










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAnales de Psicología
On-line version ISSN 1695-2294Print version ISSN 0212-9728
Anal. Psicol. vol.32 n.2 Murcia May. 2016
https://dx.doi.org/10.6018/analesps.32.2.215251
Beliefs about obesity and their relationship with dietary restriction and body image perception
Creencias sobre las causas de la obesidad y su relación con la restricción alimentaria y la percepción de la imagen corporal
Alejandro Magallares1, Rocio Carbonero-Carreño2, Inmaculada Ruiz-Prieto3 and Ignacio Jauregui-Lobera4
1 School of Psychology. Social Psychology Department, Universidad Nacional de Educación a Distancia (UNED). Madrid (Spain).
2 IES Atenea. Mairena del Aljarafe (Sevilla).
3 Behavioural Sciences Institute. Sevilla (Spain).
4 School of Experimental Sciences. Nutrition and Bromatology. Universidad Pablo de Olavide. Sevilla (Spain).
ABSTRACT
The reviewed literature provides evidence that beliefs about the causes of obesity may actually have an influence on eating habits. In this work we wanted to analyze the relationship that may exists between beliefs about obesity, dietary restraint and body image perception. For that purpose, 258 female and male students of a High School and Occupational Training School in Seville (Spain) were recruited to conduct the study. According to our results, it was found that beliefs about obesity were positively related with dietary restraint and body image perception. Additionally, it was found that people high in beliefs about the controllability of the weight scored more in dietary restraint and body image perception than participants that did not believe that obesity was under personal control. No differences were found in Body Mass Index. Finally, it is suggested, according to the results that we found, that in order to be effective, public health campaigns may need to target people's beliefs just as much as they target their behaviours.
Key words: beliefs about the causes of obesity; dietary restraint; body image perception; Body Mass Index.
RESUMEN
La literatura revisada pone de manifiesto que las creencias sobre las causas de la obesidad tienen una influencia sobre el comportamiento alimentario. En este trabajo queríamos analizar la relación que puede existir entre creencias sobre la obesidad, la restricción alimentaria y la percepción de la imagen corporal. Con ese objetivo, 258 estudiantes, tanto hombres como mujeres, de un Instituto y centro de Formación Profesional de Sevilla (España) fueron reclutados para hacer el estudio. De acuerdo a los resultados obtenidos, se ha encontrado que las creencias sobre la obesidad estaban positivamente relacionadas con la restricción alimentaria y la percepción de la imagen corporal. Adicionalmente, se halló que la gente alta en creencias sobre la obesidad puntuaba más en restricción alimentaria y percepción de la imagen corporal que aquellos participantes que no creían que la obesidad estuviera bajo control personal. No se encontraron diferencias para el Índice de Masa Corporal. Finalmente se sugiere, en función de los resultados obtenidos, que para incrementar la efectividad de las campañas de salud sería necesario intervenir no solo sobre los comportamientos sino también sobre las creencias.
Palabras clave: creencias sobre las causas de la obesidad; restricción alimentaria; percepción de la imagen corporal; Índice de Masa Corporal.
Introduction
An increasing number of people are facing the burden of obesity, which is defined as an excess amount of body fat and it is determined by a Body Mass Index (BMI) of ≥ 30 kg/m2 (Haslam & James, 2005). Obesity is an important risk factor for other morbidities, such as type II diabetes, hypertension, coronary artery disease, and reduces life expectancy (see for a review: Guh et al., 2009). The causes of obesity are as varied as the people it affects. Many factors influence an excessive BMI such as genes (Yang, Kelly, & He, 2007), a sedentary lifestyle that includes poor diets, too much television watching and too little physical activity (see for a metaanalysis: Wilmot et al., 2012) and what is called the obesogenic environment (see for a review: Mackenbach et al., 2014). In Spain, the country where this studio has been conducted, people are not very familiar with factors influencing obesity (Martinez-Gonzalez, Martin-Almendros, Gibney, Kearney, & Martinez, 1999).
