










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkContribution to scientific literature
Auditory stimulus can induce involuntary reflex in the middle ear. This reflex is named the acoustic reflex. An overlap exists among some neural centers that involve in processing of auditory signals and the neural centers that activates during the voluntary contractions of Valsalva and Jendrassik manoeuvres.
Valsalva manoeuvre change the activity of the cerebellum, brain stem, limbic system, amygdala and some cortical regions with different time courses, and unexpectedly has laterality and affects central nervous system in one side much more than the opposite side. Another instance is the Jendrassik manoeuvre that reinforces the stretch reflex and has peripheral and central effects on sympathetic tone. In our knowledge there is no report about the effect of these manoeuvres on stapedius muscle reflex as the smallest striated skeletal muscle of the body.
Introduction
Middle ear functions include converting sound energy into kinetic mechanical energy, amplifying sound pressure, resonance and increasing sensitivity to certain frequencies. Middle ear also protects nervous system against harsh sounds. The mechanism of the middle ear protection is by means of decreasing the energy transmission of intense sounds to the inner ear. This phenomenon is involuntary and is done by the acoustic reflex (AR). The auditory stimulus depending on its intensity can induced two responses, the startle reflex and the acoustic reflex. In humans the AR is mainly caused by stapedius muscle contraction(1). The tensor tympani muscle has no important role in human AR. The contraction of tensor tympani is due to non-acoustic stimuli such as facial stimulation, tight eyes closing, swallowing and also to auditory stimulus e.g., the startles response(2). The AR neural pathways include the vestibulocochlear nerve, the cochlear nucleus, the superior olivary complex, and the facial nerve. The central pathways of auditory signals can affect the autonomic activity of the amygdala, hippocampus, and anterior cingulate cortex(3-5). The stapedius muscle is innervated by the facial nerve. Functionally, the facial nerve contains the following components: somatic afferent (general sensory), general visceral efferents (parasympathetic), general visceral afferents, special visceral afferent (special visceral senses taste and smell), special somatic afferent (special senses related to body position) and special visceral efferents (branchiomotor). These special visceral efferents supply the motor nerve of the stapedius muscle(6-8).
All activities that have some strain are very similar to Valsalva manoeuvre (VM). Cardiovascular effects of VM and its effect on autonomic balance are well documented(9,10). The VM is an effective ways for increasing the parasympathetic activity and has clinical application in the control of supraventricular tachycardia. There is very limited evidence regarding the effect of the autonomic system on skeletal muscle reflex. However, the proposed assumptions for such effects include the autonomic modulations on muscle spindle and on the muscle blood flow(11-13).
Jendrassik manoeuvre (JM) also has clinical application. JM intensifies some muscle reflex by activation of muscle spindle through preand/or post-synaptic mechanisms(14). All forms of exertion, including anaerobic exercise, defecation, and lifting or moving heavy objects induce physiological effects that are very similar to VM. In patients with middle ear problems such as inflammatory otitis and Eustachian tube disorder, the autoinflation maneuver may inadvertently be associated with varying degrees of strain and VM-like conditions(15). However, there is very limited data regarding the effect of VM and JM on muscle reflex and in our knowledge there is no report about the effect of JM and VM on stapedius muscle. The stapedius muscle is the smallest skeletal muscle in the body and its length is about one millimeter. This skeletal muscle in humans lacks voluntary control and, unlike other skeletal muscles, its reflex contraction is not dependent on direct or painful mechanical stimulation. This muscle has a special visceral efferent innervation and its contraction protects the inner ear against loud sounds. The AR as a popular audiology test can also provide quantitative information about the stapedius contraction. In this study the modulation of acoustic reflex by VM and JM were investigated using the AR test.
Subjects and Methods
This quasi-experimental and pre-post study was self-controlled. The participants were 12 male volunteer students. The study protocol was confirmed by the research council of Golestan University of Medical Sciences. The ethic number was ir.goums.REC.1396.275. All participants were informed about the study and assigned the informed consent. All participants had good general health and had no history of disease, any drug use, any ear disease or hearing impairment. The participants underwent the general clinical and otoscopic examination. There was not any exclusion of the case from this study because of a closed ear canal, rigid ear wax, rupture of the tympanum, a history of Dizziness, vertigo and tinnitus. All experiments were performed in the morning and between 9 and 11AM. The volunteers were fasting at least 3 hours before the experiment. The subjects were test in sitting position. They were trained to remain relaxed, not to move the head, nor to swallow during the audiometric tests. The pure tone audiometry, AR and tympanometry was performed by Impedance Audiometer AT235 version 1.1, Model 1077, Interacoustics A/S; Denmark. It was calibrated for Gorgan city based on its high from the sea level. The AR was first established, using ipsilateral tonal stimulation at frequencies of 500, 1,000 and 2,000 Hz. We used auto mode for acoustic reflex test. This mode had five intensity steps. If the AR at selected frequency was elicited twice at the set-threshold then the remaining steps would be stopped automatically. The stimulus intensity for each frequency was 80, 85, 90, 95 and 100 dB(16). The frequency of sound stimulus in AR decay test was 1000 Hz. For every participant, the tympanometry and the AR tests were repeated immediately following the performance of VM and/or JM. Each participant performed the VM for 15 seconds by expiring through a plastic tube that was connected to a mercury column. The target expiratory pressure with open glottis was set at 40 mmHg. The tube had a small hole to prevent pressure from easily increasing at the mouth without any intrathoracic hemodynamic effects(17). The JM was done by clenched hand pulling which consists of pulling the hands apart against interlocked fingers(18). Mean AR threshold, AR decay, middle ear pressure and compliance were measured before and after the VM and JM. The pure tone audiometry was done for all participants. The test frequency range was 250-8K Hz.
