










 Custom services
Custom services
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Adherence to healthy behaviours has been one of the most important research topics in recent years (WHO, 2004). The difficulty of adopting and/or maintaining healthy behaviour has led organisations to provide favourable contexts to improve lifestyles by increasing physical activity and consuming less high-fat and high-sugar food, among others (WHO, 2016, 2020). However, early findings indicate that, even when favourable environments exist, they are not sufficient to encourage people to adopt or maintain healthy behaviour, contributing to behavioural abandonment (Giles-Corti & Donovan, 2002; Morgan & Dishman, 2001).
A variety of theoretical models have attempted to understand the dynamics of behavioural change by demonstrating strong associations between psychological variables and health behaviours. Some examples are self-determination theory (Ryan & Deci, 2017), the transtheoretical model of change (Prochaska & DiClemente, 1983), and, recently, the Grit personality (Duckworth et al., 2007).
Globally, in 2016, 39% of adults aged 18 years and older were overweight, and 13% were obese (WHO, 2021). The Region of the Americas has the highest prevalence, and 62.5% of adults are overweight and obese (64.1% of men and 60.9% of women) (PAHO, 2021). In Mexico, in 2019, the prevalence of overweight and obesity was reported to be 76.8% in women and 73% in men, increasing more than 12% between 2000 and 2018 in the entire population (NIPH/SH, 2020). In a situation of overweight and obesity, weight control is clearly a primary health promotion behaviour (PAHO, 2021; WHO, 2021). Weight control refers to controlled dietary intake and physical activity with the primary goal of losing weight, maintaining a healthy weight, or achieving an ideal body shape (Wing & Hill, 2001).
This study has two main objectives: (1) to assess healthy weight control behaviour from a perspective that integrates important theoretical models of healthy behaviour and addresses the need to evaluate models and sets of variables that can explain the behavioural outcome (Palmeira et al., 2007) by developing better explanatory models that lead to more effective interventions (Rothman, 2004); and (2) to provide clinical and social-community nutrition professionals with better knowledge and application tools, enabling them to assess the patient or population group from a more holistic perspective that promotes change.
Some studies have shown that personality traits such as impatience, negative emotionality, impulsivity, responsibility, extraversion, and neuroticism are associated with excessive caloric intake, weight gain, risky behaviours, sedentary behaviour, and healthy and unhealthy eating behaviours (Armon et al., 2013; Caspi et al., 1997; Monds et al., 2015; Räikkönen et al., 2003; Sutin et al., 2011). Thus, interest in understanding the role of personality in healthy behaviours has been growing, arguing that the main effect that personality has on health-related behaviours occurs through the quality of our health practices (Rhodes & Smith, 2006).
The Grit personality has been cited as a predictor of achievement, performance, and success. Grit, or the passion and perseverance to achieve long-term goals (Duckworth et al., 2007, Duckworth & Quinn, 2009), has been defined as the tenacious pursuit of a priority goal over time and despite setbacks (Duckworth & Gross, 2014), and it has been found to be a predictor of performance success in different contexts (educational, military, etc.), beyond domain-specific skills or intelligence (Cormier et al., 2019; Duckworth et al., 2007; Schmidt et al., 2018). Grit has been conceptualised as a trait composed of two factors: 1) consistency of interest or the tendency to maintain commitment and focus on a specific goal over long periods of time; and 2) perseverance of effort, reflected in the pursuit of long-term goals with sustained effort despite setbacks (Duckworth & Gross, 2014). Although Grit has been questioned due to its similarity to the conscientiousness factor and the greater predictive power of perseverance of effort over consistency of interest (Credé et al., 2017; Ponnock et al., 2020; Schmidt et al., 2018), it is still positioned as an important attribute that can explain success (Schimschal et al., 2021). In relation to healthy behaviours, Grit personality has been associated with exercise (Reed, 2014; Reed et al., 2013), better quality of life, better health care skills (physical and mental) (Sharkey et al., 2017; Traino et al., 2019), autonomous motivation towards healthy eating (Marentes-Castillo et al., 2019, 2022), self-control, and use of healthy behaviours and avoidance of unhealthy behaviours for weight control (Marentes-Castillo et al., 2022).
