










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
versão On-line ISSN 2173-2345versão impressa ISSN 1889-836X
Rev Osteoporos Metab Miner vol.10 no.2 Madrid Abr./Jun. 2018 Epub 17-Maio-2021
https://dx.doi.org/10.4321/s1889-836x2018000200002
ORIGINALS
Osteoporotic hip fractures in older adults in Ecuador 2016
1Servicio de Endocrinología - Hospital Docente de la Policía Nacional Guayaquil Nº 2 - Guayaquil (Ecuador)
2Instituto de Biomedicina - Universidad Católica Santiago de Guayaquil - Guayaquil (Ecuador)
3Servicio de Medicina Interna - Hospital Docente de la Policía Nacional Guayaquil Nº 2 - Guayaquil (Ecuador)
4Servicio de Endocrinología - Omni Hospital - Guayaquil (Ecuador)
Objectives:
To ascertain the incidence of hip fractures in Ecuador in 2016, to determine whether there were variations according to geographic region, residence or season of the year.
Materials and methods:
Epidemiological, descriptive and retrospective study. The Hospital Discharges Yearbook of Ecuador was used to determine the number of people aged 60 or more hospitalized for hip fracture from January 1 to December 31, 2016. To calculate the incidence per 100,000 inhabitants/year, the Ecuadorian population projection of the Economic Commission for Latin America and the Caribbean (CEPAL) was used as a denominator for the year 2016. The incidence standardized by age was calculated by the direct method using 2 reference populations: 1) the one of 60 or more years for America Latina made by the Latin American and Caribbean Demographic Center (CELADE) in 2016; 2) with the population of Ecuador in 2010.
Results:
In total, 2,054 people were hospitalized with hip fracture diagnosis (1,470 women and 584 men) in 2016. The crude annual incidence was 123 cases per 100,000 inhabitants/year (74.6 per 100,000 men/year and 165.8 per 100,000 women/year). The age-adjusted incidence increased exponentially with age in both sexes. It was greater in women. The standardized incidence with with the population of Latin America was 165.4 and 80.1 per 100,000/year, in women and men respectively. In-hospital mortality was 5.1% and 3.8% in women and men, respectively.
Conclusions:
The incidence of hip fractures is greater in women than in men, there being an exponential increase with age, more evident after 80 years. There were no differences by geographical region. In comparison with developed countries and other Latin America countries, incidence of hip fractures was lowest in Ecuador.
Introduction
As life expectancy increases throughout the world, the number of older adults is growing in each geographic region. In Ecuador, the proportion of older adults (≥60) among the overall population rose from 7.2% in 2000 to 10.2% in 2016 (from 912,695 to 1,669,800, respectively). By 2050, this figure is expected to increase to 21% (4,994,082)1.
Osteoporosis worldwide is a serious health problem, especially in older populations. Its main consequences are fractures, with the hip being the most severe complication, associated with great morbidity and mortality. Its worldwide incidence will increase from 1.66 million in 1990 to 6.26 million in 2050, reports predict2.
Although hip fracture is the least frequent (20%) of all osteoporotic fractures3, it is considered an appropriate model for the epidemiological study of osteoporosis4, since patients who undergo it practically always enter a hospital for their attention, what allows the epidemiological registry of them5
Most available epidemiologic data concerning hip fracture comes from research carried out in the USA or Europe, whereas Latin America is scarcely considered compared to countries in the northern hemisphere (USA, Europe)6-12.
This study’s main objective was to ascertain the hip fracture incidence rates –crude, age- and gender-specific, and standardized with a reference population– in adults aged 60 years and older in Ecuador in 2016. A secondary goal was to determine if there are incidence variations by geographic region, urban or rural residence, or time of year when hip fractures occur.
Material and methods
Ecuador is located on the northwest of South America, stretching from latitudes 1°N to 4°S. The country does not undergo a definite separation of 4 seasons, as in the northern and southern hemispheres. Rather, there is one dry and one rainy season. It has different climates: a tropical and subtropical climate in the Pacific and eastern coastal regions (23 to 36°C), and a cold, temperate climate (13 to 18°C) in the Andean region of the center of the country13.
In 2016, Ecuador had 16,384,534 inhabitants, of which 1,669,800 (10.2% of the total population) are 60 years old and older1.
