










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Hemodialysis (HD) is the main treatment for patients in end-stage renal disease, however, it presents a high risk for adverse patient outcomes1. HD affects the life of Chronic kidney disease (CKD) patients and it can have negative effects on general health and well-being including mental, social, physical, emotional, spiritual, and subjective aspects. Furthermore, it can have a negative influence on physical performance, mental status, and social relationships2. Anxiety, depression and stress are frequent conditions in CKD patients, essentially during the transition from the pre-dialysis period to renal replacement therapy. Nevertheless, it tends to decrease after beginning dialysis3.
The World Health Organization (WHO) points out that subjective wellbeing is considered within the research community as an indicator of Quality of Life evaluation4. The subjective wellbeing is characterized by emotional responses, satisfaction domains, and the judgment about global satisfaction with life. The subjective wellbeing components are pleasant affect (e.g. joy, contentment, pride, affection, and happiness), unpleasant affect (e.g. guilt and shame, anxiety and worry, anger, stress, and depression), life satisfaction (e.g. desire to change, satisfaction with current life, past, and future), and a satisfaction domain (e.g. work, family, leisure, health, finances, and self) (5.
In the CKD patients the subjective wellbeing (measured by personal wellbeing index) is positively related with subjective happiness, positive affect, and quality of life and is negatively associated with negative affect. Subjective happiness, negative affect, and the physical component of quality of life are associated to the subjective wellbeing6. Moreover, higher levels of happiness are associated with higher levels of satisfaction with life in general (personal wellbeing index) (7, and also with higher levels of sense of humor8.
This study intends to disclose if CKD patients’ subjective well-being, sense of humor, and anxiety, depression and stress are significant predictors of their subjective happiness, further influencing patients’ disease management strategies and health status.
The objective was to investigate the relationship between subjective well-being, sense of humor, and anxiety, depression and stress with subjective happiness in CKD patients undergoing hemodialysis.
Material and Methods
Study design
A cross-sectional and correlational study, developed in two units of the Diaverum Dialysis Clinic and one hospital unit in the Lisbon region, Portugal, with CKD patients undergoing HD between May and June 2015.
Subjects and setting
The inclusion criteria defined were: people aged 18 years or over undergoing HD routinely for at least six months. Exclusion criteria were: people with active psychiatric illness, cognitive impairment, and non-compensated visual or hearing impairment. Information regarding these aspects was confirmed in each person’s clinical records. 253 CKD patients met the eligibility criteria (139 in Clinic 1, 114 in Clinic 2, and 15 in the hospital unit). The sample calculation was set out with a Confidence Interval of 95% and sample error of 5%. Afterwards, a random selection without replacement was made. A randomized sample of 183 people undergoing HD was selected from the dialysis clinics, 93 of clinic 1, 78 of clinic two and 12 of the hospital unit.
Procedures
Interviews were performed during the HD session by five trained nurses. The main researcher previously met with these nurses to explain the objectives and how to collect the data. Afterwards a written roadmap was provided to assist in completing the data collection instruments.
Various instruments were used to characterize the socio demographic and clinical profile of the sample (age, gender, nationality, education, occupation, marital status, dialysis sessions length, presence of hypertension and diabetes), the subjective happiness scale (SHS) (7; the satisfaction with life in general (SWLG) was measured by the Personal Wellbeing Index9; Depression, Anxiety and Stress Scale 21 (DASS - 21) (10; and Multidimensional Sense of Humor Scale (MSHS) (8.
Outcomes measurement
The SHS consists of four items, in which participants are asked to self-characterize themselves compared to their peers (items two and three) and classify their levels of happiness and unhappiness (items one and four). The last item score is reversed. The SHS uses a visual analogue scale with seven positions based on two antagonistic statements which express the level of happiness or lack of it. The application of the Portuguese scale to CKD patients shows a single factor with an internal reliability of Cronbach’s α of 0.907. Satisfaction with life in general or the personal wellbeing index is made of seven domains for the overall measure of life-satisfaction (satisfaction with standard of living, health, personal development, personal relationships, sense of security, connection to the community, and security for the future). For each domain respondents were asked to classify their satisfaction within a scale from 0 (extremely dissatisfied) to 10 (very satisfied) with a neutral intermediate position. The personal wellbeing index was measured on a scale ranging from 0 to 100 (maximum percentage of the scale). The application of the Portuguese scale to CKD patients shows the existence of a single factor, with internal reliability of Cronbach’s α of 0.829. DASS-21 was organized into three subscales: depression, anxiety and stress, each consisting of seven items. The Portuguese version of DASS 21 in CKD patients presents a bi-dimensional structure, “Depression” and “Stress/Anxiety”, with Cronbach’s α values of 0.86 for “Depression” and 0.88 for “Stress/ Anxiety” (10.
