










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.1 Madrid Jan. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Superior mesenteric artery syndrome: an uncommon cause of intestinal obstruction
Síndrome de la arteria mesentérica superior: una causa infrecuente de obstrucción intestinal
José Barquín-Yagüez, Pedro Abadía-Barno and Juan Carlos García-Pérez
General and Digestive Surgery Department. Hospital Universitario Ramón y Cajal. Madrid, Spain
Introduction
Superior mesenteric artery (SMA) syndrome or Wilkie's syndrome is an uncommon cause of intestinal obstruction resulting from compression of the third portion of the duodenum when passing between the SMA and the aorta when the angle between the latter structures becomes smaller.
Etiologies include significant and fast weight loss as seen in patients with cancer, bariatric or other major surgery, severe burns, dementia, or advanced eating disorders.
Clinically, it may manifest with acute or chronic upper intestinal obstruction symptoms.
Diagnosis is primarily based on abdominal computed tomography (CT) scans with oral and intravenous contrast, which reveals a reduced angle (< 25o) and distance (< 8-10 mm) between the aorta and SMA with upstream gastroduodenal dilation. Under normal conditions, the above measurements are 38o - 65o and 10-28 mm, respectively.
Conservative management with decompression using a nasogastric tube and adequate nutritional support is initially recommended. Surgical duodenojejunostomy is indicated for failed conservative management. Percutaneous endoscopic jejunostomy has been posited as potential therapy as it may modify the aorta-SMA angle and provide in addition a feeding method.
Case report
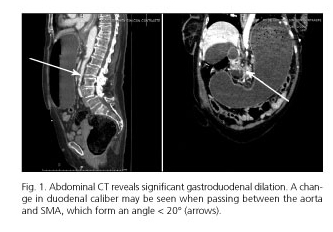
We report the case of a 75-year-old woman with Parkinson's disease and severe dementia who presents at the ER for oral intolerance and vomiting for one week, associated with a weight loss of 35 kg during the past year. Examination reveals a distended tympanic abdomen with tenderness in the epigastrium. CT shows significant dilation in the stomach and both the first and second duodenal portions, with caliber reduction in the duodenum when passing between the aorta and SMA (which form an angle < 20o), suggestive of aortomesenteric clamp. Treatment with NGT and total parenteral nutrition is started, which resulted in complete remission and discharge from hospital after 10 days.
References
1. Coşkun A, Uçar D, Carti EB, et al. Wilkie's syndrome: A rare cause of vomiting and weight loss. Int J Case Rep Imag 2013;5:150-4. DOI: 10.5348/ijcri-2014-02-461-CR-13. [ Links ]
2. Roy A, Gisel JJ, Roy V, et al. Superior mesenteric artery (Wilkie's) syndrome as a result of cardiac cachexia. J Gen Intern Med 2005;20:C3-4. DOI: 10.1007/s11606-005-0237-7. [ Links ]
3. Rosa-Jiménez F, Rodríguez González FJ, Puente Gutiérrez JJ, et al. Duodenal compression caused by superior mesenteric artery: Study of 10 patients. Rev Esp Enferm Dig 2003;95:485-9,480-4. [ Links ]
