Diagnostic efficacy of sentinel node biopsy in oral squamous cell carcinoma. Cohort study and meta-analysis
Julio Alvarez Amézaga1, Luis Barbier Herrero2, José I. Pijoan del Barrio3, Jesús C. Martín Rodríguez1, Laura Romo Simón1, José Genolla Subirats4, Gonzalo Rios Altolaguirre4, Antonio de los Ríos5, Icíar Arteagoitia Calvo6, Salvador Landa Llona7, Jose A. Arruti González8, José López Cedrún9, Joseba Santamaría Zuazua10
(1) Cirujano Maxilofacial. Facultativo Especialista de Área. Hospital de Cruces. Servicio Vasco de Salud. Osakidetza. Bilbao
(2) Cirujano Maxilofacial. Facultativo Especialista de Área. Hospital de Cruces. Servicio Vasco de Salud/Osakidetza. Bilbao. Profesor Titular de Universidad. Departamento de Estomatología. Universidad del País Vasco/Euskal Herriko Unibertsitatea
(3) Facultativo Especialista de Área. Unidad de Epidemiología. Hospital de Cruces. Servicio Vasco de Salud/Osakidetza. Bilbao
(4) Especialista en Medicina Nuclear. Facultativo Especialista de Área. Hospital de Cruces. Servicio Vasco de Salud/Osakidetza. Bilbao ]]>
(5) Especialista en Anatomía Patológica. Jefe Clínico. Hospital de Cruces. Servicio Vasco de Salud/Osakidetza. Bilbao
(6) Médico Estomatólogo. Profesora Asociada de Universidad. Departamento de Estomatología. Universidad del País Vasco/Euskal Herriko Unibertsitatea
(7) Cirujano Maxilofacial. Jefe de Servicio. Hospital de Basurto. Servicio Vasco de Salud. Osakidetza. Bilbao. Profesor Titular de Universidad. Departamento de Estomatología. Universidad del País Vasco/Euskal Herriko Unibertsitatea
(8) Cirujano Maxilofacial. Jefe de Servicio. Complejo Hospitalario Donostia. Servicio Vasco de Salud/Osakidetza. Donostia
(9) Jefe de Servicio. Complejo Hospitalario. La Coruña. Servicio Gallego de Salud. A Coruña
(10) Cirujano Maxilofacial. Jefe del Servicio. Hospital de Cruces. Servicio Vasco de Salud. Osakidetza. Bilbao. Catedrático de Universidad. Departamento de Estomatología. Universidad del País Vasco/Euskal Herriko Unibertsitatea
ABSTRACT
]]> Objectives: To evaluate the efficacy of sentinel node biopsy (SNB) in oral squamous cell carcinoma (OSCC).Key words: Sentinel node biopsy, oral squamous cell carcinoma, cohort study, meta-analysis.
RESUMEN
Objetivos: Evaluar la efectividad de la biopsia del ganglio centinela (BGC) en el carcinoma oral de células escamosas (COCE).
Diseño: Estudio prospectivo, de una cohorte consecutiva de 25 pacientes con COCE confirmado anatomopatológicamente mediante biopsia, sin tratamiento oncológico previo, en estadiaje clínico T1-T4N0, de estos 25 pacientes 14 fueron T1-T2N0. La ausencia de enfermedad regional (N0) se determinó mediante exploración clínica y TC cervical. Para establecer globalmente la sensibilidad de la técnica se ha realizado un estudio con técnicas de metaanálisis de 10 series publicadas hasta febrero de 2005, que han aplicado BGC en el cáncer de cabeza y cuello, a la que hemos sumado nuestros 14 casos T1-T2N0 lo que hace un total de 260 pacientes.
