










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.3 Madrid mar. 2014
LETTERS TO THE EDITOR
Fever and acute cytomegalovirus hepatitis in Crohn's disease
Fiebre y hepatitis aguda por citomegalovirus en enfermedad de Crohn
Key words: Cytomegalovirus. Hepatitis. Crohn's disease. Ulcerative colitis.
Palabras clave: Citomegalovirus. Hepatitis. Enfermedad de Crohn. Colitis ulcerosa.
Dear Editor,
The control of inflammatory bowel disease (IBD) is complex. Immunomodulatory therapies causes situations of immunosuppression and increases susceptibility to opportunistic infections. We report a case of acute hepatitis and Crohn's disease with prolonged fever in the context of a cytomegalovirus (CMV) primo-infection.
Case report
We present a 33-year-old male patient with ileal Crohn's disease on maintenance treatment with 6-mercaptopurine. The patient went to the emergency department because of fever, fatigue and increased serum transaminase levels. The physical examination was unremarkable. An abdominal CT scan with intravenous contrast showed inflammation of the ileum however, all other tests ruled out other sources of infection.
Funduscopy was normal and lumbar puncture was not possible due to patient's scoliosis. The patient received empirical treatment with ceftriaxone without improvement.
Serology for herpes, Epstein Barr virus, Coxiella, Legionella, HIV, Lues, Brucella, ag galactomanann, QuantiFERON, stool cultures and Clostridium toxine were negative. The CMV IgM was positive as the blood polymerase chain reaction (PCR) tests.
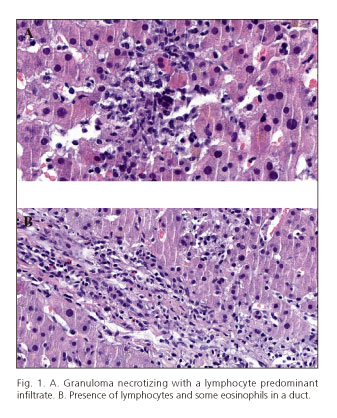
Before starting treatment with ganciclovir, liver biopsy was performed observing a lymphocyte-predominant infiltrate and necrosis of the limiting plate with some granuloma necrotizing and virus isolation by immunohistochemical techniques (Fig. 1).
The patient was discharged after 21 days of treatment with a diagnosis of acute CMV hepatitis receiving additional valacyclovir for a week without relapse.
Discussion
CMV incidence in patients with IBD ranges from 0.53 % to 3.4 % increase if receiving immunosuppressive agents (1-3).
The prevalence in Crohn's disease is low, whereas in ulcerative colitis (UC) it can rise up to 70 % (4,5).
The affinity of the virus in tissues and the high seroprevalence suggest that the virus plays only an incidental role. However, it has proven to be a pathogen in 20-30 % rate of severe steroid- refractory IBD.
The first case of UC and CMV was described by Powell et al. in 1961 (6). Most are due to reactivation of a latent infection. The presentation of the disease as an acute mononucleosis as in our case is rare (2,7).
CMV infection occurs in steroid-refractory UC, but were not the case in our patient who had a Crohn's disease and had not received corticosteroids although he was an immunocompromised patient due to treatment with mercaptopurine (8).
The diagnosis is based on histological techniques, as other methods do not differentiate between a latent colonization and active infection (9,10). Another technique is PCR in intestinal tissue or blood. Immunohistochemistry (IHC) is the standard diagnostic technique.
Clinical guidelines stipulate that the diagnosis should include PCR (without defining whether blood or colonic mucosa) and colon IHC.
Ganciclovir is the treatment of choice in severe steroid-refractory UC. However, other studies have reported improvement without antiviral treatment.
In our case, without intestinal involvement but with a primo-infection hepatitis by CMV, antiviral treatment was chosen with excellent response.
In conclusion, we present an atypical case of acute CMV hepatitis in a patient with a corticosteroid-free treated Crohn's disease, without intestinal involvement and favorable outcome after antiviral therapy.
Cristina Pisabarros-Blanco1, Mónica Sierra-Ausin1,
Pedro Linares-Torres1 and M.a Concepción Álvarez-Cañas2
Departments of 1Digestive Diseases and 2Pathology. Hospital de León. León, Spain
References
1. Vega R, Bertran X, Menacho M. Cytomegalovirus infection in patients with inflammatory bowel disease. Am J Gastroenterol 1999;94:1053-6. [ Links ]
2. Papadakis KA, Tung JK, Binder SW. Outcome of cytomegalovirus infections in patients with inflammatory bowel disease. Am J Gastroenterol 2001;96:2137-42. [ Links ]
3. Hamlin PJ, Shah MN, Scott N, Wyatt JI, Howdle PD. Systemic cytomegalovirus infection complicating ulcerative colitis: A case report and review of the literature. Postgrad Med J 2004;80:233-5. [ Links ]
4. Hommes DW, Sterringa G, Boom R. Incidence and outcome of cytomegalovirus infection in patients with inflammatory bowel disease. Gastroenterology 2002;122: A1287. [ Links ]
5. D'Ovidio V, Vernia P, Gentile G, Capobianchi A, Marcheggiano A, Viscido A, et al. Cytomegalovirus infection in inflammatory bowel disease patients undergoing anti-TNFalpha therapy. J Clin Virol 2008;43:180-3. [ Links ]
6. Powell RD, Warner NE, Levine RS, Kirsner JB. Cytomegalic inclusion disease and ulcerative colitis; report of a case in ayoung adult. Am J Med 1961;30:334-40. [ Links ]
7. Babyatsky MW, Keroack MD, Blake MA, Rosenberg ES, Mino-Kenudson M. Case records of the Massachusetts General Hospital.Case 35-2007. A 30-year-old man with inflammatory bowel diseaseand recent onset of fever and bloody diarrhea. N Engl J Med 2007;357:2068-76. [ Links ]
8. Osaki R, Andoh A, Tsujikawa T, Ogawa A, Koizumi Y, Nakahara T, et al. Acute cytomegalovirus infection superimposed on corticosteroid-naïve ulcerative colitis. Inter Med 2008;47:1341-4. [ Links ]
9. Lawlor G, Moss AC. Cytomegalovirus in inflammatory bowel disease: Pathogen or innocent bystander? Inflamm Bowel Dis 2010;16:1620-7. [ Links ]
10. Garrido E, Carrera E, Manzano R, López-Sanromán A. Clinical significance of cytomegalovirus infection in patients with inflammatory bowel disease. World J Gastroenterol 2013;19:17-25. [ Links ]