All data were reported as mean (SD). The normal distribution of data was checked by the Shapiro-Wilk test. All variables were compared using the repeated measured ANOVA. The Mann-Whitney U test was used for non-parametric data (e.g., the left and right sides). The statistical analysis was computed by SPSS 16 statistical software.
Results
The mean (SD) of age, weight and height of participants were 21.23 (2.02) years, 71.21 (6.45) kilograms and 174.57 (5.3) centimeter respectively. A sample of tympanometry and AR tests were showed in Figure 1. A sample of AR decay test was showed in Figure 2.
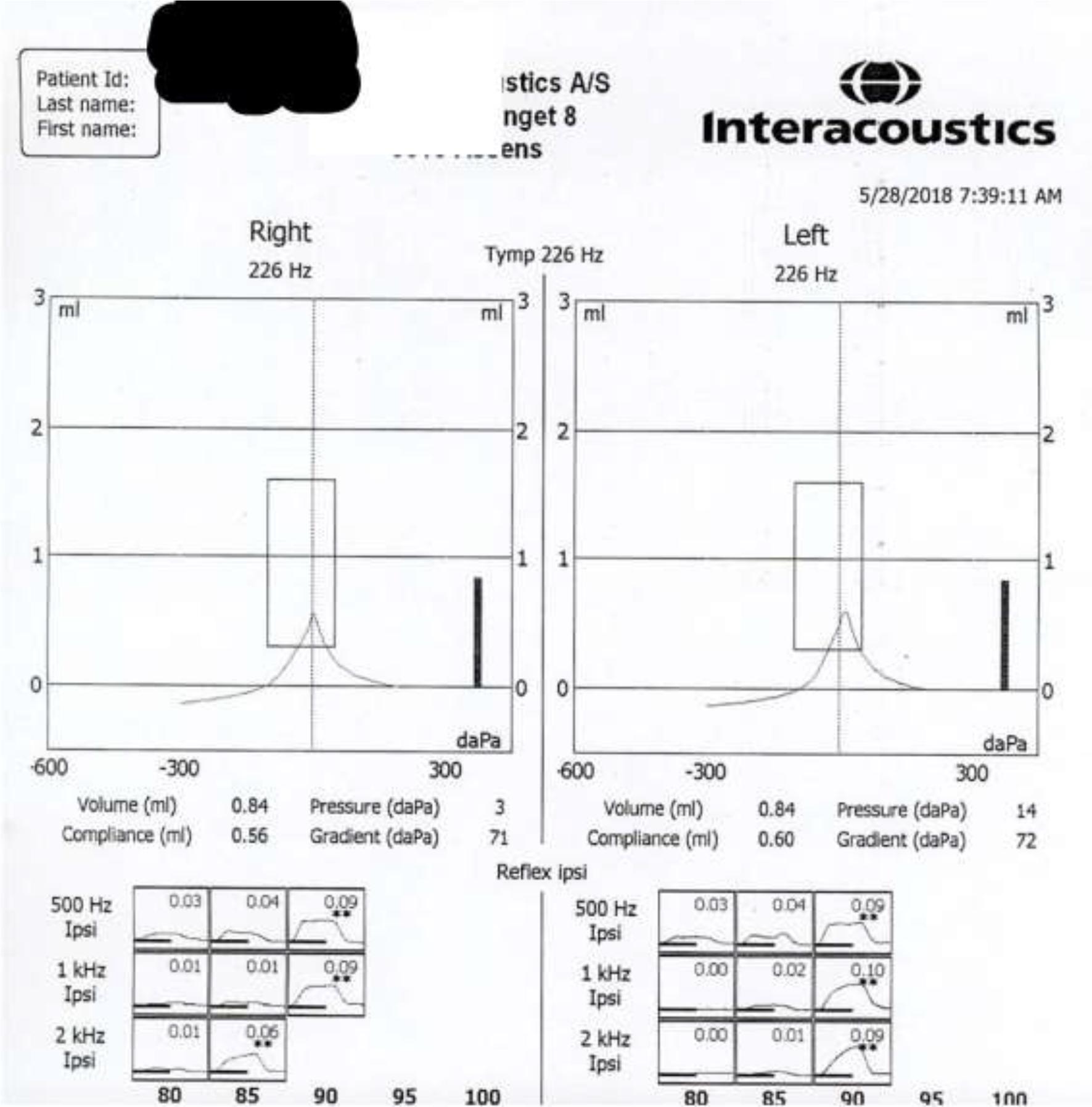
Figure 1. A sample of tympanometry and ipsilateral acoustic reflex tests. The first row represents the tympanometry of right and left ear. The second raw represents the acoustic stimulus frequency in vertical axis and its intensity in the horizontal axis. The induced and the replicable acoustic reflex are indicated by two star marks. The numbers show the deflection values of middle ear compliance in ml units.