Resultados: En los 25 casos la exactitud en la identificación del BCG fue del 96% con una sensibilidad del 66.7%. Si únicamente analizamos los casos T1-T2N0 (n=14), nuestra exactitud en la identificación fue del 100% siendo la sensibilidad de 1 (IC 95%, 0.29-1.00). La sensibilidad global fue del 93%. La exactitud en la identificación del ganglio centinela varió entre el 66% y 100%. Se identifico el GC en 251 de 260 casos, de los que 71 fueron verdaderos positivos, 5 falsos negativos y 175 verdaderos negativos. La sensibilidad global fue del 93,4% (IC 95%, 85,3-97,8) con una especificidad de 100% (IC 95%, 0,98 -100). El cociente de probabilidad negativo ponderado fue de 0,176 (IC 0,103-0,301) y el de probabilidad positivo fue de 24,75 (IC 95%, 10,8- 56,71). La odds ratio diagnóstica ponderada fue de 183,71 (IC 95%, 59,36-568,56). Si aceptamos que la prevalencia de enfermedad regional oculta es del 30%, un ganglio centinela informado como negativo tiene un 5% de posibilidades de tener enfermedad oculta.
Conclusiones: Nuestros datos aportan un cierto nivel de evidencia que el BGC es un procedimiento que por su elevada sensibilidad, puede ser aplicada en los estadios iniciales del COCE.
Introduction
The treatment of the oral squamous cell carcinoma (OSCC), and of head and neck cancer in general, when clinically presenting without regional disease (cNO) is controversial. Sentinel node biopsy (SNB) is a diagnostic technique that may contribute towards changing the management of this pathology. Accepted in breast cancer and melanoma, it remains to be validated in OSCC.
The prevalence of hidden regional metastasis in OSCC is considered to be around 30%. The most exact method of detecting hidden regional metastasis (cN+), is the anatomopathological study of the cervical lymph nodes, thus, radical cervical lymph node dissection, modified dissection, and in recent years even more selective dissections have been recommended.
Sentinel node biopsy can be considered the most selective dissection, since, theoretically, it would suppose the dissection of the first drainage node where a solid tumor metastasizes. The validity of the concept is based on the fact that if the sentinel node is free of metastasis, then other more distal nodes are also disease free.
Following the first application of sentinel node biopsy in epidermoid carcinoma of the head and neck (1), Pitman (2) using vital dyes on sixteen patients did not identify any sentinel node. Koch (3) reported 60% success in identification of the sentinel node using lymphoscintigraphy and intraoperative probes. Shoaib (4) carried out the sentinel node procedure with lymphoscintigraphy, intraoperative probes and vital dye, obtaining a high sensitivity. Other authors (5-6) established results in head and neck cancer, although in series of small samples; it being Shoaib (7) who presented results with a high sensitivity in a sample of 40 cases of head and neck cancer.
Our objective is to offer clinical and statistical results of the technique, presenting our experience in stage T1-2N0 OSCC as well as a meta-analysis of the series of cases published until February 2005.
Material and methods
]]> In order to evaluate the efficacy of SNB and to determine the existence or otherwise of regional disease in OSCC, a prospective clinical study of a cohort of patients consecutively diagnosed with OSCC by anatomopathological study was designed. The study was approved by the Ethical Board of our hospital and carried out in accordance with the Helsinki Declaration 1983. All the patients who agreed to enroll in the study were informed verbally and in writing, and signing an informed consent document.The inclusion criteria included patients with primary OSCC of the oral cavity and oropharynx with anatomopathological confirmation through biopsy of the lesion, without oncological pre-treatment, in clinical stage T1-T4 and with no clinical evidence of regional disease (N0). Twenty-five patients were recruited, 14 of whom were T1-T2 N0 (these 14 cases are those included in the meta-analytical study). The absence of regional (N0) disease was determined by means of clinical exploration and cervical CT. Patients with relapses or who had had some type of previous treatment on the anterior cervical lymph node chains were excluded.
In our 25 cases, in order to facilitate identification of the sentinel node, the triple injection procedure with lymphoscintigraphy, vital dye and gamma probe (Europrobe) was used. The day prior to surgery, the patients were infiltrated peri-tumorally at submucosal level with human colloidal seralbumin (Hazards, Nycomed Amersham-Sorin, Vercelli, Italy) labeled with 30-40 MBq 99Te, in 1 ml of saline serum.