We present a descriptive, retrospective study based on data from hospital discharges registered in 2016 by the National Institute of Statistics and Census of Ecuador (INEC)14. The Hospital Expenditures Yearbook 2016 was used to secure the information of people aged 60 and older hospitalized with the main diagnosis of hip fracture from January 1 to December 31, 2016.
The Hospital Expenditures Yearbook is part of the National Surveillance System conducted annually by INEC14, which records the expenditures of all public and private hospitals in Ecuador. The data extracted from the hospital records contain information related to demographic and administrative data, hospital discharge status and primary diagnosis upon discharge14.
The diagnosis of hip fracture was recorded according to the International Classification of Diseases, tenth revision, clinical modification (S72.0-S72.1 and S72.2)15. Crude and age-specific incidence rates and sex were calculated for age groups 60-64, 65-69, 70-74, 75-79, 80-84 and 85 and over. To calculate the incidence rates per 100,000 inhabitants/year, the projection of the Ecuadorian population by age and sex for 2016 prepared by the Economic Commission for Latin America and the Caribbean (ECLAC)1 was used as the denominator. We calculated the incidence standardized by age by the direct method using two reference populations: 1) the one 60 or more years for Latin America prepared by the Latin American and Caribbean Demographic Center (CELADE) - Population Division of ECLAC, revision published in 20161; and 2) with the population of Ecuador according to the 2010 population and housing census16. The cases were considered to come from urban or rural areas according to the territorial division classification of Ecuador17.
Most epidemiological studies use data from Caucasian populations, generally from the USA and Europe, for standardizing incidence rates, or the World Health Organization (WHO) global ones. Latin America is a melting pot of nationalities, which share a diversity of climates, racial origin, ethnicities and socio-cultural characteristics. We used the ECLAC-published reference population for Latin America1, because it better represents the similarities of our region’s populations. In addition, for comparison purposes, we also standardize with Ecuador's own population 2010.
The hospital mortality rate was defined as the number of fatal events divided by the total number of patients hospitalized for hip fracture18. The statistical data analysis was carried out with the EPIDAT program, Version 4.2 (www.sergas.es/Saude-publica/EPIDAT). A value of p<0.05 was considered statistically significant.
Projects that involve surveys/research and bibliographic databases of public access and use (e.g., INEC)14 was excluded as it requires approval by an ethics committee in research. Even so, this study was reviewed and approved by the Teaching Hospital of the Guayaquil National Police Center Number 2 Ethics Committee.
Results
In 2016 in Ecuador, the population of adults aged 60 or older was 1,669,800 inhabitants, 10.2% of the total population (n=16,384,534). During 2016, there were 183,191 hospitalizations among people 60 years of age or older, of which 2,054 (1.12) were attributed to hip fractures.
The mean age of the total cases is 80.7±10.8 (95% CI: 80.36; 81.2); and separated by sex, 81.5±9.6 years in men (95% CI: 80.7; 82.3) (n=584) and 82.7±8.6 years in women (95% CI: 82.2; 83.1) (n=1,470).
The annual crude incidence of hip fractures in older adults (≥60 years) was 123 cases per 100,000 inhabitants (95% CI: 117.7; 128.4); 74.6 per 100,000 men (95% CI: 68.7; 80.9) and 165.8 per 100,000 women (95% CI: 157.4; 174.4) (Table 1).
The incidence of hip fracture adjusted for age standardized with the Latin American population1 was 80.1 per 100,000 men (95% CI: 73.7; 86.9) and 157.3 per 100,000 women (95% CI: 149.2; 165.4) (Table 1), and the incidence adjusted for age standardized with the population of Ecuador in 2010 was 75 per 100,000 men (95% CI: 70-79.3) and 166 per 100,000 women (95% CI: 159-173) (Table 1).
Table 1. Incidence of hip fracture in older adults in Ecuador 2016

a: incidence per 100,000 inhabitants/year; b: 95% CI = 95% confidence interval; c: standardized incidence for population ≥60 years of Latin America 20161; d: standardized incidence for population ≥60 years of Ecuador 2010. 2010 Population and Housing Census.
