










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
versão On-line ISSN 2173-2345versão impressa ISSN 1889-836X
Rev Osteoporos Metab Miner vol.15 no.2 Madrid Abr./Jun. 2023 Epub 25-Set-2023
https://dx.doi.org/10.20960/revosteoporosmetabminer.00001
ORIGINALS
High and very high risk of osteoporotic fractures in Chilean women
1AECE Research Group. The Association of Clinical Endocrinologists of Ecuador. Guayaquil, Ecuador
Objective:
to evaluate the application of intervention thresholds based on FRAX in Chilean women. Recategorize the risk of osteoporotic fracture to optimize the selection of eligible women for intervention.
Methods:
we selected 1782 women aged 50 and older from the 2016-2017 National Health Survey (third version). We estimated the probability of major osteoporotic fractures and hip fractures using the Chilean FRAX model. We estimated the percentage of women eligible for treatment and assessment of bone mineral density by applying specific intervention thresholds by age from 50 to 90 years and a hybrid threshold that combines age-dependent thresholds up to 75 years and, thereafter, a fixed threshold with a single fracture probability up to 90 years.
Results:
twenty-two women (1.23 %) had a previous fracture and were eligible for treatment for this reason. Using age-specific thresholds, another 33 women were eligible for treatment because the probability of major osteoporotic fracture was above the upper assessment threshold. In 1107 (62.12 %) women, bone mineral density measurement is recommended to recalculate FRAX with the inclusion of femoral neck bone mineral density. With the hybrid threshold, an additional 44 (3.69 %) women were eligible for treatment, and bone density measurement was advised in 1169 women (65.50 %). If treatment was assigned based on FRAX without bone mineral density alone, the number of women eligible for treatment was 70 (5.15 %) with an age-specific intervention threshold and 120 (6.72 %) with the hybrid threshold.
Conclusions:
the hybrid threshold identifies more women eligible for treatment compared to age-specific thresholds. The average fracture probability was higher with the hybrid threshold. Based on this, our position is to recommend the hybrid threshold.
Keywords: FRAX®; Intervention threshold; Hybrid threshold; Risk of fracture; osteoporosis; Chile
INTRODUCTION
The worldwide prevalence of osteoporosis has significantly increased and will continue to grow in the future. The main causes of this increase are the global aging population and lifestyle changes. Consequently, there will also be an increase in both the prevalence and incidence rate of fragility-related fractures associated with osteoporosis (1).
According to the latest audit conducted in 19 Latin American countries published by the IOF (2), in Chile, the incidence rate of hip fractures in people aged 50 and older is 144 cases per 100 000 inhabitants, a rate that did not vary from 2015 through 2019 (2). Recently, Quevedo et al. reported a 40 % increase in hospital discharges due to hip fractures in patients aged ≥ 45 years from 2006 through 2017 (3).
The primary endpoint of osteoporosis treatment is to prevent fractures, so it is essential to recognize and treat individuals at high risk of fractures. Several simple and cost-effective alternatives have been developed to identify and select individuals at risk who are eligible for treatment and bone mineral density (BMD) measurement (4).
The FRAX tool to predict risk of fracture was developed back in 2008 by Kanis et al. and is currently the most widely used tool across the world. It is available cost-free on the internet and allows us to assess the risk of fracture based on clinical risk factors and the elective inclusion of BMD. Its use has been added to most national and international clinical practice guidelines on the management of osteoporosis (5) including those in Latin America (6-11). Country-specific FRAX models (FRAX v4.1) are currently available in 14 countries in Asia, 36 countries in Europe, 11 in the Middle East and Africa, 2 in North America, and 2 in Oceania (https://www.sheffield.ac.uk/FRAX/) back in Jannuary 21, 2023) (12). In Latin America, the FRAX tool is available in 7 countries (13-16) including Chile, where it was built based on population data provided by Riedemann and Neira (2001-2006) (17).
The establishment of country-specific intervention thresholds based on age (following the methodology of the United Kingdom National Osteoporosis Guideline Group - NOGG) allows us to select patients eligible for treatment and refer them for BMD measurement to recalculate the risk of fracture. However, we should mention that the addition of BMD into the FRAX form is not essential to calculate the risk of fracture, which is particularly significant in countries with limited access to this technique (17). One disadvantage of age-dependent FRAX thresholds obtained using the NOGG strategy is that inequalities in treatment access arise among older individuals (18). To overcome this setback, the latest NOGG guidelines add a combination of age-dependent thresholds up to 70 years and thereafter a fixed threshold with a single fracture probability across all age groups (hybrid threshold) (18). This strategy has also been adopted by other authors who argue that the use of hybrid thresholds may be appropriate in countries with low incidence rates of hip fracture like some countries in the Middle East, Southern Europe, and Latin America (19-21).