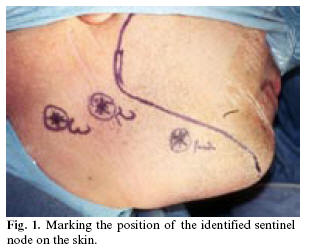
The patient was immediately transferred to the nuclear medicine service where a static lymphoscintigraphy was carried out, marking the position of the identified sentinel node on the skin. (Fig. 1) Eighteen hours later, and with the patient already anesthetized, 1 ml of blue dye (Patent Blue V, Guerbet laboratories, Cedex, France) was infiltrated in the same points. The sentinel nodes were located using a gamma probe, and identified by level. Once the sentinel node or nodes had been extracted, an elective dissection of stages I-II-III (supraomohyoid) or modified radical type III (levels I to V) was made as control in those cases where the lymphoscintigraphy showed involvement at lower levels.
The anatomopathological examination of the cervical dissection specimens was carried out via bi-dissection. In the case of a sentinel node the multi-section technique was carried out and in negative cases immunohistochemical techniques for cytokeratin were carried out.
The second part of our study is a meta-analysis of an independent review of ten series published to February of 2005 (5,6,8-15) on sentinel node biopsy applied to head and neck cancer. Each of the series included more than fifteen cases. In addition, the 14 T1-T2NO cases of our study were also included in the analysis. The Cochrane, Database and MEDLlNE databases were used to select the series for the meta-analytical study. In those cases where an article, could not be accessed, the principal investigator was contacted. Complete information was not obtained for three published articles (16-18), thus forcing their exclusion from the study.
Series containing homogeneous information for comparison and sufficient data to extrapolate only cases T1-T2 were selected. All the series used lymphogammagraphy prior to the surgical intervention and intraoperative radio-localization using a gamma probe. Six of the series (5,6,8-10,14) used vital dye.
All the series used an elective cervical or supraomohyoid, or radical modified type III dissection as control. Ross (9) carried out radical dissection as control. The follow up of the patients varied between 9 and 32 months.
Regarding the statistical analysis, basing ourselves on the Bayes theorem, instead of providing predictive values for each individual study, we have preferred to show probability quotients that operate more efficiently in the diagnostic probability calculations. For each individual study we have calculated the following diagnostic values: sensitivity, positive probability quotient, negative probability quotient and diagnostic odds ratio, with a confidence interval of 95%.
]]> The sum of the ROC curve was used to estimate the general accuracy of SNB. The study was carried out using the Metadisc program (Meta-analysis of diagnostic and screening tests. Zamora J, Muriel A, Abraira V. Clinical Biostatistics Unit. Hospital Ramón y Cajal, Madrid).
Results
Our series consists of 25 consecutively-enroled patients with OSCC stages T1-T4NO and to whom the sentinel node technique was applied between January 2001 and November 2002. Of the 25 patients, 14 were T1-T2NO and were included in the meta-analysis. The mean age was 65.9 years, SD=13.7. The male/female ratio was 17/8. The location of the primary lesion is described in Table 1. As control, a total of 28 selective cervical dissections were carried out (in three patients a cervical bilateral dissection was carried out due to the proximity of the primary tumor to the mid line and bilateral lymph node marked in the lymphoscintigraphy.
In 19 of the 25 cases, control of the stage of the cervical disease was made by selective dissection of the node levels I-II-III,and in six cases levels IV-V were included because the sentinel node was identified at those levels in the lymphogammagraphy.
SNB in our series was effective in 24 of 25 cases, accurately identifying the sentinel node in 96% of the cases. The technique could not be applied in one case as it was not possible to locate the sentinel node, so an elective cervical dissection was made, and the case was not included in the statistical analysis.
One or more sentinel nodes were identified, with an average of 3.2 per patient. The average length of the procedure, from the moment of incision to obtaining the sentinel node, was between 30 and 45 minutes.
Table 2 details the positive cases, location and distribution of the sentinel node by level, both positive and negative, the number of cases and areas of positive drainage. Of the 6 positive nodes, 2 were in level I, 2 in level II and the other 2 in level III. We did not find any positive sentinel node in levels IV - V.
