










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink1. INTRODUCTION
Human immunodeficiency virus (HIV) is one of the rampaging public health issues with profound negative impacts on lives of the infected persons, their families, communities and the society at large [1]. With its pandemic proportion, it behooves health professionals to be familiar and equipped with current facts, information and knowledge on the effect of exercise on the overall wellbeing of this population [2]. This infection ferociously attacks different systems of the body with resultant ominous complications. Such complications according to Kruger and Nell [3], include irregularities in lipid and glucose metabolism which culminate to cardiovascular disorders and other non-communicable ailments. These include redistributions of adipose tissues as seen in lipodystrophy with attendant loss of body image; alteration in musculoskeletal apparatus as observed in muscle weakness and atrophy, and reduced bone mineral density (BMD) resulting to osteopenia and osteoporosis with inherent future fall related fractures, and legions of psychosocial issues. These complications invariably affect not only the psychological, but also physical and physiological well-being of HIV-infected persons, which inadvertently result to increased risk for morbidity and mortality.
Most HIV seropositives present with bones that are fragile and less thick or dense than those in the normal population. This cohort possesses low BMD as measured by dual energy x-ray absorptiometry (DEXA) [4]. Bone density is a quantitative measurement of bone mass by the amount of minerals in grams per square centimeter (g/cm.) of bones [5]. This quantitative measurement is used in clinical medicine as an indicator for osteoporosis and fracture risks 5]. Unfortunately, highly active antiretroviral therapy (HAART), a combined therapy effective in HIV management also reduces BMD just as the infection itself [6]. Brown et al. [7] reported that studies assessing effects of initiation of HAART on BMD unanimously reported 2%–6% loss of BMD after 48–96 weeks of therapy, which is independent of the type of the HAART. This quantity of bone loss is larger than that obtained in aging alone [8]; and is equivalent to one observed in women aged 50–59 years over a period of two years [9]. However, earlier commencement of HAART is reported to mitigate bone loss, because lower CD4 cell count before the initiation of HAART leads to greater loss in BMD [10].
Effective strategies to prevent and treat reduced BMD in HIV seropositives receiving HAART are presently obscure [11]. Ali et al. [12] asserted that some pharmacological agents like bisphosphonates, teriparatide and denosumab, as well as vitamin D and calcium supplements are beneficial in the management of reduced BMD resulting from HIV and its drug therapy. However, earlier studies [13, 14, 15] found that these pharmacological remedies are associated with severe unpleasant effects such as tumors, infections, nasopharyngitis, osteosarcoma and bronchitis. Harris and Brown [15] therefore advised that these drugs should be utilized cautiously in HIV cohort. Additionally, the cost of these pharmacological agents is quite exorbitant [16]; and according to Chisati et al. [11], the drugs tend to amplify the pill burden inherent in HIV seropositives who are already saddled with HAART. Furthermore, use of pharmacological agents to treat low bone mass in HIV is known to increase non-therapy adherence and compliance in the overall management of the infection [17].
With these manifold adverse effects of drugs that combat bone loss in HIV infected persons, Howe et al. [18] reported that exercises (jogging, weight lifting, press ups, quadriceps drilling, squatting etc.) which impact forces on bones and muscles are unanimously recommended as non-pharmacological strategies for preventing and managing bone loss in HIV seropositives. Grace et al. [19] posited that impact activities and relatively high intensity progressive resistance exercises are beneficial in managing reduced BMD in this population receiving HAART. Kelley et al. [20] had also found that progressive resistance exercise interventions seem to yield higher adherence rate and compliance compared to pharmacological intervention in treating low BMD. Over two decades ago, Standish et al. [2] reported that exercise is consistently identified as the most common accessible and easily available, nontoxic and cheapest adjunct therapy for HIV management in the developed countries such as the United States (US). Indeed, the common catchphrase, “exercise is medicine in health and disease”, is never more apposite than when applied to the universal management of HIV infection.