Results supported by self-determination theory (Deci & Ryan, 2008; Ryan & Deci, 2017) have shown that autonomous motivation is one of the best predictors of ideal weight maintenance, physical activity, weight control, eating regulation, and the use of healthy weight control behaviours (Marentes-Castillo et al., 2022; Ntoumanis et al, 2021; Santos et al., 2016; Teixeira et al., 2006, 2015). This theory focuses on the quality of motivation and its different types (i.e., autonomous, controlled, and amotivation), as well as on the autonomy of human behaviour, which impacts overall well-being. According to this theory, autonomous motivation is present when human behaviour is the result of a human being's free will, reflecting his or her values, beliefs, and interests. Controlled motivation reflects behaviour resulting from pressure from various external factors, leading the person to exhibit behaviour that is inconsistent with his or her values, interests, and beliefs. Finally, amotivation refers to a person's passivity and lack of intention to engage in a behaviour (Ryan & Deci, 2017). It has been emphasised that special attention should be paid to motivational dynamics in the initiation and persistence of behaviour (Silva et al., 2010) in order to understand the process of weight management (Teixeira et al., 2012) and discover how to maintain the behaviour in the long term (Teixeira & Mata, 2011), referring to the fact that motivation may be modifiable through intervention (Silva et al., 2010; Teixeira et al., 2012).
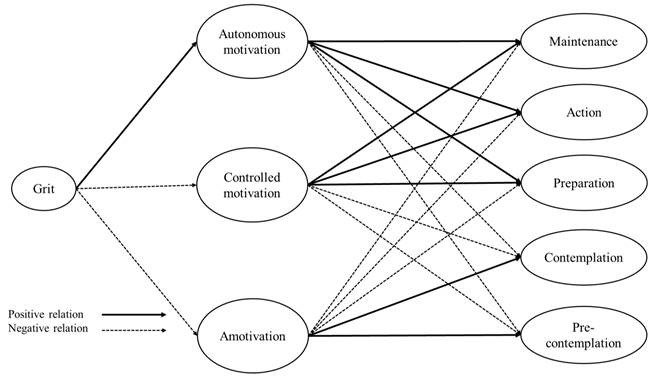
Similarly, the transtheoretical model of change (Krebs et al., 2018; Prochaska & DiClemente, 1983, Prochaska et al., 1992) has described change through five stages (i.e., precontemplation, contemplation, preparation, action, and maintenance, see Figure 1) and emphasised the importance of knowing the period of change the person is in, personalising the intervention strategies implemented to accelerate that change. People in the precontemplation stage have little or no awareness that there is anything to change. In the contemplation stage, they begin to be aware that something can be changed, and they are thinking seriously about it but still not committed to the change. They spend a lot of time evaluating the advantages and disadvantages of changing, as well as the effort that has to be invested in the change. In the preparation stage, the first attempts to change are made, and often small changes are achieved, with small decreases in the behaviour in question. However, people are not yet fully committed to the change and can spend about a month in this stage. Change is complete when they move to the action stage, which requires a considerable investment of time and energy. If individuals manage to continue to change for at least six months, they have moved into the maintenance stage, where significant changes and achievements are made, behaviour is stabilised, and relapse into old patterns of behaviour is prevented. The application of this model to weight control has shown significant changes in weight management, consumption of fruits, vegetables, and products high in fat and sugar, and physical activity (Mastellos et al., 2014). Interventions based on the transtheoretical model of change promote a reduction in the consumption of high-calorie and high-fat foods, with positive effects on weight and body image perception (Carvalho et al., 2015).