Back in 2019, the NOGG guidelines refined the categorization of risk of fracture into high and very high to optimize treatment selection (anabolic or antiresorptive) in high risk patients (5). Using this risk recategorization, the percentage of women characterized as very high risk increased with age.
In Latin America, with the exception of Ecuador, the effectiveness of FRAX thresholds in the identification of the percentage of individuals who were eligible for intervention in respective populations has not yet been determined. This study aims to analyze the effectiveness of the Chilean FRAX model (without BMD) in identifying women who would be eligible for treatment and BMD evaluation according to age-specific intervention thresholds and a combination of fixed thresholds (hybrid threshold). An additional objective is to review and update the categorization of risk of fracture as “high” and “very high” to better guide therapeutic interventions for the prevention of fragility fractures in Chilean women.
METHODS
POPULATION
In the present study, data from participants from the 2016-2017 National Health Survey (ENS), third version, were used. This survey is a national cross-sectional study that collected information from, at least 6027 individuals aged 15 years and older, residing in metropolitan and rural areas of the 15 regions of Chile from August 2016 through January 2017. The population sample was probabilistic and geographically stratified. The complete sample design and methodological details have been described elsewhere (23). The ENS primarily employed internationally validated instruments and was designed to estimate the prevalence of priority health problems and associated risk factors. The survey forms, database, manuals, and codebooks are publicly available and can be downloaded from the website (24). For this study, all women aged 50 years and older from the ENS 2016-2017 survey were selected (n = 1782) including 1760 women without previous fractures and 22 with previous fractures. The study was approved by the ethics committee of the Hospital Docente Policía Nacional Guayaquil No.2, Ecuador.
Age and sex were self-reported. Height was measured in centimeters, weight in kilograms, and body mass index (BMI) was estimated as well (kg/m2). The questions and responses described in the supplementary table 1 were used to obtain the risk factors associated with osteoporotic fractures. Some responses needed to be transformed and recoded following the FRAX® tool recommendations to convert them into dichotomous variables. The questions and responses associated with arthritis were not used as the survey indicates they have not been validated nor were those associated with glucocorticoids since the dosage and duration of use cannot be established. Smoking habits were categorized as current, former, or never. Self-reported average alcohol consumption was recoded to adjust it as equivalent to ≥ 3 units per day. Forearm and hip fractures over the past year were self-reported. The diagnosis of secondary osteoporosis or rheumatoid arthritis (RA) was not confirmed, and data were recorded as “NO” following the FRAX questionnaire recommendations (Supplementary Table I).
POSSIBILITIES OF FRACTURE
The 10-year probability of major osteoporotic fracture and hip fracture was estimated using the FRAX® tool version 4.2 specific to the Chilean population, available online (https://www.sheffield.ac.uk/FRAX/tool.aspx?country=50). The estimates did not include BMD measurement.
INTERVENTION THRESHOLDS
Two intervention thresholds were explored: an age-specific threshold and a hybrid threshold as shown onfigure 1.

Figure 1. Graphs of intervention and assessment thresholds showing the original (A) and current (B) NOGG thresholds applied to the FRAX model for Chile. The dotted line represents the intervention threshold while the solid gray lines represent the upper and lower assessment thresholds. IT: intervention threshold; LAT: lower assessment threshold; UAT: upper assessment threshold; MOF: major osteoporotic fracture (13).
To establish the intervention thresholds and BMD assessment, the methodology adopted by the NOGG in FRAX-based guidelines for the United Kingdom (25) and previously described for the Chilean population was used (13).
The number of women aged 50 years or older exceeding the intervention threshold (and thus eligible for treatment) was estimated as a total and in 5-year age intervals using FRAX probabilities (BMD was not included in the calculation). Since a previous fracture is considered to carry sufficient risk according to the NOGG to ill-advise treatment, the intervention threshold for women without previous fractures was set at the 10-year probability (age-specific) of experiencing a major osteoporotic fracture (MOF) (hip, spine, forearm, or humerus), which is equivalent to women with prior fragility fractures according the Chilean FRAX model (version 4.2). Body mass index was set at 25 kg/m2.