Despite growing evidence that exercise increases BMD in the normal population [21, 22], the impact of exercise on loss of bone mass resulting from either HAART, HIV infection or both has neither been fully explored nor promoted [19]. One study by Santos et al. [23] in Brazil seems to have so far empirically examined the effect of progressive resistance exercise on BMD in HIV population. Earlier, Santos et al. [24] acknowledged the absence of data in knowledge on impact of exercise on bone health in HIV population known to be vulnerable to fracture risks. In corroboration, Chisati et al. [11] stated that knowledge on effect of exercise in increasing BMD among HIV population is presently not easily available for referencing. Maduagwu et al. [25] had hypothesized that lack of knowledge on the effect of exercise on HIV-infected persons among health professionals might be the reason for the dearth of literature (especially in the developing nations) on the impact of exercise on this population living with HIV. Additionally, Oyeyemi et al. [26] posited that adequate knowledge, skills, readiness and willingness to provide care are prerequisites for effective management of persons infected with diseases such as HIV.
We envisage that knowing and understanding the favorable impact of exercise on bone mass in HIV cohort among health professionals may stimulate interest to conduct empirical studies on this field. The authors also hope that the outcome of the envisioned studies may encourage the utilization of exercise in the management of low BMD and probably other amenable complications inherent in HIV population, especially in low-income countries. It was based on this premise that we conceived and designed this survey to evaluate the knowledge of health professionals on the impact of exercise on bone mineral density in HIV seropositives. This survey also serves as a precursor to our future empirical study on the effect of exercise on bone mass in HIV infected persons.
2. MATERIAL AND METHODS
This cross-sectional survey was conducted between 15th July and 20th October 2019 at a tertiary teaching hospital located in Maiduguri, Borno State, Nigeria that comprises over 500 beds. This health facility serves approximately 25 million people in Nigeria, and the adjoining countries (Cameroun, Chad and Niger republics). The facility has remained as a focal point of excellence in immunology and infectious diseases for more than three decades. Maiduguri is the largest and most commercialized city in the Northeastern geopolitical zone of Nigeria; and was also the capital city of the then North-eastern Nigeria. It is presently the capital of Borno State, which occupies an area of about 50,778km2, and lies on latitude 1150N and longitude 1350E. The estimated population of Borno State based on 2006 population census was 4,098,391 and it is bordered by three countries; Niger to the North, Chad to the Northeast and Cameroun to the East [27]. Population for this survey was health professionals (nurses, physicians, medical laboratory scientists, pharmacists, physiotherapists and radiographers) who were known to have contact with HIV seropositives in the course of practice at the teaching hospital. From the database of the hospital managed by the administrative office, we took permission from the head of the administration and obtained the list of each of these professional groups by their individual staff number. The list includes 473 nurses, 223 physicians, 58 medical laboratory scientists (MLSs), 23 pharmacists, 18 physiotherapists and 15 radiographers who had practiced for at least one year. We used simple random sampling technique to enrol the nurses, physicians and MLSs; whilst the whole population of each of the pharmacists, physiotherapists and radiographers was used due to their respective small population sizes [28].
The simple random sampling technique for the enrolment of the first three health professional groups was as follows: the staff numbers of the nurses were arranged chronologically and serially; so those of the physicians and MLSs. In essence, the oldest staff number on the list was the number one, followed by others. We selected every odd number from the chronologically arranged numbers of each aforementioned three professional groups. For instance, for the nurses, we selected 1, 3, 5, 7, 9…473. At the end of this sampling method, we had 237 nurses, 112 physicians and 29 MLSs, totalling 378. Total number of the pharmacists, physiotherapists and radiographers was 56. Thus, the sample size for this survey was 434. To avoid confusion as well as easy administration and identification, every staff number selected was written on each questionnaire for individual professional group. A participant was therefore administered the questionnaire that bore her/his staff number.
A researcher-designed questionnaire on knowledge on effect of exercise on bone mineral density in HIV infected persons was the tool for this survey. The questionnaire was developed by the authors, and subjected to face and content validity by four professors who are experts in orthopaedics and sports physiotherapy, cardiopulmonary physiotherapy, exercise physiology and infectious diseases. To ensure consistency, test re-test reliability of the instrument was administered on 20 health professionals randomly selected from the studied population, but were not part of the study. After two weeks, we re-administered the instrument on the same 20 health professionals. The computed reliability co-efficient, “r” was 0.75, signifying that the questionnaire is very strongly reliable. Section A of this questionnaire comprises both open and close-ended questions on respondents' socio-demographic characteristics. Before completing section B of the questionnaire, every respondent was expected to tick/check YES or NO to a question, “Do you have knowledge on effect of exercise on bone mineral density in HIV- infected persons”? Those that checked YES continued with section B. Section B contains close-ended questions of 20 items, each with three domains (“Agree”, “Disagree” or “not sure” responses) for assessing the knowledge on effect of exercise on bone mineral density in HIV- infected persons. Examples of the wordings on the items are: “Exercise is an alternative therapy in management of reduced bone mineral density in patients with HIV”; “Swimming is a better exercise for bone mineral density than walking”; “Progressive resistance exercises are proven not to be safe or beneficial in improving bone health in HIV population”; “Brisk walking and cycling can provide significant improvement in bone mineral density for HIV seropositives”; “Muscle strength increases after training protocol in HIV seropositives, it may as well increase bone mineral density because of the more expressive traction of the muscles to the bones”; “Stepping or stair climbing exercise is not ideal when administering exercise for bone mineral density in HIV infection”. A correct and wrong answer to each question scored 1 and 0 respectively; hence the summative and maximum score was 20, and minimum 0. An “Agree” response to a correct statement scored 1, a “Disagree” response to a wrong statement also scored 1.