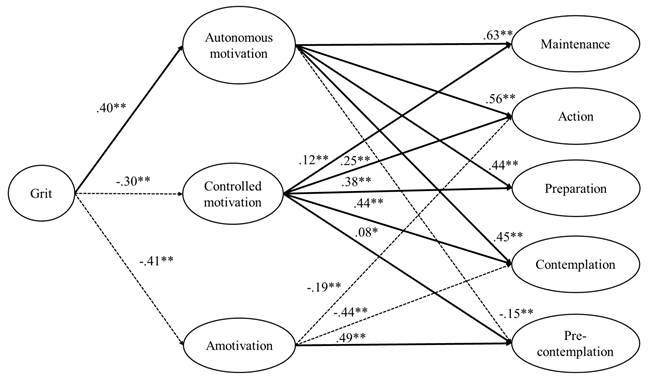
To gain a better understanding of the complexity of weight control behaviour by integrating three theoretical models (i.e., Grit personality, self-determined motivation, and stages of change), the aim of this study was to test a relationship model that hypothesises that Grit personality predicts the stages of change towards weight control through the types of motivation (autonomous, controlled, and amotivation) (see Figure 2).
Method
Participants
The research design is empirical, associative explanatory, and cross-sectional (Ato et al., 2013). Participants were 1,351 adults (688 women, 663 men) who were representative of the municipality of Monterrey, Nuevo León, Mexico and aged between 18 and 65 years old (M = 29.59; SD = 12.01). Multistage sampling with proportional allocation (distribution of the sample size) was used in five phases (choice of Monterrey, random selection of neighbourhoods, gender proportion, age range according to adult population distribution, and minimum number of participants to be able to generalise the results), generating four age groups: 18-29 years (n = 839), 30-44 years (n = 142), 45-55 years (n = 142), and 55-65 years (n = 66) (162 subjects did not answer the question about their age). Regarding their marital status, 58.1% (n = 785) were single, 27.7% (n = 374) were married, and the remaining 14.2% (n = 192) were separated, divorced, etc. In addition, 59.3% (n = 801) were college graduates, 25.5% (n = 344) had completed high school, and 15.2% (n = 206) had a lower academic degree. In terms of body mass index (BMI), 34.9% of the sample were in the normal weight range (18.5-24.9), 22.1% were classified as overweight (25-29.9), 11.7% were obese (>30), and 31.3% chose not to share their weight and height data, and so the BMI variable was not used in the data analysis. Inclusion criteria were age between 18 and 65 years old and being a resident of the municipality of Monterrey.
Instruments
The following instruments were administered:
Grit personality scale (Duckworth et al., 2007, Duckworth & Quinn, 2009) adapted to Spanish spoken in Mexico (Marentes-Castillo et al., 2019). It contains 12 items divided into two six-item subscales: consistency of interest (e.g., “My interests change from year to year") and perseverance of effort (e.g., "I have achieved a goal that took years of work"), which are answered on a Likert-type scale ranging from 1 (Not like me at all) to 5 (Very much like me). Although the original scale was developed to measure the two Grit factors or subscales, some authors consider an aggregated score to represent overall Grit (for a systematic review, see Credé et al., 2017). In this study, we use an aggregated score.
Exercise Regulations Questionnaire (BREQ-3) (Wilson et al., 2006), adapted to weight control and to Spanish spoken in Mexico for this study. The 23-item questionnaire begins with the statement "I control my weight...", and it is divided into six subscales: intrinsic regulation (e.g., "Because I enjoy the moments when I control my weight"), integrated regulation (e.g., "Because it is consistent with my life goals"), identified regulation (e.g., "Because I value the benefits of controlling my weight"), introjected regulation (e.g., "Because I feel guilty when I don't"), external regulation (e.g., "Because other people say I should"), and amotivation (e.g., “But I think controlling my weight is a waste of time"). These regulations are grouped into three types of motivation: autonomous motivation (integrating items from intrinsic, integrated, and identified regulation), controlled motivation (integrating items from introjected and external regulation), and amotivation. Items are responded to on a Likert-type scale ranging from 0 (Definitely not true) to 4 (Definitely true).