ASSESSMENT THRESHOLDS TO RECOMMEND BONE MINERAL DENSITY MEASUREMENT
Two assessment thresholds were considered to make recommendations for BMD measurement. Lower assessment threshold (LAT): probability level below which neither treatment nor a BMD test should be considered. Upper assessment threshold (UAT): probability level above which treatment can be recommended regardless of BMD. The LAT was set to exclude the need for BMD measurement in women without clinical risk factors, as indicated in the European clinical practice guidelines. An UAT was selected to minimize the probability that an individual identified as high risk (based on clinical risk factors alone) could, with additional BMD information, be recategorized into a low-risk category. The UAT was set at 1.2 times the intervention threshold (25).
HYBRID THRESHOLD
The hybrid threshold is an alternative threshold that combines age-dependent thresholds up to 75 years and, thereafter, a fixed threshold with a single fracture probability up to 90 years. This threshold was adopted following NOGG recommendations because age-specific thresholds lead to disparities in access to treatment especially at older ages (≥ 70 years) based on the presence or absence of a prior fracture. The hybrid threshold reduces disparities in treatment access and decreases the need to perform bone densitometries (18,26).
ASSESSMENT STRATEGY
The strategy to establish intervention thresholds and BMD assessment followed the FRAX-based methodology approved by NOGG in the United Kingdom (26) and subsequently recommended by the European clinical practice guidelines (5). Women with a prior fragility fracture are considered eligible for treatment without further evaluation. In women without a prior fragility fracture, the strategy was based on assessing the probability of experiencing a MOF within the next 10 years. Women with probabilities below the lower assessment threshold were considered ineligible for treatment. Women with probabilities above the upper assessment threshold were considered eligible for treatment. Women with probabilities between the upper and lower limits of the assessment threshold would be referred for BMD measurement and risk of fracture reassessment.
RISK CATEGORIZATION
Women with probabilities below the LAT can be considered at low risk. Women with probabilities above the UAT can be considered for treatment. Women with probabilities between the UAT and LAT would be referred for BMD measurement and risk of fracture reassessment (intermediate risk) (5).
In addition to the low and high risk categories mentioned in the current IOF-ESCEO guidelines (5), a very high risk category can be identified. Very high risk is defined as a probability of fracture that is 1.2 times higher compared to the intervention threshold (e. g., the UAT) following a FRAX evaluation with or without BMD inclusion. In other words, the same probability threshold can be used when BMD testing is not available (27). The justification for a more refined risk characterization is to guide patients towards the most appropriate treatments (anabolic or antiresorptive) (27). The high risk category would now fall above the intervention threshold but below the UAT while the low-risk category would be below the intervention threshold (27).
STATISTICAL ANALYSIS
The characteristics of the information collected were described using descriptive analysis. Qualitative variables were expressed as absolute frequency and percentage while the quantitative ones were expressed as mean and standard deviation. Participant filtration from the database, variable transformation or recoding, and descriptive statistics were performed using IBM SPSS Statistics software package for Windows, version 26.0 (IBM Corp, Armonk, NY, New York, United States).
In this study, information from Health Surveys on epidemiological surveillance conducted by the Ministry of Public Health was used. The authors with to thank the Chilean Ministry of Health for providing us with the database. All the results obtained from the study or research are the sole responsibility of the authors and do not compromise the aforementioned institution whatsoever [http://epi.minsal.cl/encuesta-nacional-de-salud-2015-2016/].
RESULTS
A total of 1782 women over the age of 50 from the ENS 2016-2017 survey were selected. Twenty-two participants had a previous fracture. The mean age was 65.09 (10.16) years, and they had a body mass index (BMI) of 29.84 (5.58) kg/m2. A total of 376 (21,10) were current smokers, and 71 (3.98) used ≥ 3 units of alcohol per day. The baseline characteristics are shown ontable I.

The 10-year probability (mean) of MOF and hip fracture (estimated without BMD) was 4.18 (3.72) and 1.50 (2.18), respectively (Table II).
Table II. Ten-year probability of major osteoporotic fracture (MOF) and hip fracture (n = 1782) (13).

HF: hip fracture; MOF: major osteoporotic fracture; SD: standard deviation.
THRESHOLDS
The intervention and assessment thresholds specific to the Chilean population and the methodology to obtain them have been described in a former publication (13) and are shown on the supplementary table II.