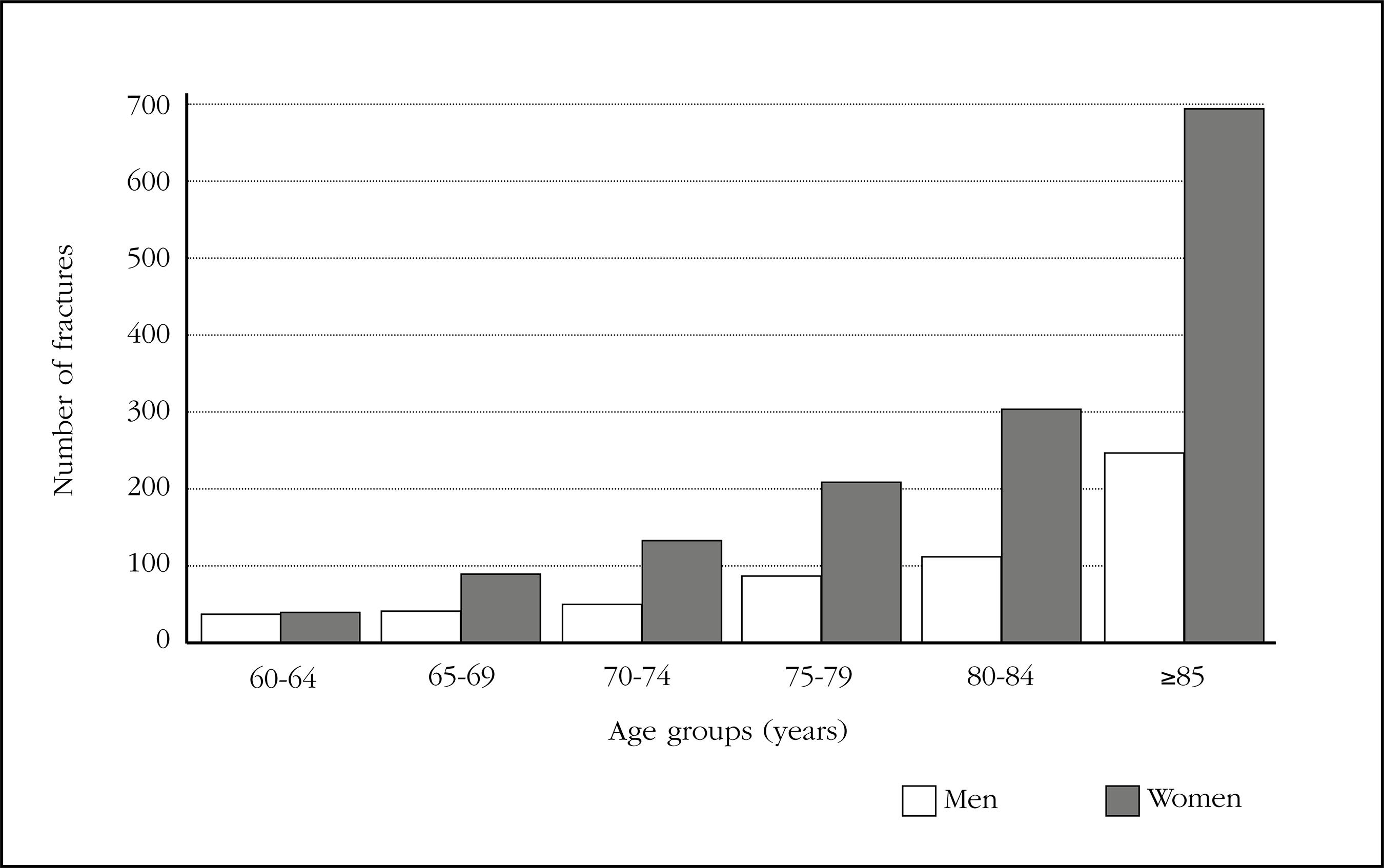
The specific incidence by age increased significantly for men and women in the group of 80 years and older, a situation that was more noticeable in women (Figure 1).

The incidence was similar in men and women aged 60-64 years, but beyond this age range the incidence was consistently higher in women (Table 1). The incidence in both sexes increased in an exponential pattern with increasing age, from 14.6 per 100,000 men and 14.7 per 100,000 women in the age group of 60 to 64 years, to 551.9 per 100,000 men and 1,086 per 100,000 women in the age group 85 years or older (Table 1).