Whilst an “Agree” response to a wrong statement scored 0, a “Disagree” response to a correct statement also scored 0. “Not sure” response was disregarded.
The aggregate of these scores were computed and the cumulative mean scores of the respondents in each professional group were compared with one another in the analysis. In addition, the cumulative mean scores of the respondents based on their sociodemographic were compared. The higher the score, the more knowledgeable the health professionals were on the effect of exercise on bone mineral density in HIV seropositives. To determine the level of knowledge of the health professionals on the effect of exercise on bone mineral density in the HIV population, the scores were ranked as follows: 0 – 4 signified poor knowledge; 5 – 9 indicated fair knowledge; 10 – 14 connoted good knowledge; ≥15 suggested very good knowledge.
The Research and Ethics Committee of the tertiary teaching hospital gave approval for the survey (approval number: UMTH/REC/19/425). We took permission from the Heads of Departments of each professional group enrolled in the study to enable us administer the questionnaire. We then approached and implored each Departmental secretary of the Departments to assist in issuing each copy of the questionnaire to each respondent. Written informed consent form containing the purpose, protocol, benefits and essence of the study as well as the assurance of confidentiality of the information obtained was attached to each of the questionnaire. Completing the questionnaire confirmed consent to participate in the study. We gave each secretary the corresponding number of the copies of the questionnaire based on the computed sample size. We instructed them to give each participant a questionnaire that bore her/his staff number. We also instructed the secretaries to inform the participants to drop the completed questionnaire in a medium sized carton, which had an opening large enough to enter the questionnaire. We placed each carton at the office of the secretary of each Department. This adopted method of administering and returning the questionnaire and the comprehensive enrolment of the 23 pharmacists, 18 physiotherapists and 15 radiographers were to guarantee anonymity and increase the response rate.
2.1 STATISTICAL ANALYSIS
Descriptive statistics of mean, standard deviation, frequency counts and percentages summarized the sociodemographic characteristics and level of knowledge of the participants.
Inferential statistic of Student t- test for independent samples analysed the knowledge on effect of exercise on BMD in HIV-infected persons between male and female participants, and between those with and without post-graduate qualifications. One-way analysis of variance (ANOVA) analysed differences on the knowledge on effect of exercise on bone mineral density in HIV-infected persons among health professionals in other five remaining socio-demographic variables. Level of significance was set at p≤0.05 using Statistical Package for the Social Sciences (SPSS) version 20.0 software (SPSS Inc. Chicago, Illinois, USA).
3. RESULTS
Out of the 434 copies of the questionnaire administered, 18 nurses, 10 physicians, three MLSs, 2 pharmacists and 2 radiographers did not return their copies; all physiotherapists returned theirs. Thus, copies returned were as follows: 219 nurses, 102 physicians, 26 MLSs, 21 pharmacists, 18 physiotherapists and 13 radiographers; totalling 399 equating to 92% response rate. Of these 399 retrieved copies, three nurses and one laboratory scientist did not duly complete theirs, and were discarded. We summarized and analysed the data based on 395 copies of duly completed questionnaire. All the respondents has knowledge on the effect of exercise on BMD in HIV seropositives; but differed in the degree of knowledge.
