | .001 | |
| SR*Sex | 2 | .26 | .773 | <.001 | 1.10 | .335 | <.001 | .68 | .504 | <.001 | |
| SR*Age | 4 | .54 | .709 | <.001 | 3.75 | .005 | .003 | .79 | .532 | .001 | |
| Sex*Age | 2 | 1.59 | .205 | .001 | .16 | .851 | <.001 | .35 | .705 | <.001 | |
| SR*Sex*Age | 4 | 2.46 | .043 | .002 | 2.02 | .089 | .001 | 2.35 | .052 | .002 | |
| Detailed suicide plan | Suicidality reported | 2 | 134.12 | <.001 | .046 | 195.80 | <.001 | .067 | 219.81 | <.001 | .074 |
| Sex | 1 | 1.11 | .293 | <.001 | 1.27 | .260 | <.001 | 7.24 | .979 | <.001 | |
| Age | 2 | 4.05 | .017 | .001 | .97 | .378 | <.001 | 3.43 | .033 | .001 | |
| SR*Sex | 2 | .07 | .935 | <.001 | .52 | .596 | <.001 | .53 | .590 | <.001 | |
| SR*Age | 4 | 1.32 | .261 | .001 | 2.53 | .038 | .002 | .26 | .907 | <.001 | |
| Sex*Age | 2 | .87 | .420 | <.001 | 2.33 | .098 | .001 | 3.12 | .044 | .001 | |
| SR*Sex*Age | 4 | 1.50 | .198 | .001 | 2.42 | .046 | .002 | 3.18 | .013 | .002 | |
| Suicide attempt | Suicidality reported | 2 | 87.66 | <.001 | .031 | 136.39 | <.001 | .048 | 160.40 | <.001 | .055 |
| Sex | 1 | .93 | .334 | <.001 | .01 | .910 | <.001 | 1.93 | .165 | <.001 | |
| Age | 2 | .53 | .591 | <.001 | .10 | .908 | <.001 | .43 | .650 | <.001 | |
| SR*Sex | 2 | 1.51 | .222 | .001 | 3.96 | .019 | .001 | 2.50 | .083 | .001 | |
| SR*Age | 4 | 1.96 | .098 | .001 | 2.79 | .025 | .002 | .68 | .609 | <.001 | |
| Sex*Age | 2 | 1.38 | .251 | .001 | .47 | .625 | <.001 | .85 | .428 | <.001 | |
| SR*Sex*Age | 4 | 1.33 | .257 | .001 | 1.45 | .216 | .001 | 1.00 | .408 | .001 |
Nota. Suicidality reported (SR): absence, presence, and omission. Sex: females and males. Age: 12-13, 14-15, and 16-18 years old. Effect size of partial eta squared (ηp 2 ): ≈ .01 small, ≈ .06 medium, and ≈ .14 large. Significance level: p < .001.
Consequently, the results of the post hoc tests determined that statistically and clinically relevant differences were between participants with presence and omission, versus participants with an absence of suicidal ideation and/or behavior during the past year (Table 3). Once again, statistical significance was found for all indicators of the suicide spectrum and all dependent variables. The effect size was large in all cases (> .95). It should be noted that statistical significance was not reached in the comparison between participants with the presence of suicidal tendencies and “prefer not to say” responders.
Table 3. Post-hoc contrasts: differences in Covitality, Psychopathology, and Subjective Well-being according to Suicidality reported
| Suicidality reported | Covitality | Psychopathology | Subjective Well-Being | vs. | Covitality | Psychopathology | Subjective Well-Being | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | PTukey | CI | d | PTukey | CI | d | PTukey | CI | d | |||
| Death wishes | 1. Absence | 3.14 ± .37 | .56 ± .28 | 4.59 ± .84 | 1-2 | <.001 | .35, .46 | 1.05 | <.001 | -.40, -.31 | 1.28 | <.001 | .95, 1.22 | 1.23 |
| 2. Presence | 2.74 ± .40 | .91 ± .27 | 3.51 ± .93 | 1-3 | <.001 | .29, .51 | .95 | <.001 | -.39, -.23 | 1.09 | <.001 | .81, 1.29 | 1.19 | |
| 3. Omission | 2.75 ± .46 | .86 ± .28 | 3.54 ± .92 | 2-3 | .985 | -.13, .11 | .01 | .154 | -.04, .14 | .16 | .878 | -.31, .23 | .04 | |
| ideation | 1. Absence | 3.14 ± .38 | .57 ± .29 | 4.56 ± .85 | 1-2 | <.001 | .34, .48 | 1.05 | <.001 | -.41, -.31 | 1.29 | <.001 | 1.01, 1.31 | 1.31 |
| 2. Presence | 2.73 ± .40 | .93 ± .27 | 3.40 ± .93 | 1-3 | <.001 | .31, .55 | 1.03 | <.001 | -.40, -.22 | 1.08 | <.001 | .81, 1.35 | 1.21 | |
| 3. Omission | 2.70 ± .46 | .88 ± .30 | 3.48 ± .94 | 2-3 | .795 | -.11, .16 | .06 | .198 | -.05, .15 | .17 | .624 | -.38, .23 | .08 | |
| Suicide method | 1. Absence | 3.14 ± .38 | .56 ± .28 | 4.56 ± .85 | 1-2 | <.001 | .31, .45 | .98 | <.001 | -.41, -.31 | 1.26 | <.001 | .94, 1.26 | 1.22 |
| 2. Presence | 2.80 ± .40 | .88 ± .29 | 3.63 ± .96 | 1-3 | <.001 | .32, .56 | 1.07 | <.001 | -.43, -.24 | 1.18 | <.001 | .80, 1.36 | 1.20 | |
| 3. Omission | 2.84 ± .41 | .80 ± .26 | 3.76 ± .89 | 2-3 | .276 | -.08, .20 | .14 | .714 | -.08, .13 | .08 | .968 | -.34, .30 | .02 | |