In men, the number of fractures increased from 38 in the age group of 60-64 years, to 248 in the group of 85 years and older, an increase of 6.5 times; and in women it increased from 41 in the age group 60-64 years to 693 in the 85-year-old and older, an increase of 16.9 times (Figure 2).
In the group of 80 or more years, the number of hip fractures was 48.4% and 17.6% in women (n=995) and men (n=361), respectively.
The female: male ratio of the general incidence was 2.22, and it was higher than 1 in all age groups, except in the group of 60 to 64 years in which it was similar (ratio=1). The highest ratio between women and men was found in the groups of 70-74 and 80-84 years (2.3 and 2.1, respectively) (Table 1).
The mean age of men with cervical and pertrochanteric fractures was 81.1±9.7 and 82.5±9.3 years respectively, and in women 82.6±8.5 and 83.3±8.6 years. Femur neck fractures were more numerous than the pertrochanteric fractures, 64.8% and 30.48% respectively, while the subtrochanteric fractures were scarcely 4.72%.
57% of hip fractures cases were treated in public sector hospitals, 35.7% in private sector hospitals, and 7.15% in charitable hospitals. The duration of the overall hospital stay was 8.6±8.3 days (95% CI: 8.28; 8.99); in public hospitals it was 9.9±8.6 (95% CI: 9.4; 10.3) (n=1,173) and for private hospitals, 7.02±7.9 days (95% CI: 6.5; 7.5) (n=881).
There were no significant differences in the number of fractures between the coastal and Andean regions, 49.03% (n=1.007) and 48.2% (n=990), respectively. The Amazon and insular regions represent only 2.58% (n=53) and 0.19% (n=4), respectively (Figure 3).

In the last quarter of 2016 there were more hip fractures than in the first 3 quarters of this: 27% vs. 24.7% (p<0.001).
In the urban area, more fractures occurred than in the rural area (91.7% vs. 8.3%, p<0.05). In-hospital mortality rates were 5.1% and 3.8% for men and women, respectively.
Discussion
In the 21st century, most hip fractures will occur in developing countries, and the largest increases will occur in the countries of Asia and Latin America19. Life expectancy is increasing in all Latin American countries, presaging the increased importance of osteoporosis as a public health issue. Ecuador is also undergoing an epidemiological and demographic transition, with a growing number of older adults and increased life expectancy. The country’s life expectancy at birth in both sexes increased from 72 years in 1990 to 76 years in 2015, this increase being greater in women than in men (79 vs. 74 years, respectively). In the year 2000, the proportion of older adults in our population was 7.2% and increased to 10.2% in 2016. So, the number of fractures associated with aging and osteoporosis (fracture of hip and others) is expected to increase1
Hip fracture is the most serious complication of osteoporosis and is the one that is usually used worldwide as a model to carry out epidemiological studies4. The countries of Latin America have a common historical origin (invasion and colonization by Europeans), as well as similarities in racial origin (miscegenation), climate, economic, social and cultural development, which identifies us as a true subcontinent. These particularities are also reflected in the epidemiological trends of diseases of worldwide distribution, such as osteoporosis. For example, if one considers the specific ethnicity rates, the population of Hispanics in the US it would be in the low risk category in relation to the Caucasian population5.
There is great geographic variation in the incidence of hip fractures across continents, as well as between different regions of the same country20. On average, hip fracture rates standardized by age are highest in North America and Europe, followed by Asia, the Middle East, Oceania, Latin America and Africa2. There is a north-south gradient in European studies, and more fractures are also observed in the northern US. than in the south19,20. These variations show that demographic, geographic, environmental and ethnic factors play an important role in the epidemiology of hip fracture2. In Latin America there are also differences between the different countries of the region, and even between regions of each country6.
In a recent study of the trend in the incidence of hip fracture from 1999 to 2016 in our country22, it is reported that a marked annual increase in hip fracture rates was observed predominantly among residents of the coastal region, surpassing those rates in the Andes region in 2016. However, in the current study no significant differences in the geographical distribution of the frequency of hip fractures between the coastal and Andean regions in 2016 are shown. It should be noted that the age group at which this study was conducted is different (60 vs. 65 years), which we estimate would explain this discrepancy.