Stages of Change Questionnaire (URICA-Continuous Form) (Marcus et al., 1992), adapted to weight control and to Spanish spoken in Mexico for this study. It contains 24 items divided into five subscales corresponding to the five stages of change. The precontemplation stage contains eight items (e.g., "I do not have time or energy to lose/control my weight regularly"), and the other stages contain four items each: contemplation (e.g., "I have been thinking that I might want to start losing/controlling my weight regularly"); preparation (e.g., "I have set a day and a time to start lose/control my weight within the next few weeks; action (e.g., "I am finally losing/controlling my weight regularly"); and maintenance (e.g., "I have managed to lose/control my weight regularly thorough the last 6 months"). Items are responded to on a Likert-type scale ranging from 1 (Strongly disagree) to 5 (Strongly agree).
Following the recommendations of the International Test Commission (ITC, 2018), the English version of the motivation types questionnaire and the stages of change scale, both adapted to weight management, were translated into Spanish spoken in Mexico using the double translation and reconciliation procedure.
Procedure
This study was conducted in accordance with international ethical guidelines consistent with the American Psychological Association and in accordance with the guidelines set forth in the Declaration of Helsinki (WMA, 2013). All procedures involving participants in the research study were approved by the Institutional Review Board of the Autonomous University of Nuevo León, México (REPRIN-FOD-83). After the sample had been selected in the randomly selected neighbourhoods of the city of Monterrey, the project was presented to each research participant. Data collection was carried out by trained enumerators, who resolved any doubts that might arise, in the period between November 2018 and March 2019. The administration of the instruments was carried out in the participants' homes and took between 15 and 20 minutes to complete. It was supervised by the enumerators, who requested honesty in the answers. Prior to the administration of the questionnaires, informed consent was requested in writing from all the sample members to participate freely and anonymously in the study.
Statistical analysis
Multivariate outlier, distribution, and normality analyses were performed. No missing values were detected. Descriptive, normality, and reliability analyses were obtained for all study variables using Cronbach's coefficient and composite reliability. Values considered acceptable for these indicators should be greater than .70 (Cronbach, 1951; Hair et al., 1999). Subsequently, multivariate analysis of variance (MANOVA) was carried out to assess the variability between the groups and the variables studied, and Pearson's correlation analysis was performed to corroborate the relationship between the variables. These analyses were carried out using the SPSS statistical package version 25.
The measurement model was calculated considering Grit personality, the three types of motivation, and the stages of change towards weight control as latent variables and their respective items as indicators. The analysis of the structural equation model allowed us to estimate the effect and the multiple relationships between the variables studied, first testing the measurement model and then the structural model. Due to the ordinal nature of the variables, the maximum likelihood estimation method was used. The χ2, the non-normative fit index (NNFI), the comparative fit index (CFI), and the root mean squared error of approximation (RMSEA) were used to verify the model fit. NNFI and CFI values above .90 indicate an acceptable fit of the data. RMSEA values below .08 are considered satisfactory. These analyses and the confirmatory factor analyses (CFA) of the scales were performed using the LISREL software version 8.80.
Results
The results of the CFAs of the instruments used in the study are presented below. The fit indices of the two-factor model with a second-order single-factor factor of the Grit personality, after removing Item 3 ("I become interested in new pursuits every few months") corresponding to the consistency of interest subscale due to low saturation, were adequate: χ2 = 25949, df = 43, p < .01, NNFI = .96, CFI = .97, and RMSEA = .06. The fit indices of the three-dimensional model of the exercise regulations questionnaire were satisfactory: χ2 = 2733.17, df =227, p < .05, NNFI = .94, CFI = .94, and RMSEA = .09. Finally, the fit indices for the five-factor model of the stages of change questionnaire, after removing Item 1 ("As far as I´m concerned, I don´t need to lose/control my weight") corresponding to the precontemplation stage due to low saturation, were also adequate: χ2 = 1469.54, df = 220, p < .05, NNFI = .94, CFI = .94, and RMSEA = .07.
