










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkA 62, years old female patient was admitted to the hospital for a planned laparoscopic cholecystectomy. One month earlier she was admitted with a case of acute cholecystitis and was managed conservatively. The preoperative USG demonstrated a gallbladder within normal range [70-100 mm in length and 30-40 mm in transverse diameter] with signs of cholecystolithiasis. There were no other abnormal instrumental or laboratory findings. The patient did not have any comorbid conditions. The intraoperative picture revealed a left-sided gallbladder (Figures 1 and 2), which made a standard procedure more complicated and required a change in the port placement. The cholecystectomy was performed without complications but required more time due to difficult dissection. The patient did not have other visible anomalies during laparoscopy.
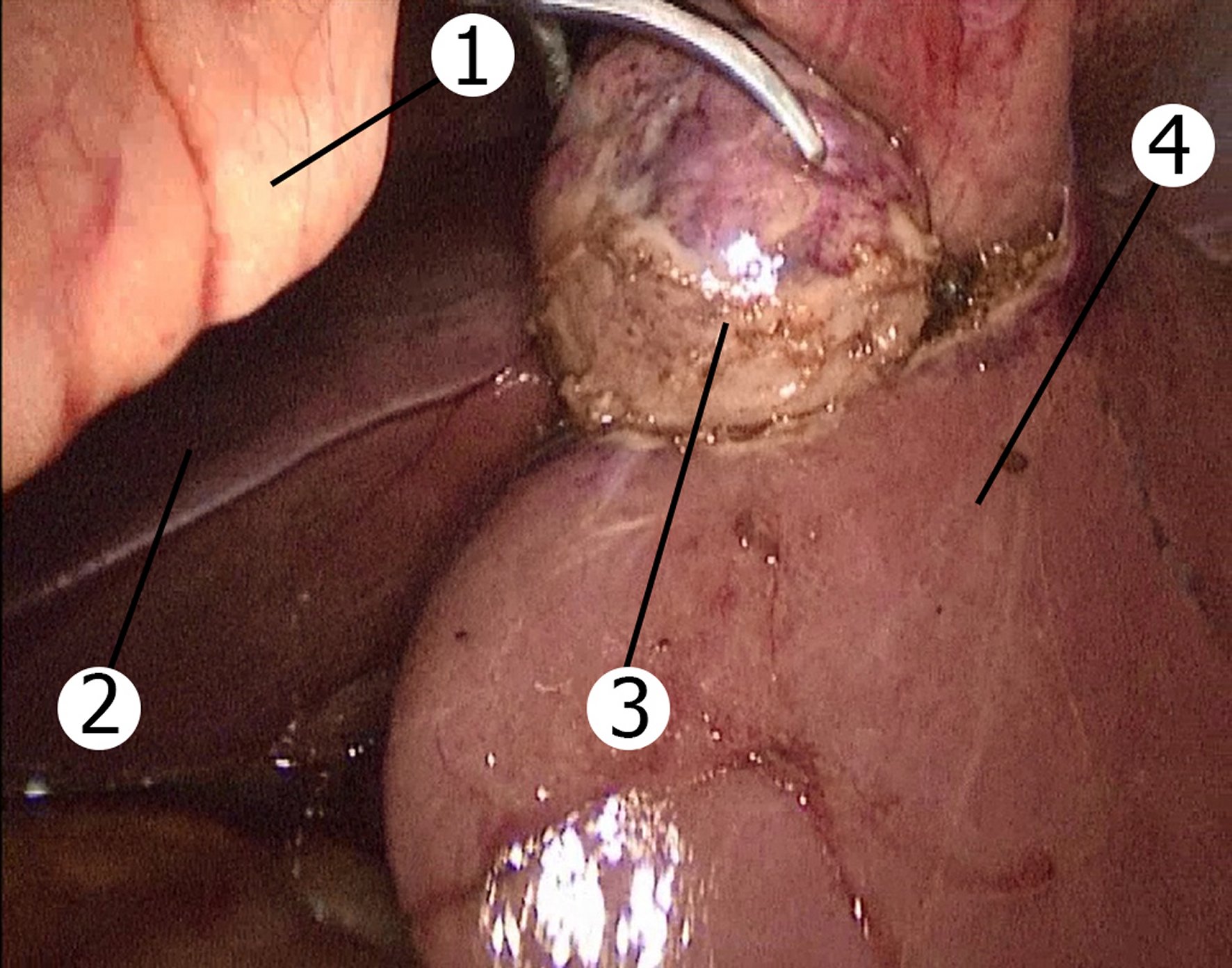
Figure 1. Left-sided gallbladder (intraoperative image).1: Round ligament; 2: Right lobe of the liver; 3: Gallbladder; 4: Left lobe of the liver.