The reviewed literature has showed that the beliefs that people have about which are the causes of obesity may be related with their BMI (McFerran & Mukhopadhyay, 2013). According to these authors, whether a person believes obesity is caused by overeating or by a lack of exercise predicts his or her actual BMI. For example, they found that people who implicated diet as the primary cause of obesity actually had lower BMIs than those who implicated lack of exercise. These findings provide evidence that beliefs about obesity may actually have an influence on eating habits. In this line of thinking, there are other studies that have found similar results. For example, it has been suggested that individuals' food and exercise choices may be influenced by the beliefs that people have (Burnette, 2010). This author found that individuals were especially unlikely to self-regulate effectively after dieting setbacks when they believed body weight must be fixed rather than malleable (Burnette, 2010). Additionally, it has been suggested that fostering the belief that body weight is changeable helps people to avoid setback related weight-gain (Burnette & Finkel, 2012). Finally, a recent study has showed that participants who received information about the obesogenic environment, in order to change their beliefs about the causes of obesity, reported greater self-efficacy to lose weight (pearl & Lebowitz, 2014). For all these reasons, we believe it would be interesting to continue the study of the effects that may be having the beliefs about which are the causes of obesity on eating behavior. Therefore, the goal of this work is to analyze if beliefs about obesity are linked or not with dietary restraint and body image perception.
Dietary restriction is defined as a reduction of nutrient intake without causing malnutrition (Lowe & Timko, 2004) and dietary restraint is the cognitive intention to limit dietary intake (Stice, Fisher, & Lowe, 2004). Body image perception may be defined as a person's perceptions, thoughts, and feelings about his or her body (Grogan, 2008). It is important to remark that BMI and body image perception do not have a perfect and positive correlation, which means that people do not perceive themselves with the weight they really have and sometimes individuals think that they have more weight than they actually have (Mikolajczyk et al., 2010). Both variables, dietary restraint and body image perception, are related with eating disorders (Lawson, 2012) and obesity (Mussell et al., 1996). We believe that it is especially interesting to analyze the relationship that may exist between these two variables and beliefs about obesity, because recent studies suggest that eating concerns may be related with the way people perceive obese individuals. For example, some authors have found that the perception that normal weight populations and patients with eating disorders have about obese people are different (Magallares, Jauregui-Lobera, Ruiz-Prieto, & Santed, 2013) . According to these authors, eating disorders patients had a more negative perception of obese people than normal weight individuals. Additionally, it has been found that women in risk to develop eating disorders had worse attitudes toward obese people compared with women without eating concerns (Magallares, 2012). Finally, some authors have showed that there was an association between weight satisfaction and negative attitudes toward obese individuals among people with normal weight (Hansson & Rasmussen, 2014) . All these studies suggest that eating concerns and BMI may be related with the perception that we have about obese individuals. In this line of thinking, some authors suggest that body image and dietary restraint are risk factors for obesity (Megalakaki, Mouveaux, Hubin-Gayte, & Wypych, 2013). For all these reasons, we believe that it is necessary to conduct a study to analyze if beliefs about obesity are linked or not with eating concern variables, like dietary restraint and body image perception.
To summarize, it is expected that beliefs about the controllability of weight may be related to dietary restraint and body image perception. According to the reviewed literature, it is expected that beliefs that obesity is under personal control will be related with a lower BMI and, therefore, with more dietary restraint (McFerran & Mukhopadhyay, 2013). Additionally, it is expected that beliefs about the controllability of weight will be related with a perception of a heavier body image (Mikolajczyk et al., 2010), as the studies that have found that people who believe obesity is under personal control are more likely to be aware of other people's weight may suggest (Teachman, Gapinski, Brownell, Rawlins, & Jeyaram, 2003). Furthermore, gender differences will be tested with the variables of our sample, as studies about the prevalence of obesity conducted in Spain suggest (Gutierrez-Fisac et al., 2012).