The lymphoscintigraphy demonstrated that 5 (20.8%) of our cases had bilateral drainage. One of these, lingual, T1, presented bilateral positive sentinel nodes, an ipsilateral node in level I and two nodes with disease (N+)on the contralateral side in level III. Of the five cases with bilateral drainage to our tracers one was positive to disease, meaning that 20% of our cases with bilateral drainage presented contralateral metastasis. We identified another three cases in our series with drainage at unexpected node levels, without invasion node levels I-II. Two cases of primary tumors located in the anterior lingual third at stage T1 and one case in the gingiva at stage T1. These eight cases with unexpected drainage constitute 33.3% of our series.
Of the 24 cases included in our series, 18 turned out to be true negative, four true positive cases and 2 false negative cases. This represents a sensitivity of 66.6%for the technique (CI 0.22-0.96) and a specificity of 1 (CI 0.81-1).
]]> The negative probability quotient was 0.37 (CI 0.14-0.999) (Fig. 2) and the positive 24.43 (CI 1.5-397.83). The diagnostic odds ratio was 66.6 (CI 2.6-1644.3).Four nodes (16%), clinically considered as N0 before the intervention, revealed hidden micrometastases diagnosed by immunohistochemistry and not by anatomopathological bi-dissection. (Table 2). Of these two false negatives, one was a tumor (T3) at the base of the tongue, where a sentinel node was indicated as negative in level V and the control cervical dissection contained a positive node in level III.
The second case was in the jugal mucosa (T3) where a node of 10mm in diameter (obtained in level I) did not take up either radiotracer, or dye and was given as positive. Both the cervical dissection and the two sentinel nodes obtained were indicated as negative to disease.
Lymph node metastases were found in levels I, IIA, IIIA and IIIB, however the nodes obtained in levels IV and V were disease free. (Tables 1 and 2)
Regarding the meta-analysis, ten series published (5,6,8-15) on sentinel node biopsy in epidermoid carcinoma of head and neck were included in addition to our series. All the series included more than 15 cases, comprising a total of 260 SNB procedures. The basic descriptive information of the series is shown in Table 3, including our 14 T1-T2 cases.
From the analysis of these series, a similar incidence of false negatives can be deduced. We did not find any significant differences between the series that analyze cases in initial stages T1-T2 and those that include cases T1-T4 (p>0.05).
The accuracy of the technique in identifying the sentinel node varies between the 66 and 100%, with 251 of the 260 cases identified (96.5%). The results show 71 true positive cases, 5 false negatives and 175 true negative cases. This constitutes an overall sensitivity for the technique of 93.4% (CI 85.3-97.8) with a specificity of 100%, (CI 0.98-100). The negative weighted probability quotient is 0.176 (CI 0.103-0.301). (Fig 3). The positive probability quotient is 24.75 (CI 10.8-56.71). The weighted diagnostic odds ratio is of 183.71 (CI 59.36-568.56). No statistically significant evidence exists (p=0.16) for the threshold effect shown in the regression curve by Moses (19,20). In Fig 3 it can be seen that the area under the ROC curve was 0.989 (standard error 0.0059).
Discussion
Although diagnostic tools have developed significantly, we have no effective procedures available to identify hidden metastatic disease in the cervical lymph nodes of patients with OSCC. The incidence is situated at around 30%, a high percentage, and the presence of regional disease is the cause of the death of one of every two patients. (21, 22).
]]> The recommendation to carry out an elective cervical dissection when the probability of hidden cervical metastasis is higher than 20% persists (23-25), for this reason the use of elective dissections and its variants is common practice in the staging of regional disease in OSCC (26-32).Analyzing less invasive procedures, the application of SNB has been demonstrated to be very useful in other types of cancer (33,34) and for this reason we have studied its application in primary OSCC, presenting the results of a series of 25 patients and a meta-analytical study, in an attempt to determine if SNB is a useful technique in the diagnosis of regional metastasis.