| Detailed suicide plan | 1. Absence | 3.12 ± .39 | .58 ± .29 | 4.52 ± .87 | 1-2 | <.001 | .33, .52 | 1.06 | <.001 | -.47, -.33 | 1.42 | <.001 | 1.05, 1.49 | 1.35 |
| 2. Presence | 2.72 ± .40 | .96 ± .28 | 3.36 ± .99 | 1-3 | <.001 | .31, .60 | 1.13 | <.001 | -.45, -.23 | 1.16 | <.001 | .76, 1.43 | 1.20 | |
| 3. Omission | 2.72 ± .42 | .87 ± .28 | 3.61 ± .89 | 2-3 | .763 | -.14, .21 | .08 | .183 | -.07, .19 | .23 | .258 | -.57, .22 | .18 | |
| Suicide attempt | 1. Absence | 3.11 ±.39 | .59 ± .30 | 4.50 ± .89 | 1-2 | <.001 | .33, .56 | 1.08 | <.001 | -.50, -.32 | 1.43 | <.001 | 1.11, 1.64 | 1.46 |
| 2. Presence | 2.75 ± .43 | .92 ± .28 | 3.34 ± .99 | 1-3 | <.001 | .26, .63 | 1.12 | <.001 | -.49, -.22 | 1.27 | <.001 | .73, 1.57 | 1.31 | |
| 3. Omission | 2.63 ± .37 | .94 ± .29 | 3.37 ± .82 | 2-3 | .984 | -.22, .22 | .01 | .423 | -.11, .22 | .21 | .236 | -.72, .27 | .24 |
Note. Rating anchor: Covitality 1-4, Psychopathology 0-2, Subjective Well-being 1-6. CI = 99% Confidence Intervals. d: ≈ .20 small, ≈ .50 medium, and ≈ .80 large. Significance level: p < .001.
Figure 3 illustrates that participants with an absence of suicidality had the highest estimated marginal means in socioemotional strength and subjective well-being, and the lowest in psychopathology. Participants with a presence of suicidal tendencies and/or omission of response reported very similar results: as the severity of the indicator on the suicide spectrum increased, so did their psychopathological symptoms, and their levels of covitality and subjective well-being decreased. At the same time, the width of the confidence intervals of these two groups increased, indicating greater variability in the psychological profiles.

Discussion
The purpose of the study was to examine the self-reported presence of suicide spectrum indicators among adolescents, using a trichotomous rating scale: no (absence), yes (presence), and prefer not to say (omission). Specific objectives are discussed considering the main findings.
Firstly, the manifestation of suicidal thoughts and behaviors was explored across a lifetime and during the last 12 months. To avoid dehumanizing the data of this research, the number of adolescents who reported each suicide indicator is cited rather than their statistical prevalence exclusively. Thus, alluding to lifetime occurrence, of the 5,528 adolescents 850 (15.38%) experienced death wishes, 692 (12.52%) thought about taking their own life, 515 (9.32%) chose a method of suicide, 295 (5.34%) devised a detailed suicide plan, and 202 (3.65%) attempted suicide previously. In addition, as many as 268 (4.85%) people opted not to respond. Shortening the time frame to the last year, the figures dropped modestly to 587 (10.62%), 437 (7.91%), 416 (7.53%), 216 (3.91%,) and 147 (2.66%) adolescents, respectively. These results are consistent with the prevalence reported in previous studies. Lim et al. (2019) collected publications on the subject between 1989 and 2018, grouping 686,672 individuals. Lifetime prevalence was 18% for suicide ideation, 9.9% for suicide planning, and 6% for suicide attempts; while past 12-month prevalence was 14.2%, 7.5%, and 4.5%, respectively. At the national scope, Fonseca-Pedrero et al. (2020) obtained figures of up to 17.8% for suicidal ideation, 5.9% for planning, and 3.7% for attempted suicide among 3,454 adolescents aged 14-19 years.
Secondly, an attempt was made to identify the age of onset of suicidal tendencies. The results were homogeneous across the diversity of suicidal indicators, placing the marker at 12 years old and an extended range from 10 to 14. In other words, early adolescence could be considered a critical period in the emergence of suicidality, as pointed out by previous authors (e.g., Alqueza, 2021; Solmi et al., 2022). Thus, it should be emphasized that this age of onset assumes an important precursor character on the severity of future suicidal thoughts and behavior, and consequently, on the risk of suicide in later developmental stages (Thompson et al., 2012).