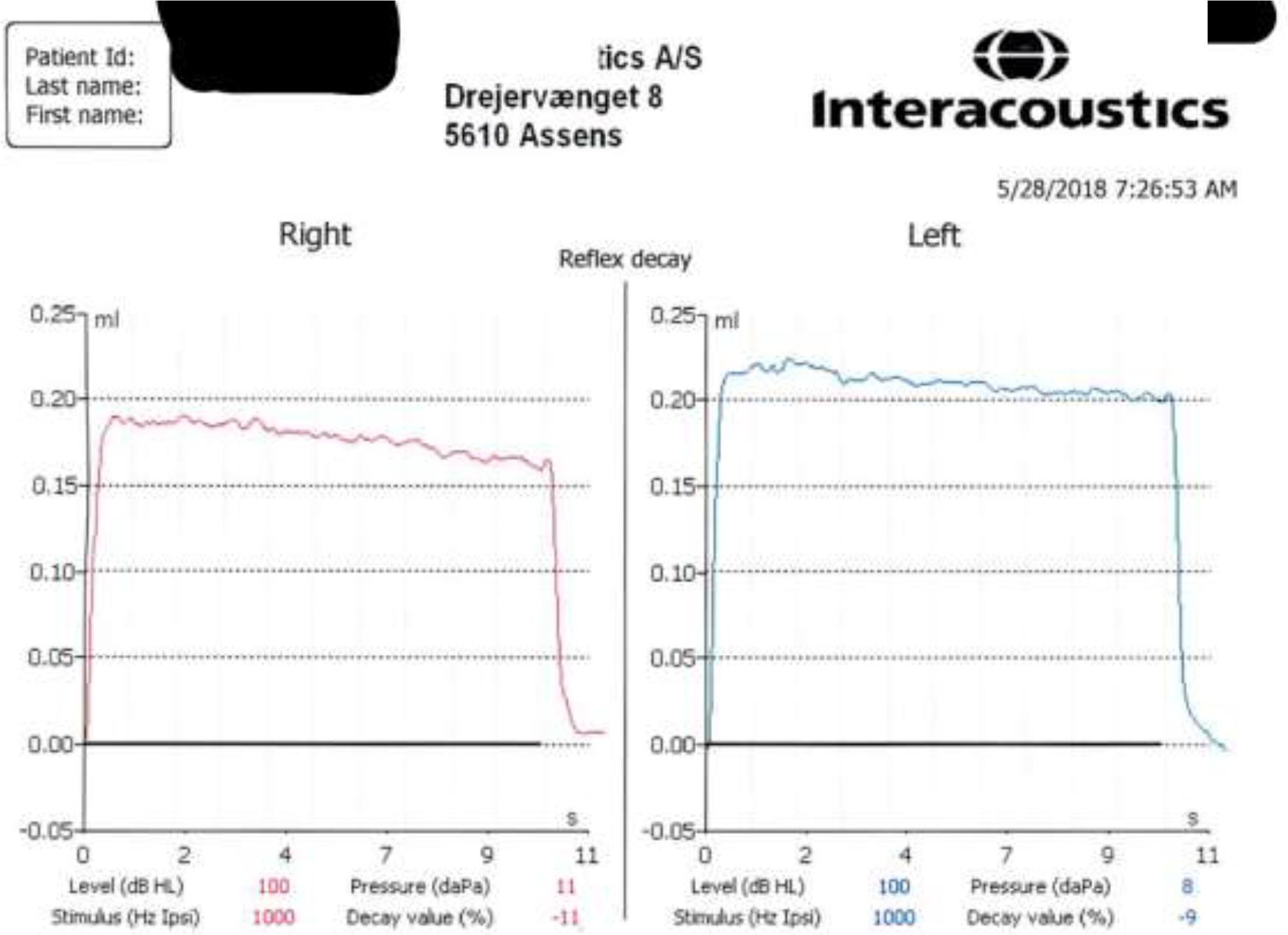
Figure 2. A sample of acoustic reflex decay test at basal condition. It represented the percent of decay of striatal muscle contraction. This contraction was induced by the 1000 Hz acoustic stimulus. The duration and the intensity of acoustic stimulus were10 seconds and 10 dB over the acoustic reflex threshold respectively.
