










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.96 n.4 Madrid Apr. 2004
| ORIGINAL PAPERS |
Topical glyceryl trinitrate in the treatment of anal fissure
F. Novell, F. Novell-Costa and J. Novell
Service of General Surgery. Hospital Clínic. Barcelona. University of Barcelona, Spain
ABSTRACT
Aim: the aim of this study was to assess the effectiveness of topical glyceryl trinitrate (GTN) in the treatment of anal fissure.
Patients: eighty consecutive patients were randomized to receive 0.2% GTN gel twice a day during a minimum of 6 weeks. Of these 80 patients 34 were males and 46 female, with ages be-tween 20 and 78 years. All patients underwent a work-up that included gender, age, symptom duration, site, previous treatment attempts, pain score, associated diseases, and maximum anal resting pressure. These patients were followed at regular intervals of 4, 8, and 12 weeks to assess symptom outcome, rate of healing, adverse effects, and recurrence rate.
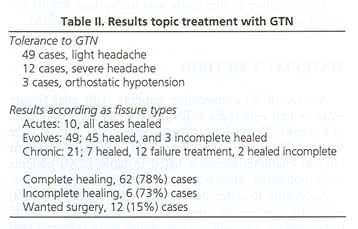
Results: pain scores were significantly reduced during the treatment period in 65% of cases. After 4 weeks, 55% of patients had healed, and 78% after 9 weeks. In 18 patients (22%), anal fissures did not heal even with 6 additional weeks of treatment, and 12 of them (15%) underwent lateral sphincterotomy. Sixty one percent of patients had flushing and 15% severe headaches.
Conclusion: the results of this study have demonstrated the significant benefit of topical GTN when administered to patients suffering from anal fissures.
Key words: Anal fissure. Gliceryl trinitrate. Surgical treatment.
Novell F, Novell-Costa F Novell J. Topical glyceryl trinitrate in the treatment of anal fissure. Rev Esp Enferm Dig 2004; 96: 255-258.
Recibido: 09-06-03.
Aceptado: 22-09-03.
Correspondencia: F. Novell. Mallorca 309, 3º. 08037 Barcelona. Telf.: 93 2074244. Fax: 93 2724831
INTRODUCTION
Until recently, anal fissures were treated with diverse surgical procedures (1,2), like anal dilation and lateral internal sphincterotomy, with the purpose of diminishing the tension at the internal sphincter and to achieve its healing. However, both surgical treatments may cause varying degrees of anal incontinence in nearly 30% of cases. Recent studies have shown that nitric oxide donor derivatives like glyceryl trinitrate (GTN) may reduce the pressure of the sphincter and achieve the healing of the fissure.
The objective of this study was to evaluate results obtained with GTN in the treatment of anal fissure (3-5).
MATERIAL AND METHOD
A total of 80 consecutive patients with anal fissure were treated with 0.2% GTN twice a day for a minimum of 6 weeks. Thirty-four patients were males and 46 were females. Their age ranged from 20 to 78 years, and their clinical characteristics are listed in table I. All patients were monitored on an outpatient basis.
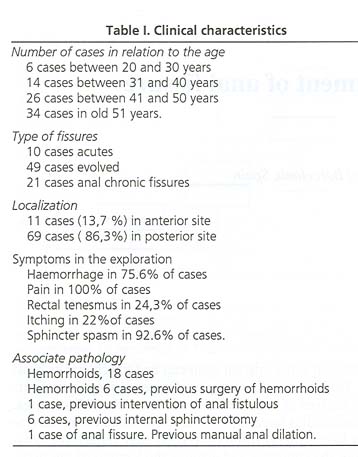
According to outcome, fissures were classified as: a) acute; b) progressive -more than 1 month of evolution, thick borders, and sentry hemorrhoid; and c) chronic anal fissures, evolving through several months with marginal induration, sphincter muscle fiber exposure, great sentry hemorrhoid, and failure of previous treatments.
The pain score was checked using a visual analog scale (VAS) for absent, mild, moderate, severe or maximum pain.
All patients were monitored at regular intervals of 4, 8 and 12 weeks in order to control their symptoms, fissure healing, adverse effects, and potential relapse.
RESULTS
The results of GTN administration are shown in table II.
There were 69 posterior and 11 anterior fissures. Pain severity decreased to mild when evaluated with the VAS at 3 days after treatment onset in 42 patients.
At week 4, 44 patients had achieved a complete healing, and 62 achieved this on the 9th week. GTN treatment failed in 18 patients, 15 with chronic fissures and 3 with progressive fissures. Twelve of these 18 patients subsequently underwent lateral sphincterotomy. Six patients, 5 with chronic fissures and 1 with progressive fissures, who had incomplete healing rejected another treatment because of minor nuisances.
Forty-eight patients had flushing and mild headache after GTN administration. No patient required treatment discontinuation because of adverse effects, despite the fact that 12 subjects had severe headache. Three patients had orthostatic hypotension fol-lowing the first application of GTN.
DISCUSSION
Until recently the treatment of anal fissure was surgical (6,7), but the moderate prevalence of complications such as anal incontinence or abscess has promoted other treatments (8,9), like topical 0.2% GTN (10-13).
GTN is an nitric oxide donor that increases local blood flow, contributes to the relaxation of the internal sphincter, and decreases resting pressure at the anal canal. Its topical application acts like a "chemical sphincterotomy" and is able to cure the fissure.