Method
Participants
The convenience sample comprised of 258 Spanish students of the High School and Occupational Training School Atenea (IES Atenea) in Seville (Spain) from 12 to 28 years (age: M = 17.38, SD = 3.81). 107 were female and 151 were male. 28 participants were underweight (BMI ≤ 18 kg/m2), 160 were normal weight (BMI Range18-25 kg/m2), and 70 were overweight (BMI ≥ 25 kg/m2). 141 participants were under legal age and 117 were adults.
Procedure
Before conducting the study, the project was approved by the director of the Behavioral Sciences Institute. Thereafter the project was transferred to the Director of the IES Atenea, who, after accepting it, submitted that project to the students' council, the academic staff and the students' fathers and mothers association thus obtaining the approval by all of them. Once this approval was obtained, a timetable was established to collect the data during a week thus avoiding evaluation periods, in which the possible distress could have influenced the study.
In order not to alter the routines of the classes in the Centre, the questionnaires were filled in during the periods assigning to tutoring and the anthropometric measures were collected in hours devoted to physical education. All students were invited to participate, this participation being completely voluntary. Participation rate was 94%. For the participants under legal age the parents' informed consent was compulsory. No exclusion criteria were established.
Measurements were taken individually and participants were instructed in detail about how to complete the questionnaires. In addition, a professional (nutritionist or psychologist) was in charge to resolve any doubts about the tasks when carrying out them. None of the participants received any kind of recompense for participate and anonymity was guaranteed.
Weight and height were taken in individual sessions, with the participants in the standing position, barefoot, and in light garments.
Instruments
To measure beliefs about the causes of obesity the Beliefs About Obese Persons Scale (BAOP) (English and Spanish versions: Allison, Basile, & Yuker, 1991) was used. BAOP measures beliefs about the causes of obesity with an eight-item Likert rating scale (from 1, strongly disagree, to 7, strongly agreed). An example is "Most obese people cause their problem by not getting enough exercise". A score was computed by averaging the 8 items of the scale. The coefficient alpha was .76. Higher scores on this measure reflect greater beliefs that obesity is under personal control.
To measure dietary restraint the cognitive restraint of eating subscale of the Three-Factor Fating Questionnaire-R18 (TFEQ) was used (English version: Stunkard & Messick, 1985; Spanish version: Jauregui-Lobera, Garcia-Cruz, Carbonero-Carreño, Magallares, & Ruiz-Prieto, 2014). This subscale comprises of 6 items on a 4-point response scale (definitely true -1-, mostly true -2-, mostly false -3-, definitely false -4-). It has an adequate internal consistency reliability coefficient (.74). An example of cognitive restraint of eating is "I consciously hold back at meals in order not to gain weight". A score was computed by averaging the 6 items of the cognitive restraint of eating subscale. Higher scores on this measure reflect greater dietary restraint.
To measure body image perception the Stunkard Scale (English version: Collins, 1991; Stunkard & Stellar, 1990; Spanish version: Marrodan et al., 2008) was used. This silhouettes scale consists of a series of images of progressively heavier body types labeled from 1(BMI 17 kg/m2) to 9 (BMI 33 kg/m2). Collins (1991) developed a series of figure drawings incorporating both child and adult figures, male and female. It is mainly used in research to measure body image perception. Participants are asked to choose the silhouette that most closely resembles how they look. Higher scores on this measure reflect that participants perceive they have a higher BMI.
BMI was calculated as the relationship between weight (kg) and height squared (m).
Apparatus
A stadiometer (Atlántida S13; Básculas y Balanzas Añó-Sayol, Barcelona, Spain) was used to measure height and weight of the participants.
Data analysis
First of all, Pearson's correlations were calculated among all the variables of the study.