In our series it was possible to apply the technique in 96% of the patients, a very similar percentage to other contrasted series. The technique is quickly applied in comparison with cervical staging dissections.
It remains to be determined if the absence of lymphatic drainage, demonstrated by a lymphoscintigraphy has any diagnostic significance in itself, since it could indicate some blockage of the lymphatic system by the disease.
We center the present study on T1-T2 cases aiming to prioritize the homogeneity of the study. Our results do not reveal any heterogenetic significance in the diagnostic indicators among the studies analyzed in these cases.
The overall sensitivity of 93.4% with a negative probability quotient of 0.176% makes sentinel node biopsy a diagnostic tool able to substantially reduce the uncertainty over regional staging, demonstrating a DOR of 183.71 with an area under the curve of 0.989. Instead of providing predictive values, we have preferred to show probability quotients, since the former are strongly dependent of the prevalence of the disease and the latter allow a more simple application of the Bayesian theory of diagnostic probability estimation. Supposing an estimation of 30% hidden metastasis (the general prevalence in our study is 24.8%), the post-test probabilities would be 88% for a positive test result and almost 5% for a negative test result. This supposes that a sentinel node biopsy, when technically possible could significantly alter the diagnosis in cases without clinical regional disease, since the possibility of hidden disease with a negative test result is lower than 5%.
SNB revealed hidden metastasis in four of the cases considered clinically to be free of disease, equal to 16% of our series. (Table 1) Two of these cases being identified by immunohistochemistry only. If we consider the results obtained only by anatomopathological bi-dissection, we would have improved the staging in only two cases (8% of cases). This is another of the benefits to be gained from the application of the sentinel node concept.
Another advantage supposes the possibility of applying advanced anatomopathological study techniques to a very reduced number of lymph nodes (72 sentinel nodes in 22 patients with a mean of 3.2 per case), against an entire regional dissection, usually with more than 10 nodes, thus allowing an increase in the staging sensitivity. Our results are similar to those of Van Brekel (35) and Czerniecki (36) who using multi-slicing techniques and immunohistochemistry find optimized positive sentinel node identification in 21% and 10% of cases respectively.
Among those factors that may influence the sensitivity of the anatomopathological study of these adenopathies are those attributable to errors in taking the sample which will depend on the size and location of the metastasis, the size of the adenopathy, on the orientation within their section and on the number of sections evaluated.
A recent multicenter study (37), in which we took part, shows that applying immunohistochemical procedures in SN optimizes staging by 17%, (59/348) against 6% (67/1180) if the anatomopathological study is carried out using bi-dissection and hematoxylin-eosin staining.
]]> Ross (9) using multi-section techniques and immunohistochemical marking, identified hidden metastasis in 5 of 27 patients (19%), the other 22 patients were confirmed with standard bi-dissection techniques and hematoxylin-eosin staining.These data suggest that multi-section and immunohistochemical techniques should be applied systematically in SN, since they significantly increase the sensitivity of the anatomopathological study. Another subject to mention is the cervical drainage pattern of the metastasis: is it predictable? In the lymphoscintigraphy, 12.5% (3/24) of our cases that did not involve the mid-line presented bilateral drainage. We found another three cases in our series with drainage in unexpected lymph node levels, in that the node stages I-II were skipped. These unexpected drainages constituted 20.8% of our cases. With these data one might ask if the lymphatic route of regional metastasis in OSCC is predictable. Kowalski (38) in a review of 513 patients found that in high risk patients the possibility of presenting contralateral metastasis is greater than 20%. Byers (39) in a review of lingual tumors at stage T1 to T2 found 16% of cases with an unpredictable or disordered drainage and were defined as "skip metastases" and which we have named jump metastases. Other authors such as Woolgar (40) found a 10% incidence in 154 patients.
