










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Anxiety and mood disorders are among the most prevalent issues in mental health, and they have become more frequent over the past few decades (Remes et al., 2016). Specifically, anxiety disorders affect 6.7% of the users of the Spanish health care system (8.8% of women and 4.5% of men), making them the most frequently appearing mental health problem in primary care centers (Subdirección General de Información Sanitaria, 2020). Despite the frequency with which people seek care for their anxiety symptoms at primary care centers, and despite the fact that people with anxiety disorders often prefer to be treated in this setting (Shepardson & Funderburk, 2016), these facilities themselves do not often offer treatment to these patients (Alonso et al., 2018; Shepardson et al., 2018). In other words, primary care services to treat anxiety disorders remain scarce, even though it is clear that these disorders have a negative effect on people's quality of life and involve high costs in terms of health and productivity (Bandelow & Michaelis, 2015).
It is clear, then, that anxiety disorders have serious consequences for both patients and for the public health care system as a whole. There is also broad consensus among professionals that these disorders can be effectively treated in the primary care context (Cano-Vindel et al., 2016, 2021; Shepardson et al., 2018; Twomey et al., 2015). In light of all this, it is necessary to develop quality intervention programs that make it possible to meet the needs of these patients in this setting. Among the treatments for anxiety disorders, there is a great deal of evidence for the effectiveness of Cognitive-Behavioral Therapy (CBT), the approach that is recommended in the most prominent guides to good practices (Carpenter et al., 2018; Kaczkurkin & Foa, 2015; Twomey et al., 2015; Zhang et al., 2019). This type of therapy has proven to be an efficient and effective way to reduce anxiety symptoms in a range of different presentations of anxiety disorders (Kaczkurkin & Foa, 2015), whether via exposure techniques or cognitive therapy.
Although in many cases professionals choose to treat these patients via individual interventions, especially when mood disorders are also involved, group therapy offers a number of potential benefits, especially in the context of primary care. A number of studies have found that group interventions can be just as effective as individual treatment (i.e. Fanous & Daniels, 2020) and that both approaches can be valid ways to treat anxiety disorders (Fawcett et al., 2020). Additionally, group CBT offers some advantages in terms of treatment efficiency which is always an important concern for public health services. Group therapy can also provide benefits in terms of group cohesiveness, improved interpersonal skills, greater feelings of hope and an enhanced sense of universality (Cordero-Andrés et al., 2017). Therefore, group therapy has a good deal of potential in the context of primary care, as it can help reduce the costs associated with care and decrease the number of doctor visits in public health jurisdictions. Nonetheless, there have been few clinical trials aimed at assessing the results of group interventions (Zhang et al., 2019).
People with anxiety disorders, and specifically those diagnosed with Generalized Anxiety Disorder (GAD), often have trouble identifying and regulating their emotions, especially when it comes to negative emotions ( i.e. Lizeretti & Extremera, 2011; Kerns et al., 2014). These difficulties in managing, differentiating and regulating emotions might pose an additional risk factor in the development of these disorders (Lizeretti, 2009, 2012; Lizeretti & Extremera, 2011). Thus, it is important for interventions aimed at people with anxiety disorders to provide support in the understanding and management of emotions and to offer strategies that can serve as protective factors (Calzada, 2020).
While it is true that cognitive-behavioral therapy has proven effective at reducing the symptomology associated with a range of mental health disorders, there is less evidence for the effects of this approach when it comes to promoting overall mental health and wellbeing (Gallagher et al., 2020). Beyond the symptoms themselves, people who suffer from anxiety disorders also experience negative effects on their overall quality of life, family functioning and perception of social support (Wang et al., 2016). Recent research has indicated that, for people with these disorders, improvements in emotional regulation are associated with an enhanced quality of life (Conroy et al., 2020). Another important aspect, and one that has not received sufficient attention from researchers, is the relationship between this improved emotional management and subjective wellbeing, especially with one of the components of this concept, life satisfaction. There is evidence that interventions featuring emotional regulation strategies tend to be more effective at improving the life satisfaction of people with anxiety disorders (Jazaieri et al., 2017), and such strategies have also produced promising results in terms of contributing to CBT's potential to produce lasting changes in the wellbeing of people with anxiety, displaying a relationship with changes in anxiety disorder symptoms (Gallagher et al., 2020).