The intervention threshold in Chilean women increased with age from a 10-year probability of 2.5 % at 50 years to 20 % at 90 years.
The age-specific UAT and LAT to recommend BMD measurement are also shown on supplementarytable 2. For example, at 65 years, a BMD test would be ill-advised for an individual with a fracture probability rate < 3.2 %. At the same age, a BMD test would, however, be advised for an individual with fracture probabilities between 3.2 % and 7.8 %. Treatment would be advised without the need for a BMD test (for risk of fracture assessment, but possibly for treatment monitoring) in individuals with fracture probabilities > 7.8 %. In women who undergo a BMD test, treatment would be advised for those with fracture probabilities > 6.5 %.
MANAGEMENT PATHWAY
With age-specific thresholds, 22 women (1.23 %) had a previous fracture and would, therefore, be eligible for treatment. A total of 1107 women (62.12 %) had probabilities above the LAT but below the UAT, thus indicative of the need for BMD testing. Treatment without the need for a BMD test could be advised in 33 women (0.61 %). In the case of using a hybrid threshold, 1169 women (65.50 %) had probabilities above the LAT but below the UAT, thus indicative of the need for a BMD test. Treatment without a BMD test could be advised for 44 women (3.69 %) (including the 22 women with previous fractures). If treatment was assigned based solely on FRAX without BMD measurement (including those with a previous fracture), the number of women eligible for treatment was 70 (5.15 %) with an age-specific intervention threshold, and 120 (6.72 %) with the hybrid threshold. Distribution accross the different possible scenarios is shown onfigure 2.
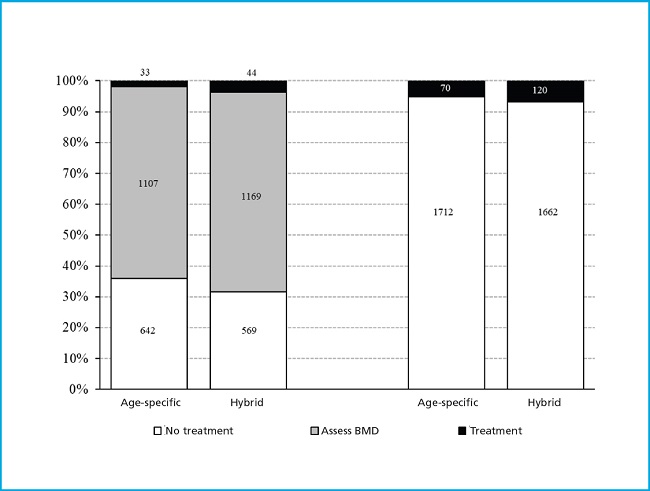
Figure 2. Distribution (n) of women assessed for risk of fracture (MOF) using age-specific or hybrid intervention and assessment thresholds. The bars on the left predict the subsequent use of DMO in those with intermediate risk. The bars on the right guide treatment using FRAX without DMO alone. MOF: major osteoporotic fracture.
The hybrid threshold (compared to the age-specific threshold) increases the number of women selected for treatment by 1.3 times when considering an intermediate risk category and by 1.71 times when treatment is assigned based solely on FRAX without BMD measurement.
Table III shows fracture probabilities in women eligible for treatment based on categorization. Fracture probabilities were higher in those eligible for treatment based on the hybrid thresholds, intermediate with age-specific thresholds, and lower in those with a previous fracture (Table III).
Table III. Ten-year fracture probabilities ( %) in women eligible for treatment according to the specified criteria.

HF: hip fracture; MOF: major osteoporotic fracture.
Using the age-specific threshold, the number of patients categorized as high risk doubled down (2.12 times; from 33 to 70). With the hybrid threshold, the number of high risk patients almost tripled (increased by 2.72 times; from 44 to 120) (Fig. 2).
Adopting the methodology used by NOGG (26), the European clinical practice guidelines, and IOF-ESCEO (5,27) for risk categorization refinement, we found that with age-specific thresholds, 50 women were categorized as high risk and 15 as very high risk whereas with the hybrid threshold, 87 women were categorized as high risk and 28 as very high risk (Fig. 3).