From the available studies on the epidemiology of osteoporosis in Latin America, it can be inferred that there is a generally lower incidence of hip fractures than in developed countries6. Some of these population-based studies produced incidence figures between 263.6 and 304.5 fractures per 100,000 people aged 50 or older. While others based on hospital data reported values between 40 and 362 fractures per 100,000 people aged 50 or older6-8,26. The country with the highest incidence is Peru, followed by Brazil and Argentina. Those with the lowest incidences are Venezuela and Ecuador6,11. In our study, the incidence rate in adults aged 60 and over increases with respect to a previous study11, although it is still among the lowest in the region and far below that in the northern hemisphere5. According to the classification of Kanis et al., Ecuador would be among the low risk countries5. In a previous study carried out in 2005 in our country11, a substantially lower annual incidence was reported (49.5 per 100,000) than that described in the present study. Given the different design (adult population ≥50 years), such work is not directly comparable to ours. Furthermore, there is a difference of 11 years compared to the present.
Although most studies in Latin America have shown hip fracture rates lower than those found in the population of the US, Canada and Europe, these results may be due to the selected population studied, differences in the populations’ life expectancy1, differences in the definition of the cases and other methodological factors6.
A seasonal variation in hip fracture incidence has been described, being higher in winter27. Changes in weather conditions could explain these seasonal differences27. In effect, a fall –usually from the individual’s own height– is the underlying mechanism of hip fracture in most cases. This would be favored by bad weather conditions (rainy season and/or cold, wet climate). Another mechanism involved is the metabolic alteration of vitamin D and the absorption of calcium that occurs during the winter months, although it would be less likely in the short term. Ecuador does not have a winter season similar to that of the Nordic countries, as our rainy season starts in January and ends in April. We have no explanation for the prevalence of fractures in the last 3 months of the year in the present study. In Ecuador, a vitamin D deficit has been reported in the population both in residents of the coast and in the Andean region, which could be a contributing factor to the incidence found in this study28,29. However, this evidence would not necessarily be related to the seasonality in which most fractures occurred. One limitation is, perhaps, the short period of study, which makes it difficult to investigate temporal changes in both the trend, as well as the seasonality of hip fractures. In subsequent studies, the influence of weather conditions on this seasonal distribution should be analyzed.
Although it is true our country’s Andean region dress habits and cold climate conditions13 mean less exposure to sunlight, no regional differences are found in the frequency with which hip fractures occur (coast vs. Andes).
Globally, hip fracture rates are higher in women than in men, with an average ratio of approximately 2:13,21, which concurs with our data where we find on average a 2:1 ratio.
A lower incidence of hip fracture in the rural population has been described30. Since hip fractures require immediate medical attention and, in most cases, a surgical procedure, it would be very rare for a rural inhabitant who suffers a hip fracture to not receive hospital care. This would be in accordance with our results, in which the proportion of hip fractures in rural areas is lower than in urban areas (8.3% vs. 91.7%, respectively). Similar results are observed in other countries31. A more physically active lifestyle reportedly protects them against osteoporosis and fractures31. However, it should be noted that the generally great distance from urban centers, the limited availability of transport or lack of specialized health personnel may prevent these rural patients from receiving care.
There are discrepancies in the literature on the proportion of cervical fracture/pertrochanteric fracture. For some authors, this relationship varies widely, while for others it is approximately equal. Together they comprise more than 90% of the fractures of the proximal femur2. In our study, the number of femoral neck fractures is greater than that of the pertrochanteric fractures in all age groups, 64.8% and 30.5% respectively, while the subtrochanteric fractures are only 4.72%. This probably depends on the type of population studied, since in some previous studies the average age of subjects with trochanteric fractures is greater than that of cervical fracture cases7,11. However, our results do not support this claim, as we did not find differences in the average age between cases with fracture of the femoral neck and that of other sites. We have no explanation for the prevalence of femoral neck fractures reported in the present study, but these fractures may be more sensitive to the effects of nutrition, socioeconomic and environmental factors.
The differences found in the days of hospital stay are probably due to the structure of the general medical care system and to the practices of hip fracture care in different countries. In our cohort, they were somewhat shorter (8.6±8.5 days) than those reported in other studies (11-16 days)32.