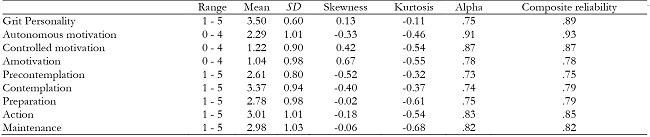
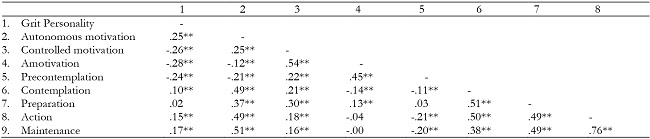
Skewness and kurtosis values were within the appropriate parameters (+1, -1). Participants perceived themselves as having Grit personality characteristics and autonomous motivation above the scalar mean. Controlled motivation and amotivation were below the scalar mean. For the stages of change (continuous form), participants perceived themselves as being above the scalar mean in the contemplation stage and in the action stage and below the scalar mean in the maintenance, preparation, and precontemplation stages. Furthermore, adequate reliability was observed for all the variables (Table 1), and correlation analyses indicated significant associations between all the variables, in line with theoretical expectations, with the exception of the null association between Grit personality and the preparation stage and between amotivation and the action and maintenance stages (Table 2).
MANOVA analyses showed no significant differences according to sex, age, or the interaction between the two (Λ Wilks = .97; F = .97, df = 39, p = .51, Eta = .01), and so the following analyses were performed for the overall sample. The measurement model showed satisfactory fit indices: χ2 = 56,236.80, df = 1493; p < .001; NNFI = .96; CFI = .96; and RMSEA = .05. All the variables were associated with their items. The hypothesised model also showed satisfactory fit indices: χ2 = 7,554.20, df = 1521; p < .001; NNFI = 92; CFI = .94; and RMSEA = .06. Grit personality was positively and significantly related to autonomous motivation, and negatively and significantly related to controlled motivation and amotivation. In turn, autonomous motivation was positively and significantly related to the maintenance, action, preparation, and contemplation stages, and negatively and significantly related to the precontemplation stage. Controlled motivation was positively and significantly related to all the stages of change, but most strongly to the contemplation stage, moving downward to the preparation, action, maintenance, and precontemplation stages. Amotivation was negatively and significantly related to the action and contemplation stages, and positively and significantly related to the precontemplation stage (see Figure 3). Finally, indirect effects showed that the Grit personality was related to all the stages of change across the motivation types. Specifically, Grit personality was positively and significantly related to the maintenance stage (β = .23, p < .01), the action stage (β = .23, p < .01), the preparation stage (β = .07, p < .05), and the contemplation stage (β = .23, p < .01), and it was negatively and significantly related to the precontemplation stage (β =-.28, p < .01). The model explained 40% of the variance in the maintenance stage, 40% of the variance in the action stage, 30% of the variance in the preparation stage, 56% of the variance in the contemplation stage, and 31% of the variance in the precontemplation stage.
Discussion
The present study, as described in the literature review, integrates the Grit personality, the types of motivation, and the stages of change towards weight control into a single theoretical model, in order to achieve a better approach to the phenomenon of adopting and maintaining weight control in a sample of Mexican adults. The resulting model reveals, in general, that individuals with a Grit personality are more likely to engage in weight control change through autonomous motivation, and less likely through controlled motivation and amotivation. If we focus on the types of motivation, autonomous motivation and controlled motivation are associated with the same stages of change, but autonomous motivation is more strongly associated with the most active stages of change (maintenance, action, and preparation), as well as with the contemplation stage, which, although considered a non-active stage, can be considered an activating stage of change (Krebs et al., 2018; Prochaska et al., 1992). In this case, initially, weight control behaviour can be performed in a controlled manner or conditioned by external factors (e.g., I was told to do so by my doctor) (Deci & Ryan, 2012; Deci et al., 1994); however, consistently performing a behaviour in a controlled manner can lead to unhealthy weight control behaviours (e.g., I use laxatives to lose weight) (Deci & Ryan, 2000). Amotivation, however, is strongly associated with the precontemplation stage, which is the least active stage of all, where there is no awareness of the problem to be modified (Deci & Ryan, 2012, Krebs et al., 2018).