Then, Student's t tests were calculated with participants with low and high scores on the BAOP scale. The groups of participants were formed by categorizing those individuals with the higher and lower scores on the BAOP scale (50% upper and 50% below) as groups with beliefs that obesity is under personal control and without that belief respectively. Comparisons between these two groups on all the variables of the study (dietary restraint, body image perception and BMI) were made by means of the t test. To test if the groups were correctly formed, the mean scores on the classification variable (BAOP) were analyzed with a t test. This process of categorization a continuous variable has been made following the recommendations of experts in the field (preacher, Rucker, MacCallum, & Nicewander, 2005). Cohen's ds (Cohen, 1988) were also calculated as indices of effect size. Cohen (1988) defined d as the difference between means divided by standard deviation of either group. According to this author, ds ≥ .2 are considered medium effect sizes and ds ≥ .8 large effect sizes.
Finally, Student's t tests were calculated to estimate if there were sex differences in the variables of our study. Additionally, it was calculated a Multiple Analysis of Variance (MANOVA) with sex (man and women) and BAOP (control and no control) as the factors and the rest of the variables of the study as dependent variables to test if there was an interaction between these two independent variables.
The SPSS 19. (SPSS 19.0, SPSS Inc, Chicago, IL) was used to conduct all the analyses.
Results
First of all, we calculated Pearson correlations among the different scales of the study. As shown in Table 1, positive, significant correlations were found between beliefs about the causes of obesity and dietary restraint and body image perception. Additionally, BMI was not related with beliefs about the causes of obesity. Finally, it was found that dietary restraint was positively correlated with body image perception and BMI, and that body image and BMI were highly correlated between each other.

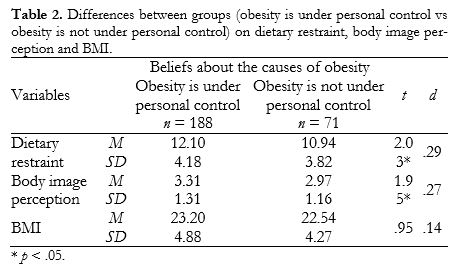
Then, Student's t tests were calculated with beliefs about the causes of obesity as the independent variable (two groups: obesity is under personal control vs obesity is not under personal control) and dietary restraint, body image perception and BMI as dependent variables. These groups were correctly formed, given that the mean scores on classification variable (BAOP) were significantly different between groups [obesity is under personal control = 5.11 vs. obesity is not under personal control = 3.29, t= 18.57, p <. 01; d = 2.59]. After this verification, the rest of the t tests were calculated (see Table 2). The results showed that participants with higher scores in the beliefs about the causes of obesity scale reported more dietary restraint and perceived themselves with more weight than participants with lower scores in the classification scale. Additionally, it was found that there were no differences in the case of BMI for the two groups. The t test revealed that the differences were statistically significant in the case of dietary restraint and body image perception. The size effects found are medium according to the Cohen (1988) criterion.
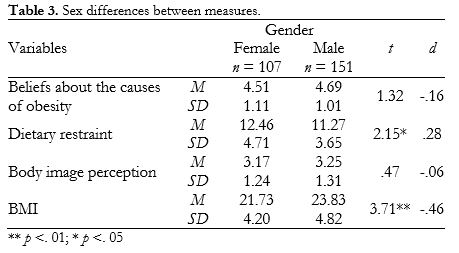
Finally, t tests were estimated with all the variables of the study to see if there were sex differences. As it can be seen in Table 3, there were no differences in the case of beliefs about obesity and body image perception. However, we found significant differences in the case of BMI and dietary restraint. For this reason, a MANOVA was conducted with sex and beliefs about the causes of obesity as the independent variables (two levels) and BMI and dietary restraint as the dependent variables. According to the results that we found, there was no interaction effect for both BMI (F = .01, p > .05) and dietary restraint (F = .26,p > .05).
Discussion
It was found a positive and significant correlation between beliefs about the controllability of weight and dietary restraint and body image perception, as expected. This result suggests that beliefs about the causes of obesity may have a role in explaining some eating concern variables, such as dietary restraint and body image perception. It is important to remark that both variables are related with the apparition and/or maintenance of eating disorders (Lawson, 2012) and obesity (Mussell et al., 1996).