The mean (SD) of middle ear compliance, middle ear volume, pressure gradient and AR decay at basal resting condition and after VM and JM are shown in Table 1. There were no significant changes in these variables before and after the VM or JM. All pure tone audiometry were normal and there was not any hearing loss.
Table 1. The mean (SD) of acoustic reflex (AR) decay and middle ear compliance, pressure, volume and gradient at basal resting condition and after Valsalva and Jendrassik manoeuvres, n=12.
| variable | Right | Left | ||||
|---|---|---|---|---|---|---|
| Basal | Valsalva | Jendrassik | Basal | Valsalva | Jendrassik | |
| AR decay (%) | -12.5 (5.72) | -26.83 (28.9) | -20.2 (16.7) | -14.5 (6.95) | -22.25 (29.23) |
-21.2 (17.6) |
| Compliance (ml) |
0.57 (0.15) | 0.54 (0.11) | 0.58 (0.14) | 0.65 (0.25) | 0.65 (0.27) | 0.69 (0.28) |
| Volume (ml) | 1.22 (0.29) | 1.27 (0.31) | 1.39 (0.35) | 1.11 (0.26) | 1.15 (0.32) | 1.18 (0.25) |
| Gradient (daPa) | 79.17 (6.31) | 80.17 (13.29) | 88.80 (14.65) | 79.67 (29.05) | 75 (22.47) | 82.80 (29.16) |
Discussion
These data indicated that 1000 Hz sound stimulation with 10±5 dB above the acoustic reflex threshold induced less than 15 percent decay in AR in normal healthy ears during 10 seconds. This fatigue was similar in left and right sides. Following the VM and JM this AR decay was changed to more negative values. However, these decreases were not statistically significant. Our data in resting or basal condition were similar to other reports(19). As expected, the Valsalva and the Jendrassik manoeuvres had no effect on the compliance, pressure, gradient and volume of the middle ear. It should be noted that the VM is not equivalent to autoinflation. Autoinflation means an increase in the pressure of the middle ear by the mechanism of air transfer through the Eustachian tube which is done by the person. Although not widely accepted, autoinflation is clinically practiced in some cases of serous otitis(20). The VM is a forced expiration against the closed glottis and is not associated with pressure transfer to the middle ear; VM induces hemodynamic changes and is associated direct and indirect autonomic reflexes during a 4-phase step(21). There are some evidences regarding the autonomic modulation of skeletal muscle contraction(22,23). Central or peripheral effects on muscle spindle discharges as well as the possibility of altering muscle blood flow are mechanisms that proposed for autonomic effects on skeletal muscle stretch reflex(24,25).
The autonomic effects of VM are well known. Cooke reported a baroreflex independent effect of VM on autonomic tone(26). However, the effects of VM on skeletal muscle reflex and its mechanisms are still not completely clear. León-Sarmiento reported the effect of VM on corneal or blink reflex. They proposed an inhibitory effect of VM on muscle spindle efferents(27). Loud sound can induce blink reflex by activation of facial nerve. This polysynaptic reflex has similarities to the AR(28). We did not observe any significant changes in AR decay following VM and JM. This may be related to the time course and size effect of VM or JM on AR. The time of AR decay test is 10 seconds and the autonomic effect of VM in phase 1 and 3 is very short(10,21). Therefore, a transient and short-lasting effect of VM or JM may be missed in AR decay test. The JM can increase the sensitivity of muscle spindle and can decrease the tonic pre-synaptic inhibition of the alpha motor neuron. The effect of JM on stretch reflex is very fast and transient (29). The main effect of JM is to increase the muscle spindle's sensitivity; therefore if the stapedius lacks this sensory receptor, JM will not alter its reflex contraction. We did not find any information regarding the stapedius muscle spindle in literature. The JM also has complex transcortical inhibitory effects on muscle stretch reflex. Our data may also be interpreted as a manifestation of these late inhibitory effect of JM on muscle reflex. However, this effect is reported in soleus and tibialis anterior muscles(30).
This study had some limitations and any generalization of data need more caution. They included small sample size, using only auto mode method for AR study and no simultaneous EMG recording due to technical and laboratory limitations. The application of a wideband reflectance technique instead of single probe tone for AR and a larger sample size can provide better data about the effect of VM and JM on AR.