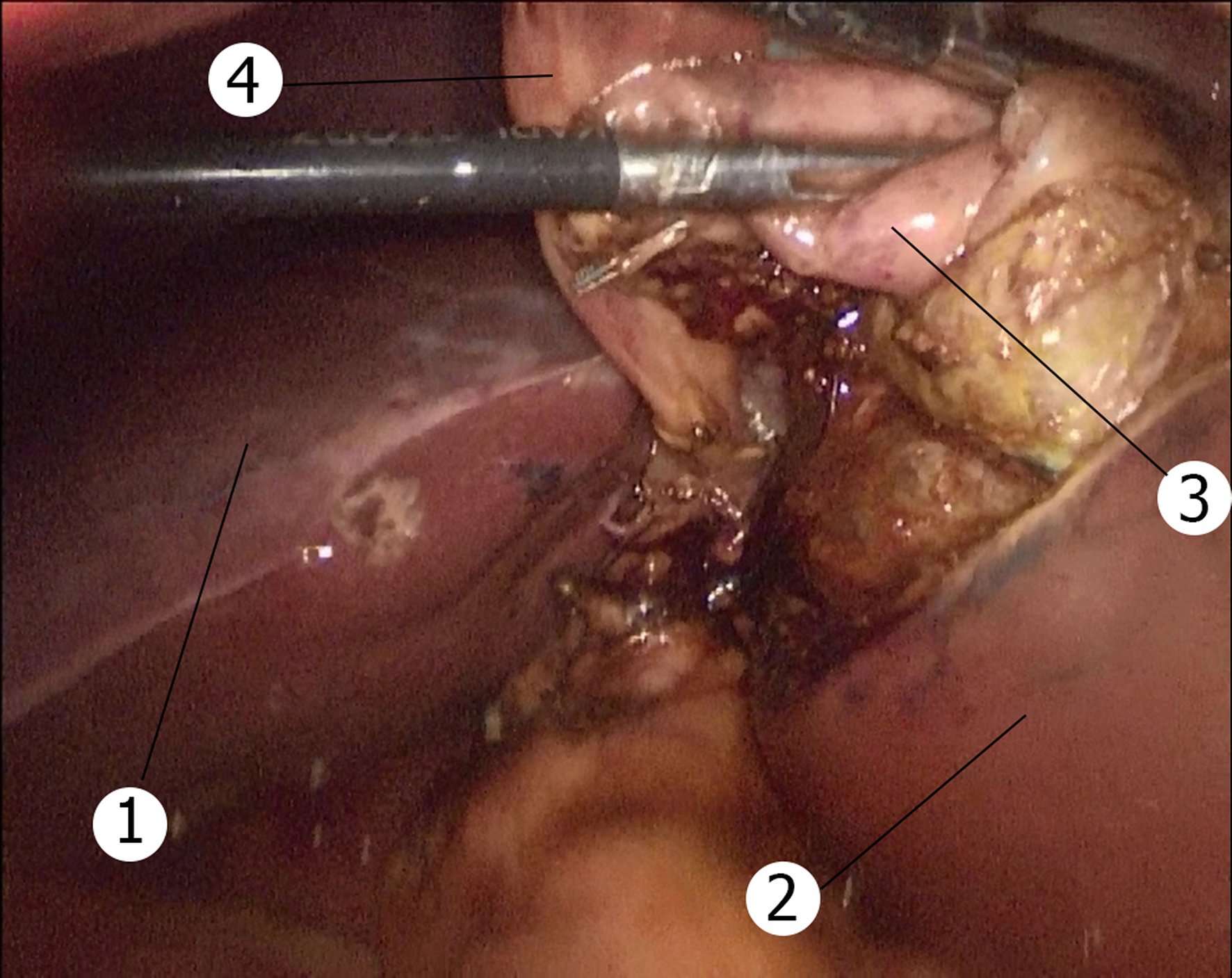
Figure 2. eft-sided gallbladder (intraoperative image).1: Right lobe of the liver; 2: Left lobe of the liver; 3: Gallbladder; 4: Round ligament.
A left-sided gallbladder is a rare anatomical anomaly when the gallbladder is located on the left side of the round ligament. It was first described by Hochstetter in 1856 and the incidence is approximately between 0.1% and 1.2% [1]. There are three possible types of this anomaly: left-sided gallbladder associated with situs viscerum inversus, true left-sided gallbladder, and cases where there is an abnormal right-sided round ligament. However, true left-sided gallbladder is the rarest of these anomalies and is located under the liver segment III. Left-sided gallbladder due to right-sided teres ligament is usually located under the IVb liver segment [2]. The anomaly arises due to gallbladder migration or development of a second gallbladder with atrophy of the original one. The main concerns during laparoscopic cholecystectomy are the necessity to change ports, modification of a standard surgical technique, and increased risk for iatrogenic injury [3]. Due to the unpredictable anatomy intraoperative cholangiography may be helpful to safely perform the procedure.
A recent systematic review and meta-analysis of fifty-three studies demonstrated that during pre‐operative imaging left-sided gallbladder was reported on imaging in 29.6% patients. There were also several cases of variants of cystic union with the common hepatic duct, the most common (67.8%) of which was union on the right side of the common hepatic duct after a hairpin bend anterior to the common hepatic duct. The study also reported that 4.4% of patients had a common bile duct injury [4]. This risk can be higher and in some reports is up to 7.3% [5].
A change in port placement is one of the possible ways to improve visualization and decrease the risk of injury. The subxiphoid trocar can be moved to the left of round ligament. Alternatively the use of left subcostal and left anterior axillary line ports, or change in patient's position may improve the outcomes and provide a better view to the surgeon. If this is not possible conversion to open surgery may be required as a last resort [3]. Left-sided gallbladder is an important and rare anomaly, which is difficult to manage. Careful dissection, change of ports and management by an experienced hepatobiliary surgeon is the optimal tactic to decrease the risk of iatrogenic injury.