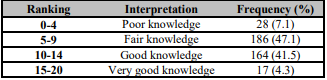
Age range and mean age in years of the respondents were 21-59 and 35.88±9.09 respectively; those in the age group of 30-39 years predominated (45.3%). Males were in preponderance (52.4%), and most (74.4%) were married; while majority (54.7%) were nurses. Participants with degree certificates accounted for 85.3% and those without postgraduate qualification constituted 80.3%. Respondents with one to 10 years working experience comprised 70.1% and most (56.0%) were of low rank. Table 1 shows the demographic characteristics of the respondents. Respondents with fair knowledge on effect of exercise on HIV- infected adult accounted for 47.1% as portrayed in Table 2.
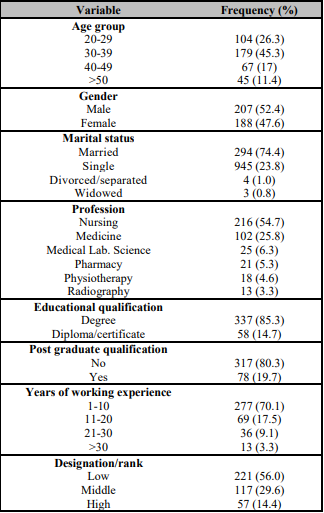
Table 2: Levels of knowledge on effect of exercise on bone mineral density in HIV seropositives among the respondents (n=395).
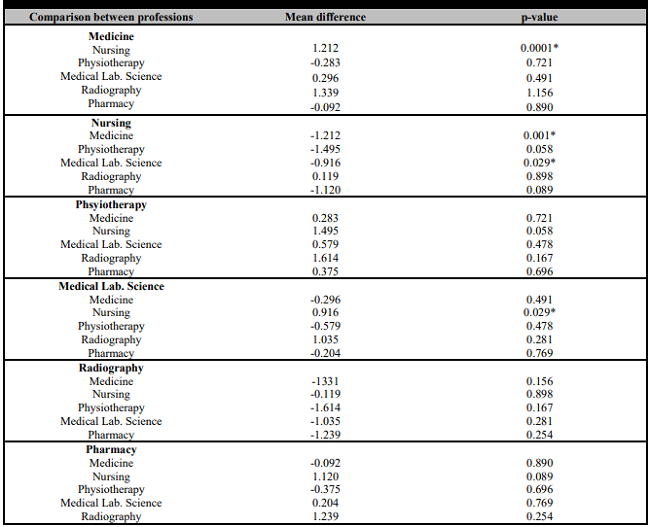
Significant difference (p<0.05; p=0.015) in the knowledge on effect of exercise on BMD in HIV seropositives existed among the health professional groups as illustrated in Table 3. Although the physiotherapists had the highest mean score (10.25 ± 3.751) on the subject as shown in the same table (Table 3); their knowledge was not significant (p>0.05; p= 0.167) when compared with those of the other health professional groups (Table 4). However, the same Table 4 portrays that physicians and laboratory scientists demonstrated significantly higher (p<0.05; p=0,001 and p<0.05; p=0.029 respectively) knowledge on the subject than the nurses.
Table 3: Statistical analysis on knowledge on effect of exercise on bone mineral density in HIV infected persons among the respondents by sociodemographic.
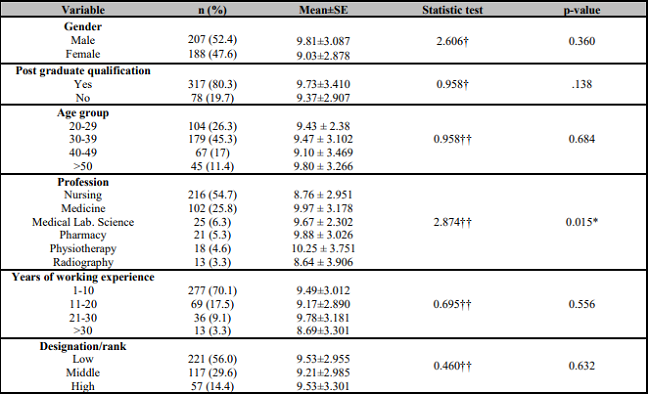
*= significant at p≤0.05;
†= Independent Student t-test;
††= ANOVA.
4. DISCUSSION
Our study on knowledge of effect of exercise on BMD in HIV seropositives among health professionals seems to enjoy global novelty. Thus, we hope that its publication in highly impact, competitive journal with open accessibility may contribute in stimulating health related exercise scientists to employ this nontoxic, low cost, easily available and accessible therapy in the prevention and management of reduced BMD, and other complications inherent in HIV seropositives.