Why does this occur? Do aberrant lymphatic canals or paths exist that become permeable under special circumstances? Among the possible answers it has been suggested that a primary tumor drains to a node defined by the immune system. It is not clear if the tumor cells stimulate the immune system inside the lymph nodes, increasing the uptake of the metastatic cells, or if they do this by suppressor T cells induced by the tumor that limit the action of the cytotoxic T cells, allowing the implantation of the metastatic cells in the lymph nodes. Schuller (41) attempting to evaluate regional immunity in head and neck cancer, put lymphocytes extracted from the same patients lymph nodes in contact with the tumor and observed that the immune system is regionally active. Is it the metastatic node that activates the response or is this immunostimulated by the tumor? This same author (42) with non-specific stimulants of the immune system found an intrinsic response from the lymph node. Chu (43) suggests that the tumor stimulates the T helper lymphocytes through antigen carrier cells that circulate from the tumor toward the lymph node containing the antigen-specific T cells (the sentinel node).
Cochran (44) demonstrates a reduction in the paracortical area, and of dendritic cells in sentinel nodes in melanoma resulting from immunosuppression factors liberated by the tumor. These data suggest more an immune and histopathological justification of the sentinel node concept than the classic system of stratified lymph node stations that would partly explain the so-called "skip metastases" or "jump metastases".
Conclusions
Our study contributes a certain degree of evidence that in T1-T2N0 OSCC, SNB should be considered a highly sensitive diagnostic procedure, thus it is a valid alternative to elective stage dissection. It reduces both time spent in surgery and postoperative morbidity. The technique should be carried out using lymphoscintigraphy, vital dye and an intraoperative gamma probe.
References
1. Alex JC, Krag DN. Gamma-probe-guided localization of lymph nodes. Surg Oncol 1993;2: 137-44. [ Links ]
2. Pitman KT, Johnson JT, Edington H, Barnes L, Day R, Wagner RL et al. Lymphatic mapping with isosulfan blue dye in squamous cell carcinoma of the head and neck. Arch Otolaryngol Head Neck Surg 1998;124:790-3. [ Links ]
3. Koch WM, Choti MA, Civelek C, Eisele DW, Saunders JR. Gamma probe directed biopsy of the sentinel node in oral squamous cell carcinoma. Arch Otolaryngol Head Neck Surg 1998; 124:455-9. [ Links ]
4. Shoaib T, Soutar DS, Prosser JE, Dunaway DJ. A suggested method for sentinel node biopsy in squamous cell carcinoma of the head and neck. Head Neck 1999;21:728-33. [ Links ]
5. Mozzillo N, Chiesa F, Botti G, Caraco C, Lastoria S, Giugliano G, et al. Sentinel node biopsy in head and neck cancer. Ann Surg Oncol 2001;8:103-5. [ Links ]
6. Stoeckli SJ, Steinert H, Pfaltz M, Schmid S. Sentinel lymph node evaluation in squamous cell carcinoma of the head and neck. Otolaryngol Head Neck Surg 2001;125:221-6. [ Links ]
7. Shoaib T, Soutar DS, MacDonald DG, Camilleri IG, Dunaway DJ, Gray HW, et. al. The accuracy of head and neck carcinoma sentinel node biopsy in the clinically N0 neck. Cancer 2001;91:2077-83. [ Links ]
8. Hyde NC , Prvulovich E, Newman L, Waddington WA, Visvikis D, Ell P. A new approach to pre-treatment assessment of the N0 neck in oral squamous cell carcinoma: the role of sentinel node biopsy and positron emission tomography. Oral Oncol 2003;39:350-60. [ Links ]