Additionally, it was found that participants with higher scores in the scale to measure if obesity is under personal control reported more dietary restraint and perceived themselves with more weight than participants with lower scores in the beliefs about obesity scale. The size effects found are medium according to the Cohen criterion (1988). These results suggest that participants of our sample who believe that obesity is under personal control avoid to eat certain things in order to not become obese and at the same time they perceive themselves with more overweight than subjects who do not believe that weight can be controlled trough diet and exercise. Given the cross-sectional nature of the study, data prohibit us from making a strong causal claim, but the direction we propose seems more plausible than the reverse. For example, it has been found that women with eating disorders usually perceive themselves to be fatter than they actually are (Garfinkel, 1995). Future studies should address the relationship that may exist between beliefs about the controllability of weight and other eating disorders variables.
It is important to remark that we have not found that BMI was related with beliefs about obesity. This is an unexpected result because recently some authors have showed in their work that beliefs about the causes of obesity were a good predictor of BMI (McFerran & Mukhopadhyay, 2013). However, we have found that although these beliefs are not related with weight itself, they are linked with body image perception. In other words, to believe that obesity is under personal control is not related with people's current weight but it affects the way they perceive themselves, as it was pointed in the last paragraph. Additionally, these beliefs are related in a positive way with dietary restraint. Interestingly, it has been found that dietary restraint may lead to restriction, but at the same time it has been showed in several investigations that many individuals who restrain fail to restrict (Slice et al., 2004) and that restraint is a poor predictor of restriction (Slice, Cooper, Schoeller, Tappe, & Lowe, 2007). Finally, we would like to add that the measurement of beliefs about the causes of obesity was made in a different way in our study (McFerran & Mukhopadhyay, 2013). These authors measured beliefs about obesity not with a scale, as we did with the BAOP, but with some questions that they developed by their own.
The finding of the significant correlation between BMI, body image perception and dietary restraint is congruent with the reviewed literature (Hernandez-Cortes & Londono-Perez, 2013).
Additionally, we found sex differences in BMI and dietary restraint. This is an expected result, because usually women are slimmer than men (Ramos-Valverde, Rivera de los Santos, & Moreno-Rodriguez, 2010) and their scores on dietary restraint scales are higher compared to males (Snoek, Van Strien, Janssens, & Engels, 2008).
These findings suggest that, in order to be effective, public health campaigns may need to target people's beliefs just as much as they target their behaviours (McFerran & Mukhopadhyay, 2013). In other words, it is not only important to promote healthy behaviours, as diet and exercise, but also to give information about which are the causes of obesity, because as we have seen these beliefs may be related with eating habits. For example, it has been showed that beliefs interventions with obesity relapse prevention programs are very useful to provide people a tool to control their own weight (Burnette & Finkel, 2012). Recently, some authors have suggested that emphasising the role of the food environment in causing obesity may promote health behaviours without imposing the negative consequences associated with the beliefs about obesity is under personal control (pearl & Lebowitz, 2014). For example, it has been found that only the belief that obesity is caused by external causes was associated with support for government policies to prevent and treat overweight which gives an idea about how obese people are blamed by Society about their condition (Beeken & Wardle, 2013). Finally, in a more individual level, it is also important to remark that it has been suggested that to assess individuals' beliefs about the causes of obesity when following a diet is a very important issue (Barberia, Attree, & Todd, 2008). According to these authors, the evaluation of these beliefs could lead to more effective diet behaviour-change interventions.
The current study is subject to some limitations that deserve mention. In the first place, it is a cross-sectional study. We believe that longitudinal and experimental studies are needed to confirm some of the patterns presented here. In the second place, the present study utilized self-report measures and could be enhanced with the inclusion of more objective criteria. In the third place, future studies should include dietary restriction measures. In the fourth place, the correlations that we have found are significant but not very high. Finally, the size of the sample could be increased. Despite these limitations, the study provides new data with potential applications.