DISCUSSION
In this study, following the same methodology adopted by NOGG and the European clinical practice guidelines (5,25,27,28), we categorized Chilean women aged 50 and above according to fracture probabilities based on the country-specific FRAX model into low, intermediate, and high risk categories. It is demonstrated that the hybrid threshold identifies more women at high risk compared to the age-dependent threshold. The percentage of female population potentially eligible for treatment was 3.6 % or 6.4 % depending on the intervention threshold used (age-specific or hybrid). As expected, a higher percentage of women were eligible for treatment when hybrid thresholds were applied. Approximately 65 % of women would be advised to take a BMD test. BMD was not measured in this population sample, so we do not know what percentage of women would exceed the intervention threshold and, therefore, be eligible for treatment. However, we should mention that NOGG guidelines state that FRAX can be used without BMD measurement as the performance of FRAX with and without BMD is approximately equivalent (29).
In the United Kingdom National Osteoporosis Guideline Group (NOGG) and more recently in the European clinical practice guidelines (5,28), the intervention threshold is set at the fracture probability equivalent of a woman of the same age with a previous fragility fracture because if women with a previous fragility fracture are considered eligible for treatment, women without a fracture but with equivalent probabilities would also be eligible for treatment. The screening strategy for women is based on opportunistic case-finding as general population screening is ill-advised (except in North America) (30,31). Based on the NOGG guidelines, women with fracture probabilities equivalent or lower compared to those without clinical risk factors should not be evaluated with BMD. In high risk individuals, BMD measurement is ill-advised. When the estimate risk of fracture without BMD is close to the intervention threshold, adding a BMD test increases the possibility of risk re-stratification (from high to low and vice versa) (32), the use of BMD becomes more efficient.
Although FRAX is available online in 72 countries and 81 different populations, the availability of country-specific (or ethnicity-specific) intervention thresholds is limited. In a systematic review, out of 120 articles recommending FRAX for treatment decision-making, 38 did not provide clear thresholds to identify those in need for treatment (21). Most countries that have not established their own intervention thresholds have added fixed thresholds recommended by the National Osteoporosis Foundation (NOF) for the United States population (21). The NOF-recommended intervention thresholds are the result of an economic analysis conducted in 2008 and their application outside the United States is not justified (21). On the other hand, the United Kingdom NOGG clinical practice guidelines use a clinically oriented approach to determine the percentage of individuals who would be eligible for treatment. Also, costs associated with treatment depend on the algorithm used to analyze them (12).
Previously, clinical practice guidelines worldwide were based on the diagnosis of osteoporosis to make treatment decisions for each patient. Currently, there has been a paradigm shift away from diagnosing osteoporosis to assessing the risk of fracture to guide the clinical decision-making process (3,34). However, the international clinical practice guidelines on the management of osteoporosis do not consistently provide treatment recommendations based on the risk of fracture (33).
The European clinical practice guidelines have proposed risk refinement into high and very high categories to optimize the selection of anabolic or antiresorptive treatment following the evidence available on the imminent risk of fracture and previous fractures (5).
In a review of 70 English-language guidelines, 63 discussed the idea of risk of fracture, but only 34 recommended using FRAX alone to classify such risk of fracture (33). A total of 28 provided a risk category or threshold that made up an indication for drug therapy. A total of 12 guidelines reported a moderate, medium, or intermediate risk category, and management recommendations were made based on this categorization.
In Latin America, only 5 out of 7 countries with FRAX have published national osteoporosis guidelines (6-11). All of them include FRAX as a tool to assess to risk of fracture. However, in 3 of these countries, starting drug therapy to treat osteoporosis is advised based on the NOF thresholds. The Chilean guidelines do not provide a clear recommendation on whether to use NOGG- or NOF-based thresholds for treatment decision-making. Only in Colombia and Brazil, is it recommended to use the NOGG thresholds (specific to age and country) to start treatment. None of the guidelines differentiate among different types of anti-osteoporotic treatment (anabolics or bisphosphonates) based on FRAX-derived risk categorization.
Except for Ecuador (22), the application of intervention thresholds in Latin America has not been described. The findings of this study are similar to those published by López Gavilánez et al. (22) on the Ecuadorian population, in the sense that the application of risk categorization using FRAX alone without measuring BMD allowed selecting more candidates for treatment with both age-specific and hybrid thresholds.
The most appropriate intervention thresholds for a country should be decided locally considering economic factors, availability of healthcare resources, and physician based preferences (12). In Chile, the individual cost of treating a hip fracture goes from USD 4000 to USD 9000 in the public and private healthcare systems, respectively. The cost of hospitalization due to hip fractures back in 2020 was 34 million dollars per year (3). While the use of intervention thresholds has been shown to be cost-effective in Europe (5) and the UK (35) the risk of fracture (13) and healthcare costs associated with fracture care (3) in Chile are different. Therefore, the cost-effectiveness of using these intervention thresholds in the Chilean population has not yet been established through their use in the routine clinical practice and should be backed by a comprehensive economic study of the healthcare system.