9. Ross GL, Soutar DS, MacDonald DG, Shoaib T, Camilleri IG, Robertson AG. Improved staging of cervical metastases in clinically node-negative patients with head and neck squamous cell carcinoma. Ann Surg Oncol 2004;11:213-8. [ Links ]
10. Pastore A, Turetta GD, Tarabini A, Turetta D, Feggi L, Pelucchi S. Sentinel lymph node analysis in squamous carcinoma of the oral cavity and oropharynx. Tumori 2002;88:58-60. [ Links ]
11. Barzan L, Sulfaro S, Alberti F, Politi D, Marus W, Pin M. Gamma probe accuracy in detecting the sentinel lymph node in clinically N0 squamous cell carcinoma of the head and neck. Ann Otol Rhinol Laryngol 2002;111:794-8. [ Links ]
12. Pitman KT, Johnson JT, Brown ML, Myers EN. Sentinel lymph node biopsy in head and neck squamous cell carcinoma. Laryngoscope 2002;112:2101-13. [ Links ]
13. Civantos FJ, Gomez C, Duque C, Pedroso F, Goodwin WJ, Weed DT, et al. Sentinel node biopsy in oral cavity cancer: correlation with PET scan and immunohistochemistry. Head Neck 2003;25:1-9. [ Links ]
14. Kontio R, Leivo I, Leppanen E, Atula T. Sentinel lymph node biopsy in oral cavity squamous cell carcinoma without clinically evident metastasis. Head Neck 2004;26:16-21. [ Links ]
15. Hoft S, Maune S, Muhle C, Brenner W, Czech N, Kampen WU, et al. Sentinel lymph-node biopsy in head and neck. Br J Cancer 2004;91:124-8. [ Links ]
16. Werner JA, , Dunne AA, Ramaswamy A, Dalchow C, Behr T, Moll R, et al. The sentinel node concept in head and neck cancer: solution for the controversies in the N0 neck. Head Neck 2004;26:603-11. [ Links ]
17. Hyde NC, Prvulovich E, Newman L, Waddington WA, Visvikis D, Ell P. A new approach to pre-treatment assessment of the N0 neck in oral squamous cell carcinoma: the role of sentinel node biopsy and positron emission tomography. Oral Oncol 2003;39:350-60. [ Links ]
18. Alex JC. The application of sentinel node radiolocalization to solid tumors of the head and neck: a 10-year experience. Laryngoscope 2004;114:2-19. [ Links ]
19. Moses LE, Shapiro D, Littenberg B. Combining independent studies of a diagnostic test into a summary ROC curve: data-analytic approaches and some additional considerations. Stat Med 1993;12:1293-316. [ Links ]
20. Deeks JJ. Systematic reviews of evaluations of diagnostic and screening tests. En Egger M, Smith GD, Altman DG, eds. Systematic reviews in health care. Meta-analysis in context. Londres: BMJ Books; 2001.p.248-82. [ Links ]
21. Don DM, Anzai Y, Lufkin RB, Calcaterra TC. Evaluation of cervical lymph node metastasis in squamous carcinoma of the head and neck. Laryngoscope 1995;105:669-74. [ Links ]
22. Leemans CR, Tiwari R, Van der Waal I, Karim ABMF, Nauta JP, Snow GB. The efficacy of comprehensive neck dissection with or without postoperative radiotherapy in nodal metastases of squamous cell carcinoma of the upper respiratory and digestive tracts. Laryngoscope1990; 100:1194-8. [ Links ]
23. Weiss MH, Harrison LB, Isaacs RS. Use of decision analysis in planning a management strategy for the stage No neck. Arch Otolaryngol Head Neck Surg 1994;120:699-702. [ Links ]
24. Pillsbury III HC, Clark MA. A rationale for therapy of the No neck. Laryngoscope 1997;107: 1294-315. [ Links ]
25. NCCN practice guidelines for cancer of the head and neck. Version 1. The National Comprehensive Cancer Network. Inc eds. Rockville:2000. [ Links ]
26. Kowalski LP, Magrin J, Waksman G, Santo GF, Lopes ME, de Paula RP, Pereira RN, Torloni H. Supraomohyoid neck dissection in the treatment of head and neck tumors. Survival results in 212 cases. Arch Otolaryngol Head Neck Surg 1993 ;119:958-63. [ Links ]