These limitations considered, the current study offers new directions for the study of the relationship between beliefs about the causes of obesity and eating concerns.
This study presents some contributions with respect to the previous literature. As far as we know, this is the first time that beliefs about the causes of obesity have been analyzed with some relevant variables related to eating concerns, such as dietary restraint and body image perception. We believe that this article enriches and extends the field of eating concerns, as it provides a series of approaches that have not been taken into account before.
References
1. Allison, D.B., Basile, V.C., & Yuker, Y.E. (1991). The measurement of attitudes toward and beliefs about obese persons. International Journal of Eating Disorders, 10, 599-607. DOI: 10.1002/1098-108X(199109)10:5<599::AID-EAT2260100512>3.0.C0;2-#. [ Links ]
2. Barberia, A.M., Attree, M., & Todd, C. (2008). Understanding eating behaviours in Spanish women enrolled in a weight-loss treatment. Journal of Clinical Nursing 17, 957-966. DOI: 10.1111/j.1365-2702.2007.02073.x. [ Links ]
3. Beeken, R.J. & Wardle (2013). Public beliefs about the causes of obesity and attitudes towards policy initiatives in Great Britain. Public Health Nutrition, 16, 2132-2137. DOI: 10.1017/S1368980013001821. [ Links ]
4. Burnette, J. L. (2010). Implicit theories of body weight: Entity beliefs can weigh you down. Personality and Social Psychology Bulletin, 36, 410-422. DOI: 10.1177/0146167209359768. [ Links ]
5. Burnette, J. L. & Finkel, E. (2012). Buffering against weight gain following dieting setbacks: An implicit theory intervention. Journal of Experimental Social Psychology, 48, 721-725. DOI: 10.1016/j.jesp.2011.12.020. [ Links ]
6. Cohen, J. (1988). Statistical power analysis for the behavior sciences. New York: Lawrence Earlbaum Associates. [ Links ]
7. Collins, M.E. (1991). Body figure perceptions and preferences among preadolescent children. International Journal of Eating Disorders, 10, 199-208. DOI: 10.1002/1098-108X(199103)10:2<199::AID-EAT2260100209>3.0.CO;2-D. [ Links ]
8. Garfinkel, P.E. (1995). Eating disorders. In H.I. Kaplan & B.J. Sadock (eds.), Comprehensive Textbook of Psychiatry (pp 1361-1371). Baltimore: Williams & Wilkins. [ Links ]
9. Grogan, S. (2008). Body image: understanding body dissatisfaction in men, women, and children. East Sussex: Routledge. [ Links ]
10. Guh, D.P., Zhang, W., Bansback, N., Amarsi, Z., Birmingham, C.L., & Anis, A.H. (2009). The incidence of comorbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health , 9, 88. DOI: 10.1186/1471-2458-9-88. [ Links ]
11. Gutierrez-Fisac, J. L., Guallar-Castillon, P., Leon-Muñoz, L. M., Graciani, A., Banegas, J. R., & Rodriguez-Artalejo, F. (2012). Prevalence of general and abdominal obesity in the adult population of Spain, 2008-2010: The ENRICA study. Obesity Review, 13, 388-392. DOI: j.1467-789X.2011.00964.x. [ Links ]
12. Hansson, L.M. & Rasmussen, F. (2014). Attitudes towards obesity in the Swedish general population: the role of one's own body size, weight satisfaction, and controllability beliefs about obesity. Body Image, 11, 43-50. DOI: 10.1016/j.bodyim.2013.10.004. [ Links ]
13. Haslam, D.W. & James, W. P. (2005). Obesity. Lancet, 366, 1197-1209. DOI:10.1016/S0140-6736(05)67483-1. [ Links ]