The MSHS structure was globally consistent with studies conducted in other samples, presenting satisfactory internal consistency values. It is considered a valid instrument for characterizing an individual’s “state of humor” and to describe its different dimensions. The Portuguese version of MSHS showed a structure with three factors, “Humor Production and Social Use of Humor”, “Adaptive Humor and Appreciation Humor” and “Attitude Towards Humor”, with Cronbach’s α values of 0.93, 0.90 and 0.83 respectively8.
Ethical approval
Approval was received from the ethics committee of Diaverum (Approval No 1/2015) as from the ethics committee of the Hospital Center (Approval No 175/2015). All participants signed the informed consent form after being informed about the guarantee of confidentiality of their data and the right of withdrawal without risk to oneself. Informed consent was therefore obtained from those who met the inclusion criteria and agreed to participate.
Data analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS), version 23.0. Descriptive statistics are reported as frequency, percentage, mean, and standard deviations were calculated using two-tailed Student’s t-test for pairwise comparisons, one-way analysis of variance (ANOVA) for multiple comparisons, and two-way ANOVA for multiple comparisons involving two independent variables. ANOVA analyses were subjected to Bonferroni’s post-hoc test. Inferential procedures included Spearman correlation coefficients, and multiple linear regression with control of age, marital status, professional activity and diabetes. The significance level was set at p<0.05.
Results
The sample consisted of 183 patients diagnosed with CKD, with an average age of 59.17 (±14.64) years, mostly men (59.6%). The nationality of the patients was distributed as follows: most patients are Portuguese (78.7%), followed by Cape Verdean (13.7%), Sao Tomean (3.3%), Angolan (2.2%), Guinean (1.6%), and Bulgarian (0.5%). Concerning literacy level, 3.3% were illiterate, 41.1% had the 4th grade, 18.9% the 6th grade, 15% the 9th grade, 12.2% the 12th grade and 9.4% university education. In this sample 28% of the patients were single, 53.8% married, 11.5% widowed and 6.6% divorced. Concerning occupation, 76% were retired while 24% had a regular job. Regarding health data, patients underwent hemodialysis for 70.09 (±54.2) months, 61.9% had high blood pressure and 25.8% diabetes.
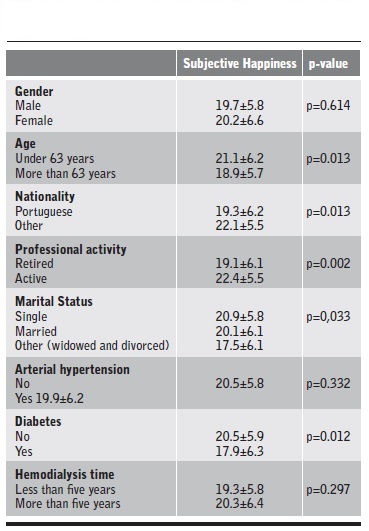
CKD patients under 63 years of age had higher levels of subjective happiness (p=0.013) than older patients. Portuguese CKD patients had the lowest score for subjective happiness (p=0.013), compared with the remaining population (Cape Verdean; São Toméan; Angolan, Guinean and Bulgarian). Retired patients had lower levels of subjective happiness (p=0.002) than those who have regular jobs. Widowed and divorced patients had lower levels of subjective happiness (p=0.033) in comparison to married and single patients (Bonferroni correction). Finally, CKD patients with diabetes had a lower level of subjective happiness (p=0.012). Table 1 shows both socio demographic and clinical factors related with CKD, that are associated with subjective happiness.
Mean score of subjective happiness was 19.9 (±6.1), satisfaction with life in general/personal wellbeing index has a mean score of 64.2% (±18.5%). Mean scores for the other variables are as following: stress/anxiety 6.9 (±6.5); depression 4.3 (±4.4); humor production and social use of humor 37.7 (±11.2); adaptive humor and appreciation humor 27.1 (±6.1) and attitude towards humor with 24.7 (±5.1) (Table 2).