Thirdly, socio-demographic correlates of the suicide phenomenon were analyzed. Women doubled and even tripled the prevalence rates of men on the presence of suicidality and the omission of response. Fonseca-Pedrero et al. (2020) found higher figures in women, although with a small effect size. Miranda-Mendizabal et al. (2019) identified more suicide attempts in women and more suicide deaths in men, as official sources continue to reflect (INE, 2020). In this way, the suicidal tendencies showed a differential pattern by sex that the literature links to variability in the arrangement and interaction of biological, psychological, and social elements (O'Connor & Nock, 2014; Turecki & Brent, 2016).
Additionally, suicidality reported showed a tendency to increase with age. Participants aged 14 years and older stated twice as many suicidal elements as those aged 12-13 years. Thereafter, the figures raised almost proportionally until they reach 18 years of age. Similarly, Voss et al. (2019) reported cumulative incidence estimates of suicidal ideation and behavior in adolescents, starting at age 10 (<1%), increasing slightly up to age 12 (2.2%), and rising sharply up to age 20 (13.5%).
Finally, the clinical implications of the use of the self-report with a trichotomous response scale in the assessment of suicidal risk were explored. Findings revealed that the group of adolescents with the presence of suicidal indicators and/or omission of response obtained, equivalently, lower levels of socioemotional strength and subjective well-being, and higher levels of psychopathology, compared to the group with the absence of markers. Prior studies already indicated differences between minors with the absence and presence of suicidality in terms of psychopathological symptoms (e.g., Soto-Sanz et al., 2019a), self-perceived emotional intelligence (e.g., Domínguez-García & Fernández-Berrocal, 2018) and subjective well-being (e.g., Fonseca-Pedrero et al., 2018). However, the response mode "prefer not to say" was, to the best of our knowledge, a pending issue to be explored in this collective. Such an alternative had been tested in other population samples, revealing similar psychological profiles between "yes" and "prefer not to say" responders to suicide markers (Kyron et al., 2020; Podlogar et al., 2016; Stanley et al., 2022). Kyron et al (2020) further qualified that this was associated with the perception of mental health stigma.
In short, the findings of this study support the hypothesis that "prefer not to say" could be a covert way of reporting suicidal risk, accordingly to previous research. However, the results should be interpreted with caution, as the gradual growth of the confidence intervals in synchrony with the severity of the suicide indicator denotes a plurality of psychological patterns in terms of psychopathology, covitality, and subjective well-being. This could mean that their selection would be motivated to a greater extent by the degree of suicidal tendency, but also by an inherent self-report bias in some isolated cases, which is an important limitation of the study. For this reason, it would be advisable to combine their use with specific validity scales (infrequency, acquiescence, social desirability or response tendency; e.g., Fonseca-Pedrero et al., 2009) and instruments aimed at the assessment of more specific biopsychosocial factors scientifically linked to suicidal risk; such as depressive symptomatology (e.g., Soto-Sanz et al., 2019a), self-esteem (e.g., Soto-Sanz et al., 2019b) or peer relationship problems (e.g., Barzilay et al., 2017), among others.
Added to this limitation is the latency between data collection in the pre-pandemic period and publication in article format. Reports issued after the emergence of the health crisis warn of an increase in deaths by suicide, reaching historical records among adolescents (INE, 2020). Therefore, it is considered that the exposed data may underestimate the magnitude of the suicide phenomenon in the current social and health care context. In any case, considering that the scientific community agrees that previous suicidal thoughts and behaviors are key predictors of subsequent suicide death (Castellví et al., 2017; Ribeiro et al., 2016), the figures provided seem especially alarming.
In summary, suicide is a complex, multifactorial and multidimensional phenomenon, which requires a holistic approach with special emphasis on preventive actions. WHO (2021) highlights the importance of identifying, assessing, managing, and monitoring people with suicidal ideation and/or behavior. In particular, early detection and care of adolescents with suicidal tendencies could be a very important part of successful intervention, given the great impact it confers on the course and prognosis of future suicide markers (Al-Halabí & Fonseca-Pedrero, 2021). To this end, the school is undoubtedly a natural context for potential screening (Díez et al., 2022) and with accumulated evidence on the speed and cost-effectiveness of its actions (O'Shea & McHayle, 2022).
Given the sensitive and stigmatized nature of suicide, it is imperative to dispose of reliable detection tools that prevent its underestimation and promote the early implementation of evidence-based psychological treatments: effective, efficient, and effective (Fonseca-Pedrero et al., 2021). Not from a nosologically perspective of suicide, as it is not a mental disorder in its own right, but from the perspective of a psychological phenomenon with serious social and health implications. The findings of this study suggest that the "prefer not to say" response alternative could increase the sensitivity of self-report in the field of suicidology, allowing for more accurate identification of cases at high risk of suicide that would go unnoticed by the traditional dichotomous response system.