The evaluation of blood flow at the anal canal has been shown to be increased very significantly in 65% of patients treated with GTN (14), and the pressure at this level decreased by 40% of previous values within 20 minutes following GTN (15,16). This decrease maintained at least for 90 minutes.
In responsive subjects, anal pain usually begins to decrease within 3-5 days of treatment, and healing is achieved between weeks 4 and 9. GTN treatment failure is due to poor GTN gel administration, to the presence of marked fibrosis at the fissure, or to sphincter spasm.
Seventy-six percent of our patients showed flushing and headache (17-19).
When related to age, incidence started from 50 years on. Regarding our patients, 12.5% had acute anal fissures, 61.25% had progressive fissures, and 26.25% had chronic anal fissures. In 40% of treated cases there was some associated anal condition.
In conclusion, these results demonstrate a significant benefit from the topical administration of 0.2% GTN to anal fissures.
REFERENCES
1. Richard CS, Gregoire R, Plewes EA, Silverman R, Burul C, Buie D, et al. Internal sphincterotomy is superior to topical nitroglycerin in the treatment of chronic anal fissure: results of a randomized controlled trial by the Canadian Colorectal Trials Group. Dis Colon Rectum 2000; 43: 1048-57. [ Links ]
2. Nelson RL. Meta-analysis of operative techniques for fissure-in-ano. Dis Colon Rectum 1999; 42: 1424-8. [ Links ]
3. Watson SJ, Kamm MA, Nichols RJ, Phillips RK. Topical glyceryl trinitrate in the treatment of chronic anal fissure. Br J Surg 1996; 83: 771-5. [ Links ]
4. Lund JN, Armitage NC, Scholefield JH. Use of gliceryl trinitrate ointment in the treatment of anal fissure. Br J Surg 1996; 83: 776-7. [ Links ]
5. Palazzo FF, Kapur S, Steward M, Cullen PT. Glyceryl trinitrate of chronic fissure in ano: one year´s experience with 0.5% GTN paste. J R Coll Surg Edinb 2000; 45: 168-70. [ Links ]
6. Christei A, Guest JF. Modelling the economic impact of managing a chronic anal fissure with a proprietary furmulation of nitroglycerin (Rectogesic) compared to lateral internal sphincterotomy in the United Kingdon. Int J Colorectal Dis 2002; 17: 259-67. [ Links ]
7. Libertiny G, Knight JS, Farok R. Randomized trial of topical 0.2% glyceryl tinitrate and lateral internal sphincterotomy for the treatment of patients with chronic anal fissure long-term follow-up. Eur J Surg 2002;1 68: 418-21. [ Links ]
8. Brisinda D, Maria G, Fenici R, Civello IM, Brisinda G. Safety of botulinum neurotoxin treatment in patients with chronic anal fissure. Dis Colon Rectum 2003; 46: 419-20. [ Links ]
9. Madalinski MH, Slawek J. The higher doses of botulinum toxin and the potential effects of its action after nitric oxide donors application for the treatment of chronic anal fissure. Surgery 2003; 133: 455-6. [ Links ]
10. Scholefield JF, Bock JU, Marala B, Richter HJ, Athanasiadis S, Prols M, et al. A dose finding study with 0.1%, 0.2%, and 0.4% glyceryl trinitrate ointment in patients with chronic anal fissures. Gut 2003; 52: 264-9. [ Links ]
11. Svendsen CB, Matzen P. Treatment of chronic anal fissure with topically applied nitroglycerin ointment. A systematic reviwe of evidence- based results. Ugeskr Laeger 2002; 164: 3845-9. [ Links ]
12. Graziano A, Svider L, Lencinas S, Masacangiol G, Gualdrini U, Bisisio O. Long -term results of topical nitroglycerin in the treatment of chronic anal fissures are disappointing. Tech Coloproctol 2001; 5: 143-7. [ Links ]
13. Kua KB, Kocher HM, Kelkar A, Patel AG. Effect of topical glyceryl tinitrate on anodermal blood flow in patients with chronic anal fissures. ANZ J Surg 2001; 71: 548-50. [ Links ]
14. Jonas M, Amin S, Wright JW, Neal KR, Scholefield JH. Topical 0.2 percent glyceril trinitrate ointment has a short-lived effect on resting anal pressure. Dis Colon Rectum 2001; 44: 1640-3. [ Links ]
15. Pitt J, Williams S, Dawson PM. Reasons failure of glyceryl trinitrate treatment of chronic fissure-in-ano: a multivariate analysis. Dis Colon rectum 2001; 46: 846-7. [ Links ]
16. Moorthy K, Chavez R. Audit of topical glyceryl trinitrate for treatment of fissure-in-ano. Ann R Coll Surg Engl 2001; 83: 220-1. [ Links ]
17. Ward DI, Miller BJ, Schache DJ, Cohen JR, Theile DE. Cut or paste? The use of glyceryl trinitrate paste in the treatment of acute and chronic anal fissure. Aust N Z J Surg 2000; 70: 19-21. [ Links ]
18. Hasegawa H, Radley S, Morton DG, Dorricott NJ, Campbell DJ, Keighley MR. Audit of topical glyceryl trinitrate for treatment of fissure-in-ano. Ann R Coll Surg Engl 2000; 82: 27-30. [ Links ]
19. Mc Leod RS, Evans J. Symptomatic care and nitroglycerin in the management of anal fissure. J Gastrointest Surg 2002; 6: 278-80. [ Links ]