Table 3 shows that the subjective happiness was positively correlated with professional activity (ρ=0.256, p<0.01); satisfaction with life in general/personal wellbeing index (ρ=0.627, p<0.001), humor production and social use of humor (ρ=0.476, p<0.001); adaptive humor and appreciation humor (ρ=0.387, p<0.001); and attitude towards humor (ρ=0.364, p<0.001). However, it presented a low negative correlation with stress/anxiety (ρ=-0.239, p<0.01) and depression (ρ=-0.391, p<0.001). Higher scores on subjective happiness were associated with higher levels of satisfaction with life in general/personal wellbeing index, humor production and social use of humor, adaptive humor and appreciation humor and attitude towards humor, though lower levels of subjective happiness were associated with higher levels of stress/anxiety and depression.
Table 3. Regression for Subjective Happiness with other variables and correlations.

*Significance p<0.05, †Significance p<0.01, ‡Significance p<0.001.
Professional activity was negatively correlated with depression (ρ=-0.222, p<0.001), satisfaction with life in general/personal wellbeing index was positively correlated with humor production and social use of humor (ρ=0.353, p<0.001); adaptive humor and appreciation humor (ρ=0.270, p<0.001) and attitude towards humor (ρ=0.211, p<0.001). Nevertheless, it presented a negative correlation with stress/anxiety (ρ=-0.297, p<0.001) and depression (ρ=-0.440, p<0.001). Higher scores on satisfaction with life in general/personal wellbeing index were associated with higher levels of humor production and social use of humor, adaptive humor and appreciation humor, and attitude towards humor, and lower levels of stress/anxiety and depression.
Stress/anxiety showed a significant positive correlation with depression (ρ=0.670, p<0.001) and attitude towards humor (ρ=0.232, p<0.01).
Depression was negatively correlated with humor production, with social use of humor (ρ=-0.164, p<0.05) and with attitude towards humor (ρ=-0.240, p<0.01). When depression values increased, humor production and social use of humor and attitude towards humor values decreased.
Humor production and social use of humor showed a significant positive correlation with adaptive humor and humor appreciation (ρ=0.718, p<0.001); and attitude towards humor (ρ=0.234, p<0.001). Lastly, adaptive humor and humor appreciation were positively correlated with attitude towards humor (ρ=0.338, p<0.001).
The model with professional activity, explains 8% of the subjective happiness variance. This control variable is the one that most contributes to the explanation of subjective happiness (ΔR2=0.115, p<0.01).
Table 4. Multiple linear regression adjusted for variables associated with the Subjective Happiness.

*Significance p<0.05, †Significance p<0.01, ‡Significance p<0.001.
In the second step, the adjusted R2 for the model was 51.4% for professional activity, satisfaction with life in general/personal wellbeing index, stress/anxiety, depression, humor production and social use of humor, and attitude towards humor, being these the variables that best explain subjective happiness. The resulting R2 were statistically significant at the p<0.00 and p<0.05 levels.
Professional activity, satisfaction with life in general/personal wellbeing index, humor production and social use of humor, and attitude towards humor had a positive effect on subjective happiness (respectively, β=0.142, p<0.05; β=0.430, p<0.001; β=0.239, p<0.05; β=0.165, p<0.01). Nevertheless, depression had a negative effect on subjective happiness (β=-0.178, p<0.05).These variables are the ones contributing the most to the explanation of subjective happiness (ΔR2=0.431, p<0.001).
Discussion
Our study was aimed at examining the relationship between subjective happiness and satisfaction with life in general/personal wellbeing index, stress/anxiety and depression, sense of humor and socio-demographic characteristics, as well as, verifying the relationship between these variables and subjective happiness.
The findings are aligned with the literature on the effects of HD on CKD patients’ life, and on the psychological stressors that may decrease wellbeing and quality of life, therefore contributing to less positive clinical outcomes11.
The highest levels of happiness were found in younger CKD patients with regular employment, married or single, non-Portuguese nationality and without diabetes. These results also corroborate the findings of another study carried out in patients undergoing hemodialysis, namely, standard of living and satisfaction with life achievements carried higher importance in subjective wellbeing12.
Such results can also be partly explained by the aging process. Older people patients on hemodialysis have peculiar characteristics, not only because of the greater number of associated comorbidities, but because the aging process itself entails physical and psychological changes that directly affect quality and life. Other aspects must also be considered as high stress factors during hemodialysis sessions13, such as the vascular access, which includes the cannulation process, bleeding, infection, lack of flow, and the inexperience of the team. Having a job minimizes the impact of the treatment routine, it makes the individual feel useful and socially active, which explains higher levels of personal fulfillment and greater happiness. One study points out that by the end of 2015, approximately 36% of patients undergoing peritoneal dialysis had full-time work, contrasting with 22% of hemodialysis patients14.