14. Hernández-Cortés, L.M. & Londoño-Pérez, C. (2013). Imagen corporal, IMC, aprontamiento, depresión y riesgo de TCA en jóvenes universitarios (Body Image, CMI, coping, depression and BED risk in young univesitaries). Anales de Psicología, 29, 748-761. DOI:10.6018/analesps.29.3.175711. [ Links ]
15. Jauregui-Lobera, I., Garcia-Cruz, P., Carbonero-Carreño, R., Magallares, A., & Ruiz-Prieto. I. (2014). Psychometric properties of Spanish version of the Three-Factor Eating Questionnaire (TFEQ-SP) and its relationship with some eating- and body image-related variables. Nutrients, 6, 5619-5635. DOI:10.3390/nu6125619. [ Links ]
16. Lawson, V. (2012). Appearance concerns, dietary restriction, and disordered eating. In N. Rumsey & D. Harcourt (eds.), The Oxford handbook of the psychology of appearance (pp. 320-329). New York: Oxford University Press. [ Links ]
17. Lowe, M.R. & Timko, C.A. (2004). What a difference a diet makes: Towards an understanding of differences between restrained dieters and restrained nondieters. Eating Behaviors, 5, 199-208. DOI: 10.1016/j.eatbeh.2004.01.006. [ Links ]
18. Mackenbach, J., Rutter, H., Compernolle, S., Glonti, K., Oppert, J.M., ... & Lakerveld, J. (2014). Obesogenic environments: a systematic review of the association between the physical environment and adult weight status, the SPOTLIGHT project. BMC Public Health, 14, 233. DOI:10.1186/1471-2458-14-233. [ Links ]
19. Magallares, A., Jauregui-Lobera, I., Ruiz-Prieto, I., & Santed, M.A. (2013). Antifat attitudes in a sample of women with eating disorders. Nutricion hospitalaria, 28, 649-653. DOI: 10.3305/nh.2013.28.3.6383. [ Links ]
20. Magallares, A. (2012). Well-being and prejudice toward obese people in women in risk to develop eating disorders. Spanish Journal of Psychology, 15, 1293-1302. DOI: 10.5209/rev_SJOP.2012.v15.n3.39415. [ Links ]
21. Marrodan, V., Montero, M. S., Mesa, J. L., Pacheco, M., Gonzalez, I., ... & Carmenate, M. (2008). Realidad, percepción y atractivo de la imagen corporal: condicionantes biologicos y socioculturales (Reality, perception and attractiveness of the body image: biological and socio-cultural conditions). Zainak, Cuadernos de Antropología-Etnografía, 30, 15-28. [ Links ]
22. Martínez-González, M.A., Martín-Almendros, M.I., Gibney, M.J., Kearney, J.M. & Martínez, J.A. (1999). Perceptions about body weight and weight reduction in Spain. Public Health Nutrition, 2, 557-563. DOI: 10.1017/S1368980099000749. [ Links ]
23. McFerran, B. & Mukhopadhyay, A. (2013). Lay Theories of Obesity Predict Actual Body Mass. Psychological Science, 24, 1428-1436. DOI: 10.1177/0956797612473121. [ Links ]
24. Megalakaki, O., Mouveaux, M., Hubin-Gayte, M., & Wypych, L. (2013). Body image and cognitive restraint are risk factors for obesity in French adolescents. Eating and Weight Disorders, 18, 289-295. DOI: 10.1007/s40519-013-0027-x. [ Links ]
25. Mikolajczyk, R., Maxwell, A., El Ansari, W., Stock, Petkeviciene, J., & Guillen-Grima, F. (2010). Relationship between perceived body weight and body mass index based on self- reported height and weight among university students: a cross-sectional study in seven European countries. BMC Public Health, 10, 1-11. DOI: 10.1186/1471-2458-10-40. [ Links ]