There are several limitations to consider in this study. Firstly, although the survey was broad and representative of the Chilean population, there were fewer women surveyed in the older age groups (≥ 80 years = 10 %), which could affect the accuracy of our estimates and therefore the number of women eligible for treatment. Secondly, in the NOGG guidelines (26) two different FRAX results are used: the thresholds for major osteoporotic fracture and hip fracture probabilities, and treatment is advised if fracture probability exceeds the intervention threshold in either of the 2 FRAX results (or in both). The hip fracture probability varies across countries and regions worldwide while the probability of major osteoporotic fractures is less well-known. We should mention that, in most studies, the thresholds for major osteoporotic fracture probability are based on more assumptions compared to those for hip fracture (36). This study was limited to the thresholds for major osteoporotic fracture probability. Therefore, using the fracture probabilities of both sites may increase the number of women identified as high risk.
We should mention that if we defined very high risk by multiplying the intervention threshold by 1.6, as later Kanis et al. (37) did in the hybrid FRAX model, the percentage of women classified as very high risk would be much lower compared to that obtained in this study.
Thirdly, it is important to support the application of these risk of fracture assessment thresholds using cost assessment analyses too. In the United Kingdom, this approach has been proven cost-effective. However, cost-effectiveness (35) will be necessarily different in the Chilean population due to different risk of fractures and healthcare costs. This study did not take into consideration the financial impact of applying these thresholds across different healthcare institutions.
Finally, the results of this study can only be applied to the Chilean population and are not applicable to other countries in Latin America.
CONCLUSIONS
This study proved that a risk of fracture assessment strategy following the methodology proposed by NOGG, but based on the Chilean FRAX, allows us to identify many more women at high risk of fracture and, therefore, eligible for treatment according to different age-specific thresholds and an alternative threshold for older women. The study demonstrates that the hybrid threshold identifies more women at high risk compared to the age-dependent threshold. Based on this, our recommendation is to use the hybrid threshold.
The addition of country-specific intervention thresholds and risk re-stratification into high and very high categories into the national osteoporosis guidelines will positively impact treatment decision-making by physicians in countries throughout the region.
REFERENCES
1. Reginster JY, Burlet N. Osteoporosis:a still increasing prevalence. Bone 2006;38(2 Suppl 1):S4-S9. DOI: 10.1016/j.bone.2005.11.024 [ Links ]
2. LATAM AUDIT 2021. Epidemiología, costo e impacto de la osteoporosis y las fracturas por fragilidad. Available from: https://www.osteoporosis.foundation/sites/iofbonehealth/files/2022-08/LATAM%20Audit%202021%20-%20FINAL.pdf accessed 21 Jan 2023 [ Links ]
3. Quevedo I, Ormeño JC, Weissglas B, Opazo C. Epidemiology and Direct Medical Cost of Osteoporotic Hip Fracture in Chile. J Osteoporos 2020;2020:5360467. DOI: 10.1155/2020/5360467 [ Links ]
4. Kanis JA, Johnell O, De Laet C, Jonsson B, Oden A, Ogelsby AK. International variations in hip fracture probabilities: implications for risk assessment. J Bone Miner Res 2002;17(7):1237-44. DOI: 10.1359/jbmr.2002.17.7.1237. [ Links ]
5. Kanis JA, Cooper C, Rizzoli R, Reginster J-Y;Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 2019;30(1):3-44. [ Links ]