There was a relatively male respondent (52.4%) in this study. This is not confounding, because in Nigeria most health professions from training, apart from nursing, are dominated by males. This male preponderance conforms to the findings from a study by Maduagwu et al. [25]. The male bias in this study might also be linked to socio-cultural and religious factors, which play a major role in the social and public lives of the inhabitants of Northeastern Nigeria where the study site is situated. In this part of Nigeria, most women are saddled with child bearing and upbringing, and are therefore restricted to the four walls of their homes; neither public nor work life is encouraged [29]. Nurses predominated other professions in this study; the reason is not implausible that in most public hospitals in Nigeria, nurses constitute the highest workforce among other health professionals. It may also likely be that the relative short periods of their training at many non-university public health institutions in the country might be a factor.
Substantial proportion of the participants was between the ages of 20 and 39 years. It could be reasoned that this age bracket constitutes the age of graduation from the university for most health professionals in our clime, apart from nurses trained at non-university institutions. It could also be deduced that this age group is the peak age of productivity and strength of any work force in most organizations. Majority of the respondents had degree certificates, which means they acquired university education. In our clime, diplomas are awarded to non-university graduates; most nurses are trained in non-university institutions, and these professionals predominated our study. It is therefore confounding those respondents in this study possessing degree certificates were in preponderance. From the authors' observations and anecdotal findings, some nurses, while working, strive to gain admission into the universities (mostly on part-time bases) to obtain degrees, some of these degree qualifications may not necessarily be in nursing. It was an over sight on the part of the authors not to instruct the respondents to report only the educational qualifications used in securing the employment. This may likely constitute one of the limitations to this study, because the result on educational qualification would perhaps have been different. The ratio of respondents without postgraduate qualification to those that possessed such qualification was 4:1. This is not unexpected because in Nigeria, the minimum entry requirement for any health professional who desires to pursue a clinical career at the hospital is the first degree, apart from nurses whose entry requirement may be either diploma or degree for the few who graduated from the university, mostly the younger ones.
Significant number of the respondents had less than good knowledge on the subject under discussion. The reason for this may not be easily deduced since health professionals are expected to be conversant and furnished with current facts, information and knowledge on the effect of exercise on the overall wellbeing of individuals infected with HIV [2]. This laissez-faire in knowledge on the effect of exercise on BMD in HIV seropositives among the respondents may however be connected to the old-time belief that exercise suppresses immune functions and thus increases HIV replication [30]. However, current evidence has debunked this belief and shows that exercise can reduce HIV replication and does no harm to the immune system [31]; but rather boosts and has promising effects on immune, cardiorespiratory and psychological functions, as well as body composition and metabolic status of HIV infected persons [32, 33, 34]; and improves BMD in this population [23].
Ideally, it is expected that physiotherapists should demonstrate significantly greater knowledge than the other professional groups since they incorporate exercise therapy in their practice by designing, prescribing and administering this form of therapy in both disease and health. This observed insignificant difference may not be astounding, because Oyeyemi et al. [35] found that Nigerian physiotherapists were neither familiar nor willing to manage persons living with HIV/AIDS, and showed unsatisfactory knowledge of universal precautions and AIDS pathophysiology, and low ethical temperament when it comes to providing care for persons living with HIV/AIDS [26]. Also in Canada, Worthington et al. [36] reported that most physiotherapists hardly manage persons living with HIV, were uncomfortable with the idea and HIV training was not part of the rehabilitation degree curricula. Additionally, O'Brien et al. [37] reported that few physiotherapists in Canada work with persons living with HIV.
5. CONCLUSIONS
Exercise has been shown to have a favourable effect on BMD in HIV seropositives, yet the findings of this study showed that the respondents had low knowledge about this effect. This low knowledge is worrisome as it beats the expectation of an average health professional regarding the importance of exercise among persons living with HIV. Since there is a low knowledge, this translates to inadequate utilization of exercise as a treatment option in our clime.
6. LIMITATIONS
This study was single setting centered; hence, the outcome may not be a true representation of factual situation among health professionals across other centers and settings. This may affect the generalization of the findings. Further studies, therefore, are required in multiple centers in order to ascertain a clearer view of the knowledge level of health professionals on the effect of exercise on BMD in HIV population. In addition, information on educational qualifications of the participants did not take into account the period the nurses obtained their degree certificates. This might have introduced some elements of bias in the result on qualifications.