Despite the impact of treatment on the personal routine, married patients find in their family nuclei an informal but more solid support network, which strengthens their emotional component and eventually their perception of happiness. On the other hand, widowers under hemodialysis experience more hopelessness and had lower level of general health15, probably because they have nobody to share their sorrows, maintaining their feelings on the burden of disease16. These patients consequently have greater difficulty in finding adaptive strategies that allow maintaining or increasing their levels of happiness.
Concerning nationality, the non-Portuguese patients of our sample are predominantly African. The higher levels of happiness found in this population may be explained by cultural issues, as these individuals live in larger family and social networks with expanded support. This idea is supported, in part, by a study that observed a level of low contentment, and medium to high levels of hedonic affection in a group of black Africans17.
Happiness can influence socioeconomic phenomena such as consumption activities, behavior at work, investment behavior and political behavior, presenting itself as a determining factor in person´s quality of life18. In the same way, happiness was associated with higher levels of satisfaction with life in general, humor production and social use of humor, adaptive humor and appreciation humor and attitude towards humor. Though lower levels of subjective happiness were associated with higher levels of stress/anxiety and depression. The psychological disorders are the most common problems in patients undergoing dialysis, such as depression and anxiety. Hemodialysis is considered a long-term treatment and has significant side effects on physical and mental well-being19. Stress is a common reaction of patients with CKD undergoing HD which appears as a way to deal with the anxiety associated with the threat of the disease. Since they are constantly alert, they are also more vulnerable and have more difficulty in keeping an emotional state of happiness. Such findings may have important clinical implications for these patients. Untreated mental problems increase mortality, decrease quality of life, and increase the risk of suicide19. Healthcare teams must consider the need for a periodic evaluation of the stressors and their effects on the health and quality of life of the patients, with the consequent development of strategies that offer these individuals interventions that propitiate an improvement in their quality of life.
Patients undergoing hemodialysis with higher levels of subjective happiness were found to be associated with higher levels of satisfaction with life in general9. CKD patients with higher levels of sense of humor were associated with higher levels of subjective happiness and satisfaction with life in general8.
Professional activity, satisfaction with life in general, humor production and social use of humor, and attitude towards humor had a positive effect on subjective happiness. Thus, depression had a negative effect on subjective happiness.
Fordyce’s happiness program was effective in reducing depression and anxiety11), (20 and improving life of quality of patients undergoing hemodialysis20.
Keeping in mind the limitations and implications for practice of this study, we emphasize the need for further studies on nursing interventions under the promotion of happiness in the most diverse contexts of the practice of care for the person with chronic kidney disease. Its disclosure is imperative.
Practical implications for nursing
Our results suggest that CKD patients, professionally active, with lower levels of depression, with higher levels of satisfaction with life in general/personal wellbeing index, and humor production and social use of humor, and attitude towards humor had higher levels of subjective happiness. We therefore recommend that nurses should actively participate in the process of identifying and minimizing stressors, thus favouring the treatment, quality of life and wellbeing of these patients.
Such results may also help future interventions related to the emotional wellbeing (subjective happiness) of CKD patients, particularly those aimed at improving nurse training and the identification of nursing diagnosis related to well-being and monitoring the effectiveness of nursing interventions. Nurses with this knowledge could be able to optimize their patients’ health outcomes.
Depressive symptoms in CKD patients are associated with decreased wellbeing16 and consequently decreased quality of life21)-(22.
In fact, with our data we can infer that when nurses implement interventions that increase the perception of subjective happiness, they can improve the patients’ well-being and, consequently, their quality of life when patients undergoing hemodialysis however, further research is required. Several authors point out the Fordyce’s happiness program11), (20, the integration of laughter yoga23, the simulated laughter programme24 or watching humor movies, according to the patients’ preferences25, as important strategies to increase CKD patients’ happiness.
Limitations
Some limitations can be identified. Both units involved in this study are in the same geographical region influencing socio demographic characteristics, which prevents the generalization of conclusions. Also, the data collection environment (HD room) can work as a distraction factors for CKD patients. Finally, the small sample size might limit the external validity of the results.
From the results found we can conclude about the relationship between subjective well-being, sense of humor, and psychological health with subjective happiness in CKD patients. Satisfaction with life in general/personal wellbeing index, humor production and social use of humor, and attitude towards humor had a positive relationship with subjective happiness. However, depression had a negative relationship with subjective happiness.