Mortality associated with hip fractures is substantial, with rates reported from 16% to 23% within 1 year after the event3,23. The risk of mortality appears to be higher in men than in women. In men, the general mortality rates in 1-year range between 18% and 31%3. This disparity in the rates was confirmed by a systematic review of the excess mortality a year after the hip fracture24. In Latin America, between 17% and 37% of patients with a hip fracture die in the year following the fracture6. In this study, the in-hospital mortality rate due to hip fracture was 5.1% in men and 3.8% in women, which is in the range reported in other studies11,23,25.
Given the nature of the design, our study presents some limitations that should be acknowledged. First, the number of cases could be underestimated if the patients had been treated outside a hospital. However, this eventuality is unlikely, given that it is estimated that practically 100% of hip fractures are treated in hospitals5. In Ecuador, the number of patients treated outside a hospital after a hip fracture is indeterminate.
Secondly, some cases may have been treated outside their habitual residence because of the fracture in another place. This constitutes an unpredictable and inevitable bias, but for reasons of probability it should not be significant. Other cases may have been transferred to another region, which is likely due to the conditions in which the communication routes with the neighboring regions are located.
Third, the design of this study does not allow to identify the mechanism that triggers the fracture, nor the presence of a previous fracture. The comorbidity of the hip fracture was not studied in this work, so we cannot infer the impact of these on mortality.
Despite these limitations, the main strength of the present study is that information was obtained from official sources that are updated every year and that collect data from all public and private hospitals throughout the country. Thus, such data are very reliable.
In our study then, we observed that the number and incidence of hip fractures increased with age in both sexes. This increase was greater among women, consistent with patterns described in most populations where there is a female predominance, an exponential increase with age and no differences according to geographic region.
Due to the aging of the population in Ecuador, it is expected that the number of hip fractures will increase considerably among people aged 80 or over. Accurate, updated epidemiological data are essential to design strategies for preventing and treating osteoporosis and its most feared consequence, hip fracture, in our country.
REFERENCES
1. Estimaciones y proyecciones de población total, urbana y rural, y económicamente activa. América latina. Ecuador. Revisión 2016. Disponible en http://www.cepal.org/es/temas/proyecciones-demograficas/estimaciones-proyecciones-poblacion-total-urbana-rural-economicamente-activa. Consultado el 20 junio de 2017 [ Links ]
2. Dhanwal DK, Dennison EM, Harvey NC, Cooper C. Epidemiology of hip fracture: worldwide geographic variation. Indian J Orthop. 2011;45(1):15-22. [ Links ]
3. Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int. 2004;15(11):897-902. [ Links ]
4. Sambrook P, Cooper C. Osteoporosis. Lancet. 2006;367(9527):2010-8. [ Links ]
5. Kanis JA, Odén A, McCloskey EV, Johansson H, Wahl DA, Cooper C. IOF Working Group on Epidemiology and Quality of Life. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int. 2012;23(9):2239-56. [ Links ]
6. Morales-Torres J, Gutierrez-Urena S. Osteoporosis Committee of Pan-American League of Associations for Rheumatology. The burden of osteoporosis in Latin America. Osteoporos Int. 2004;15(8):625-32. [ Links ]
7. Morosano M, Masoni A, Sanchez A. Incidence of hip fractures in the city of Rosario, Argentina. Osteoporos Int. 2005;16(11):1339-44. [ Links ]
8. Clark P, Lavielle P, Franco-Marina F, Ramírez E, Salmerón J, Kanis JA, et al. Incidence rates and life-time risk of hip fractures in Mexicans over 50 years of age: A population-based study. Osteoporos Int. 2005;16(12):2025-30. [ Links ]
9. Wittich A, Bagur A, Mautalen C, Cristofari A, Escobar O, Carrizo G, et al. Epidemiology of hip fracture in Tucuman, Argentina. Osteoporos Int. 2010;21(11):1803-7. [ Links ]