26. Mussell, M.P., Mitchell, J.E., de Zwaan, M., Crosby, R.D., Seim, H.C., & Crow, S.J. (1996). Clinical characteristics associated with binge eating in obese females: a descriptive study. International Journal of Obesity and Related Metabolic Disorders, 20, 324-331. [ Links ]
27. Pearl, R. & Lebowitz, M. (2014). Beyond personal responsibility: Effects of causal attributions for overweight and obesity on weight-related beliefs, stigma, and policy support. Psychology & Health, 29, 1176-1191. DOI: 10.1080/08870446.2014.916807. [ Links ]
28. Preacher, K.J., Rucker. D.D., MacCallum, R.C., & Nicewander, W.A. (2005). Use of the Extreme Groups Approach: A Critical Reexamination and New Recommendations. Psychological Methods, 10, 178-192. DOI: 10.1037/1082-989X.10.2.178. [ Links ]
29. Ramos-Valverde, P., Rivera de los Santos, F., & Moreno-Rodriguez, C. (2010). Diferencias de sexo en imagen corporal, control de peso e Índice de Masa Corporal de los adolescentes españoles (Sex differences in body image, weight control and Body Mass Index of Spanish adolescents). Psicothema, 22, 77-83. [ Links ]
30. Smink, F.R., Van Hoeken, D., & Hoek, H.W. (2012). Epidemiology of eating disorders: incidence, prevalence and mortality rates. Current Psychiatry Reports, 14, 406-414. DOI: 10.1007/s11920-012-0282-y. [ Links ]
31. Snoek., H., Van Strien, T., Janssens, J., & Engels, R. (2008). Restrained Eating and BMI: A Longitudinal Study among Adolescents. Health Psychology, 27, 753-759. DOI: 10.1037/0278-6133.27.6.753. [ Links ]
32. Stice, E., Cooper, J.A., Schoeller, D.A., Tappe, K., & Lowe, M.R. (2007). Are dietary restraint scales valid measures of moderate to longterm dietary restriction? Objective biological and behavioral data suggest not. Psychological Assessment, 19, 449-458. DOI: 10.1037/1040-3590.19.4.449. [ Links ]
33. Stice, E., Fisher, M., & Lowe, M. R. (2004). Are dietary restraint scales valid measures of acute dietary restriction? Unobtrusive observational data suggest not. Psychological Assessment, 16, 51-59. DOI: 10.1037/1040-3590.16.1.51. [ Links ]
34. Stunkard A. & S. Messick (1985). The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. Journal of Psychosomatic Research, 29, 71-83. DOI: 10.1016/0022-3999(85)90010-8. [ Links ]
35. Stunkard, A. & Stellar, E. (1990). Eating and its disorders. In Cash, T. & Pruzinsky, T. (Eds), Body Images (pp., 3-20). Guilford Press: New York. [ Links ]
36. Teachman, B. A., Gapinski, K. D., Brownell, K. D., Rawlins, M., & Jeyaram, S. (2003). Demonstrations of implicit anti-fat bias: The impact of providing causal information and evoking empathy. Health Psychology, 22, 68-78. DOI: 10.1037/0278-6133.22.1.68. [ Links ]
37. Wilmot, E., Edwardson, C., Achana, F., Davies, M., Gorely, T., ... & Biddle, S. (2012). Sedentary time in adults and the association with diabetes, cardiovascular disease and death: systematic review and metaanalysis. Diabetologia, 55, 2895-2905. DOI: 10.1007/s00125-012-2677-z. [ Links ]
38. Yang, W., Kelly, T. & He, J. (2007). Genetic epidemiology of obesity. Epidemiogical Reviews, 29, 49-61. DOI: 10.1093/epirev/mxm004. [ Links ]
![]() Correspondence:
Correspondence:
Alejandro Magallares,
Departamento de Psicología Social y de las Organizaciones,
Facultad de Psicología UNED,
C/ Juan del Rosal, 10, 28040 Madrid (Spain).
E-mail: amagallares@psi.uned.es
Article received: 18-12-2014;
revised: 18-02-2015;
accepted: 08-03-2015