In general, it is estimated that when individuals with a Grit personality make the change towards weight control, it is mostly for internal reasons, and to a lesser extent for controlled reasons and amotivation. Teixeira et al. (2012) mentioned that the maintenance of weight control behaviour depends not only on compliance with external demands, but also on the change as something internal to the individual. Furthermore, Duckworth (2016) suggested that goal setting (e.g., weight control) included being motivated, and Williams et al. (1996) emphasised that weight control behaviour could not be successful if the reasons for doing it were controlled, stressing that autonomous motivation is the best predictor of commitment to an activity that requires discipline and effort (Deci & Ryan, 2012). In the present study, autonomous behaviour is the best mediator of the stages of change towards weight control.
These results suggest that Grit personality and autonomous motivation are positively associated with favouring change and promoting greater permanence in the behaviour, similar to previous studies (Reed, 2014; Reed et al., 2013) showing that Grit predicted moderate and intense exercise in the later stages of change (i.e., maintenance and action). In this regard, it has been pointed out (Rothman, 2000) that initially people adopt a behaviour that they want to achieve, and then in the maintenance stage, the goal is to avoid returning to unhealthy behaviours.
The relationships between personality and motivation were emphasised by Von Culin et al. (2014), who mentioned that it was possible for personality to have a differentiating effect on motivation types. This is confirmed in our study, where Grit personality is associated differently with each type of motivation towards weight control. The above results confirm that Grit plays an important role in quality of life, physical and mental health, and healthy eating (Marentes-Castillo et al., 2019, 2022; Sharkey et al., 2017; Traino et al., 2019).
The practical implications of this study are related to its usefulness in providing nutrition professionals with better knowledge and applicability tools. In the therapeutic context, individuals entering a weight control treatment generally expect to be given indications and/or recommendations related to the treatment for their condition, and health professionals very rarely give patients the opportunity to discuss the actions to follow or provide adequate justification for carrying out the action (Teixeira et al., 2012). Therefore, knowing the individual's Grit personality and differentiating his/her type of motivation can provide better insights and adaptations of recommendations and actions that can be taken by the patient who is acquiring the weight control behaviour. Understanding the psychological processes involved in the individual's engagement will be crucial in the quest to maintain weight control (Teixeira et al., 2011).
In addition, we believe that a better understanding of behavioural change towards weight control may also be helpful in understanding why favourable environments for performing the behaviour are not sufficient for healthy change. The relative success of public policies may be influenced by psychological aspects (Robinson et al., 2020).
Conclusions
This study proposes a theoretical model that takes a more comprehensive approach to behavioural change towards weight control, answering questions such as: Why don't people stick to healthy behaviours? The answer is associated with the role of the Grit personality as an important attribute that explains the interest, focus, and perseverance of a behaviour over time and its clear association with autonomous motivation, which acts as a significant mediator of change and maintenance of weight control.
Limitations of the study include its cross-sectional and non-experimental nature, as well as the information collected in the form of self-reports. However, because the study was conducted with a large sample with characteristics of the normal population, we believe that this study has significant potential for cross-sectional research on weight control in contributing to understanding the mechanisms and causal factors of this healthy behaviour (William et al., 2017). Moreover, it can foster longitudinal study designs, in order to continue to examine the dynamics of these variables in weight control using objective measures of weight gain and/or loss.
It is important to continue to explore and delve into the various associations between personality, motivation, and stages of change by including other variables that may also play an important role in change, such as self-efficacy and social support, among others. In addition, it is important to explore the role of controlled motivation. Although it plays a role in change, it could lead to unhealthy behaviours in the long term, and so studies should try to determine not only whether weight is controlled or not, but also how it is controlled. This study leaves some questions unexplored: How can we strengthen the Grit personality? How can we formulate interventions that integrate all the elements studied in this research and produce an improvement in the practice of the nutritional health professional and in public health policies?