10. Jaller-Raad JJ, Jaller-Char JJ, Lechuga-Ortiz JA, Navarro-Lechuga E, Johansson H, Kanis JA. Incidence of hip fracture in Barranquilla, Colombia, and the development of a Colombian FRAX model. Calcif Tissue Int. 2013;93(1):15-22. [ Links ]
11. Orces CH. Epidemiology of hip fractures in Ecuador. Pan Am J Public Health. 2009;25(5):438-42. [ Links ]
12. Dinamarca-Montecinos JL, Améstica-Lazcano G, Rubio-Herrera R, Carrasco-Buvinic A, Vásquez A. Hip fracture. Experience in 647 Chilean patients aged 60 years or more. Rev Med Chil. 2015;143(12):1552-9. [ Links ]
13. Clima del Ecuador. Disponible en http://www.enecuador.com/clima.php consultado en 20 mayo 2017. [ Links ]
14. Camas y Egresos Hospitalarios. Disponible en http://www.ecuadorencifras.gob.ec/camas-y-egresos-hospitalarios. Consultado el 20 de junio 2017. [ Links ]
15. World Health Organization. 2007. International statistical classification of diseases and related health problems, 10th revision. Disponible en: http://www.who.int/classifications/apps/icd/icd10online/. Consultado 20 junio 2017. [ Links ]
16. Base de Datos-Censo de Población y Vivienda 2010.http://www.ecuadorencifras.gob.ec/base-de-datoscenso-de-poblacion-y-vivienda-2010/. Consultado 10 marzo 2018. [ Links ]
17. Clasificador Geográfico Estadístico 2016 - Esquema de Codificación de la División Político Administrativa del País. Disponible en http://www.ecuadorencifras.gob.ec/clasificador-geografico-estadistico-dpa/. Consultado 20 junio 2017. [ Links ]
18. Greenberg R.S, Daniels S.R, Glanders W.D. Medidas epidemiológicas. Capítulo 2. En: Medical epidemiology, 3rd edition. The McGraw-Hill Companies, Inc.; 2001. Versión traducida al español páginas 24-25; 3ª edición. México: Editorial El Manual Moderno, SA de CV; 2002. [ Links ]
19. Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359(9319):1761-7. [ Links ]
20. Cheng SY, Levy AR, Lefaivre KA, Guy P, Kuramoto L, Sobolev B. Geographic trends in incidence of hip fractures a comprehensive literature review. Osteoporos Int. 2011;22(10):2575-86. [ Links ]
21. Cauley JA, Chalhoub D, Kassem AM, Fuleihan Gel-H. Geographic and ethnic disparities in osteoporotic fractures. Nat Rev Endocrinol. 2014;10(6):338-51. [ Links ]
22. Orces CH, Gavilanez EL. Increasing hip fracture rates among older adults in Ecuador: analysis of the National Hospital Discharge System, 1999-2016. Arch Osteoporos. 2017;12(1):109. [ Links ]
23. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA. 2009;302(14):1573-9 [ Links ]
24. Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009; 20(10):1633-50. [ Links ]
25. Kanis JA, Oden A, Johnell O, De Laet C, Jonsson B, Oglesby AK. The components of excess mortality after hip fracture. Bone. 2003;32(5):468-73. [ Links ]
26. Riera-Espinoza G. Epidemiology of osteoporosis in Latin America 2008. Salud Publica Mex. 2009;51 (Suppl 1):S52-5. [ Links ]
27. Bischoff-Ferrari H, Orav J, Barrett J, Baron J. Effect of seasonality and weather on fracture risk in individuals 65 years and older. Osteoporos Int. 2007;18(9):1225-33. [ Links ]
28. Maldonado G, Paredes C, Guerrero R, Ríos C. Determination of Vitamin D Status in a Population of Ecuadorian Subjects. ScientificWorldJournal. 2017; 2017:3831275. [ Links ]
29. Orces CH. Vitamin D Status among Older Adults Residing in the Littoral and Andes Mountains in Ecuador. Scientific World Journal. 2015;2015:545297. [ Links ]
30. Sanders KM, Nicholson GC, Ugoni AM, Seeman E, Pasco JA, Kotowicz MA. Fracture rates lower in rural than urban communities: the Geelong Osteoporosis Study. J Epidemiol Community Health. 2002;56(6):466-70. [ Links ]
31. Chevalley T, Herrmann FR, Delmi M, Stern R, Hoffmeyer P, Rapin CH, et al. Evaluation of the ageadjusted incidence of hip fracture between urban and rural areas: the difference is not related to the prevalence of institutions for the elderly. Osteoporos Int. 2002;13:113-8. [ Links ]
32. Neuman MD, Rosenbaum PR, Ludwig JM, Zubizarreta JR, Silber JH. Anesthesia technique, mortality, and length of stay after hip fracture surgery. JAMA. 2014;311(24): 2508-17. [ Links ]
Received: December 08, 2017; Accepted: April 11, 2018
 Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