27. Pitman KT, Johnson JT, Myers EN. Effectiveness of selective neck disection for management of the clinically negative neck. Arch Otolaryngol Head Neck Surg 1997;123:917- 22. [ Links ]
28. Medina JE, Byers RM. Supraomohyoid neck dissection: rationale, indications and surgical technique. Head Neck 1989;11:111-22. [ Links ]
29. Henick DH, Silver CE, Heller KS, Shasha AR, Har El G, Wolk DP. Supraomohyoid neck dissection as a staging procedure for squamous cell carcinomas of the oral cavity and oropharynx. Head Neck 1995;17:119-23. [ Links ]
30. Davidson J, Khan Y, Gilbert R, Birt BD, Balogh J, MacKenzie R. Is selective dissection sufficient treatment for the No/Np+ neck?. J Otolaryngol 1997;26:229-31. [ Links ]
31. Shah JP, Candela FC, Poddar AK. The patterns of cervical lymph node metastases from squamous carcinoma of the oral cavity. Cancer 1990;66:109-13. [ Links ]
32. Shah JP, Andersen PE. The impact of patterns of nodal metastasis on modifications of neck dissection. Ann Surg Oncol 1994;1:521-32. [ Links ]
33. Lyman GH, Giuliano AE, Somerfield MR, Benson AB 3rd, Bodurka DC, Burstein HJ, et. al. American Society of Clinical Oncology. Guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol 2005;23:7703-20. [ Links ]
34. Morton DL, Cochran AJ, Thompson JF, Elashoff R, Essner R, Glass EC et al. Multicenter selective lymphadenectomy trial group. Sentinel node biopsy for early-stage melanoma: accuracy and morbidity in MSLT-I, an international multicenter trial. Ann Surg 2005;242:302-11. [ Links ]
35. Van den Brekel MW, Stel HV, Van der Valk P, Van der Waal I, Meyer CJM, Snow GB. Micrometastasis from squamous cell carcinoma in neck dissection specimens. Eur Arch Otorhinolaryngol 1992;249:349-53. [ Links ]
36. Czerniecki BJ, Scheff AM, Callans LS, Spitz FR, Bedrosian I, Conant EF et al. Inmunohistochemistry with pancytokeratins improves the sensitivity of sentinel lymph node biopsy in patients with breast carcinoma. Cancer 1999;85:1098-103. [ Links ]
37. Ross GL, Soutar DS, Gordon MacDonald D, Shoaib T, Camilleri I, Roberton AG et al. Sentinel node biopsy in head and neck cancer: preliminary results of a multicenter trial. Ann Surg Oncol 2004;11:690-6. [ Links ]
38. Kowalski LP, Bagietto R, Lara JR, Santos RL, Tagawa EK, Santos IR. Factors influencing contralateral lymph node metastasis from oral carcinoma. Head Neck 1999;21:104-10. [ Links ]
39. Byers RM, Weber RS, Andrews T, McGill D, Wolf P. Frequency and therapeutic implications of "skip metastases" in the neck from squamous cell carcinoma of the oral tongue. Head Neck 1997;19:14-9. [ Links ]
40. Woolgar JA. Pathology of the N0 neck. Br J Oral Maxillofac Surg 1999;37:205-9. [ Links ]
41. Schuller DE. An assessment of neck node immunoreactivity in head and neck cancer. Laryngoscope 1984;94:1-35. [ Links ]
42. Schuller DE, Libby DH, Rinehart JJ, Milo GG, Koolemans-Beynen A. Immunomodulation of nodal lymphocytes in head and neck cancer. Arch Otolaryngol 1985;111:465-8. [ Links ]
43. Chu Y, Hu HM, Winter H, Woods WJ, Doran T, Lashley D, et al. Examining the immune response in sentinel lymph nodes of mice and men. Eur J Nucl Med 1999;26:S50-S3. [ Links ]
44. Cochran AJ, Morton DL, Stern S, Lana AM, Essner R, Wen DR. Sentinel lymph nodes show profound downregulation of antigen-presenting cells of the paracortex: implications for tumour biology and treatment. Mod Pathol 2001;14:604-8. [ Links ]
![]() Correspondence:
Correspondence:
Prof. Joseba Santamaría Zuazua
Hospital de Cruces.
Servicio de Cirugía Maxilofacial
Plaza de Cruces s/n ]]>
48903 Barakaldo (Bizkaia)
E-mail: jsz@clinicaimd.com
Received: 28-04-2006
Accepted: 10-12-2006