6. Radominski SC, Bernardo W, Paula AP, et al. Brazilian guidelines for the diagnosis and treatment of postmenopausal osteoporosis. Rev Bras Reumatol Engl Ed 2017;57(Suppl 2):452-66. DOI: 10.1016/j.rbre.2017.07.001. [ Links ]
7. IMSS. Diagnóstico y tratamiento de osteoporosis en mujeres posmenopáusicas. Actualización 2018. Disponible en: https://www.imss.gob.mx/sites/all/statics/guiasclinicas/673GER.pdf [ Links ]
8. Schurman L, Galich AM, González C, González D, Messina OD, Sedlinsky C, et al. Guías Argentinas para el Diagnóstico, la Prevención y el Tratamiento de la Osteoporosis MEDICINA (Buenos Aires) 2017;77:46-60. [ Links ]
9. Arinoviche Schenker R, Arinoviche Numhauser, Arriagada Maldini M, Campusano M C, Fuentealba Perez C, Gajardo Lamas H, et al. Nueva guía SCHOMM 2018. Guías de diagnóstico, prevención y tratamiento de la osteoporosis. Disponible en: http://schomm.cl/Pdfs/SCHOMM_Guias2018_Final.pdf. Sociedad Chilena de Osteología y Metabolismo Mineral. Consultado 21 september 2021 [ Links ]
10. Medina Orjuela A, Rosero Olarte O, Rueda Plata PN, Sánchez Escobar F, Chalem Chouekae M, González Reyes MA, et al. II Consenso Colombiano para el Manejo de la Osteoporosis Posmenopáusica. Rev Colomb Reumatol 2018;25(3):184-210. [ Links ]
11. Prevención, diagnóstico y tratamiento de la osteoporosis. Guía de Consulta Para el Médico de Primer Nivel de Atención [2019]. Secretaría de Salud de México. Disponible en: http://cenetec-difusion.com/gpc-sns/wp-content/uploads/2019/06/GuiaConsulta_Osteoporosis.pdf [ Links ]
12. Li-Yu J, Lekamwasam S. Intervention thresholds to identify postmenopausal women with high fracture risk:A single center study based on the Philippines FRAX model. Osteoporos Sarcopenia 2021;7(3):98-102. DOI: 10.1016/j.afos.2021.09.003 [ Links ]
13. Clark P, Denova-Gutiérrez E, Zerbini C, Sánchez A, Messina O, Jaller JJ, et al. FRAX-based intervention and assessment thresholds in seven Latin American countries. Osteoporos Int 2018;29(3):707-15. DOI: 10.1007/s00198-017-4341-4 [ Links ]
14. Zerbini CA, Szejnfeld VL, Abergaria BH, McCloskey EV, Johansson H, Kanis JA. Incidence of hip fracture in Brazil and the development of a FRAX model. Arch Osteoporos 2015;10:224. DOI: 10.1007/s11657-015-0224-5 [ Links ]
15. Jaller-Raad JJ, Jaller-Char JJ, Lechuga-Ortiz JA, Navarro-Lechuga E, Johansson H, Kanis JA. Incidence of hip fracture in Barranquilla, Colombia, and the development of a Colombian FRAX model. Calcif Tissue Int 2013;93(1):15-22. DOI: 10.1007/s00223-013-9717-7 [ Links ]
16. Lopez Gavilanez E, Johansson H, McCloskey E, Harvey NC, Segale Bajana A, Marriott Blum D, et al. Assessing the risk of osteoporotic fractures:the Ecuadorian FRAX model. Arch Osteoporos 2019;14(1):93. DOI: 10.1007/s11657-019-0644-8 [ Links ]
17. Kanis JA, Odén A, McCloskey EV, Johansson H, Wahl DA, Cooper C. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 2012;23(9):2239-56. DOI: 10.1007/s00198-012-1964-3. [ Links ]
18. McCloskey E, Kanis JA, Johansson H, Harvey N, Oden A, Cooper A, et al. FRAX-based assessment and intervention thresholds–an exploration of thresholds in women aged 50 years and older in the UK. Osteoporos Int 2015;26:2091-9. [ Links ]
19. Chakhtoura M, Leslie WD, McClung M, Cheung AM, Fuleihan GE. The FRAX-based Lebanese osteoporosis treatment guidelines: rationale for a hybrid model. Osteoporos Int 2017;28(1):127-37. DOI: 10.1007/s00198-016-3766-5 [ Links ]
20. Goldshtein I, Ish-Shalom S, Leshno M. Impact of FRAX-based osteoporosis intervention using real world data. Bone 2017;103:318-24. DOI: 10.1016/j.bone.2017.07.027 [ Links ]
21. Kanis JA, Harvey NC, Cooper C, Johansson H, Oden A, McCloskey EV. A systematic review of intervention thresholds based on FRAX:a report prepared for the national osteoporosis guideline group and the International Osteoporosis Foundation. Arch Osteoporos 2016;11(1):25. DOI: 10.1007/s11657-016-0278-z [ Links ]
22. López Gavilánez E, Johansson H, Harvey N, Lorentzon M, McCloskey E, Valdivieso Jara J, et al. The application of FRAX in Ecuador. Rev Colomb Reumatol 2021 DOI: 10.1016/j.rcreu.2021.07.004 [ Links ]
23. Departamento de Epidemiología (1). Ministerio de Salud. Gobierno de Chile. Encuesta Nacional de Salud (ENS) 2016-2017. 2018. Disponible en: http://epi.minsal.cl/encuesta-ens-descargable/ [ Links ]
24. Departamento de Epidemiología (2). Ministerio de Salud. Gobierno de Chile. Encuesta Nacional de Salud 2016-2017. 2018. Disponible en: http://epi.minsal.cl/encuesta-nacional-de-salud-2015-2016/ [ Links ]
25. Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A. Case finding for the management of osteoporosis with FRAX–assessment and intervention thresholds for the UK. Osteoporos Int 2008;19:1395-408. DOI: 10.1007/s00198-008-0712-1 [ Links ]
26. Compston J, Cooper A, Cooper C, Gittoes N, Gregson C, Harvey N, et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos 2017;12(1):43. DOI: 10.1007/s11657-017-0324-5 [ Links ]
27. Kanis JA, Harvey NC, McCloskey E, Bruyère O, Veronese N, Lorentzon M, et al. Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures. Osteoporos Int 2020;31(1):1-12. DOI: 10.1007/s00198-019-05176-3 [ Links ]
28. Compston J, Cooper A, Cooper C, Francis R, Kanis JA, Marsh D, et al. Guidelines for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK. Maturitas 2009;62(2):105-8. DOI: 10.1016/j.maturitas.2008.11.022 [ Links ]
29. Kanis JA, Oden A, Johnell O, Johansson H, De Laet C, Brown J, et al. The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int 2007;18:1033-46. DOI: 10.1007/s00198-007-0343-y [ Links ]
30. Papaioannou A, Morin S, Cheung AM, Atkinson S, Brown JP, Feldman S, et al;Scientific Advisory Council of Osteoporosis Canada. 2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary. CMAJ 2010;182(17):1864-73. DOI: 10.1503/cmaj.100771 [ Links ]
31. Cosman F, de Beur SJ, LeBoff MS, Lewiecki EM, Tanner B, Randall S, et al. Clinician's guide to prevention and treatment of osteoporosis. Osteoporos Int 2014;25:2359-81. DOI: 10.1007/s00198-014-2794-2 [ Links ]
32. Johansson H, Oden A, Johnell O, Jonsson B, de Laet C, Oglesby A, et al. Optimization of BMD measurements to identify high risk groups for treatment - A test analysis. J Bone Miner Res 2004;19(6):906-13. DOI: 10.1359/jbmr.2004.19.6.906 [ Links ]
33. Sale JEM, Gray M, Mancuso D, Inrig T, Boire G, Beaulieu MC, et al. Treatment recommendations based on fracture risk status are not consistently provided in osteoporosis guidelines. Rheumatol Int 2018;38(12):2193-208. DOI: 10.1007/s00296-018-4181-3 [ Links ]
34. Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A. How to decide who to treat. Best Pract Res Clin Rheumatol 2009;23(6):711-26. DOI: 10.1016/j.berh.2009.09.002 [ Links ]
35. Kanis JA, Adams J, Borgström F, Cooper C, Jönsson B, Preedy D, et al. The cost-effectiveness of alendronate in the management of osteoporosis. Bone 2008;42(1):4-15. DOI: 10.1016/j.bone.2007.10.019 [ Links ]
36. Leslie WD, Kanis JA. Calibration of FRAX:A Journey, not a Destination. Calcif Tissue Int 2021;109(6):597-9. DOI: 10.1007/s00223-021-00891-8 [ Links ]
37. Kanis JA, Johansson H, Harvey NC, Lorentzon M, Liu E, Vandenput L, McCloskey EV. An assessment of intervention thresholds for very high fracture risk applied to the NOGG guidelines:A report for the National Osteoporosis Guideline Group (NOGG). Osteoporos Int 2021;32(10):1951-60. DOI: 10.1007/s00198-021-05942-2 [ Links ]

Supplementary Materials
1889-836X-romm-15-2-43-gt10.jpg
Supplementary Table II. Intervention and BMD assessment thresholds (lower and upper) derived from FRAX for Chile (13).

Received: March 10, 2023; Accepted: May 18, 2023
 This is an open-access article distributed under the terms of the Creative Commons Attribution License
This is an open-access article distributed under the terms of the Creative Commons Attribution License