Meanwhile, it is important to highlight the important role that self-esteem can play within disorders of this type. Low self-esteem means a greater risk of anxiety and thus a greater predisposition toward anxiety disorders and it also can be a protective factor against anxiety (Bajaj, Robins & Pande, 2016; Iancu et al., 2015; Rossi et al., 2020). The inverse is true as well, in that those who suffer from anxiety disorders often experience decreases in self-esteem (Manna et al., 2016). Some CBT approaches have attempted to address issues such as self-esteem, self-criticism, dependency and self-efficacy, all with an eye toward improving anxiety disorder symptoms (Iancu et al., 2015). Related approaches are found in the form of transdiagnostic treatments such as the United Protocol for Transdiagnostic Treatment of Emotional Disorders (UP) (Barlow et al., 2017; Eustis et al., 2020), an intervention that has achieved results that are equally as promising as those aimed only at a single diagnosis. This opens up a range of possibilities in the field of primary care, allowing professionals to treat the most common emotional disorders together and, consequently, more efficiently.
The objective of this study is to assess the effectiveness of a program of CBT with an eclectic approach featuring emotional techniques (CEBT), as compared with the results of a control group using traditional CBT, both in the context of the public health system.
Methods
Participants
Two hundred and thirty-seven patients were recruited from the Adult Outpatient Mental Health Center of Mataró (Barcelona), Consorci Sanitari del Maresme. They were referred by general practitioners from nine different public health jurisdictions. They had all received a main diagnosis (according to the DSM 5) (American Psychiatric Association, 2013) of an anxiety disorder (by their family doctors, then by experienced professionals at the Mental Health Center), and they all signed the informed consent document. Exclusion criteria were: prior diagnosis of intellectual disability, borderline personality disorder, major depressive disorder, bipolar disorder, obsessive-compulsive disorder, suicide risk or psychotic disorders.
Design
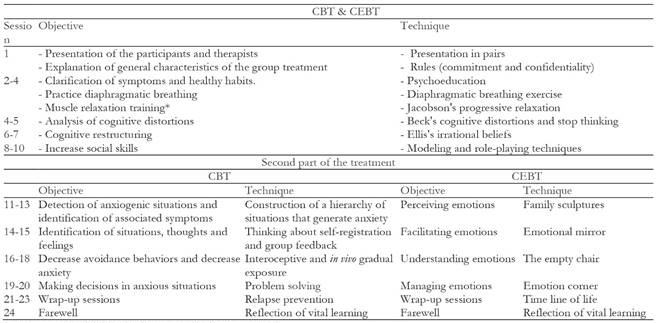
The study design was a randomized clinical trial with an experimental group and a control group. The experimental group received a program of cognitive behavior therapy with elective techniques (CEBT), and the control group was treated with traditional cognitive-behavior therapy (CBT) for anxiety. The first half of the intervention program was the same for both groups, meaning that they were distinct only in the second part of the intervention, beginning with the 11th session.
For both the experimental and control group, the first part of the intervention consisted of cognitive-behavioral techniques with the aim of clarifying the symptoms and healthy habits. In addition to these psychoeducational activities, these first sessions also included breathing exercises, muscle relaxation training through Jacobson's progressive relaxation technique (four sessions), free relaxation (from the sixth session on), anxiety management techniques, thought stopping and cognitive restructuring. There were also three sessions featuring modeling techniques and role-playing activities aimed at increasing assertiveness.
The techniques used in the second part of the intervention were completely different in the CEBT and CBT groups. The control group (CBT) received treatment including detection of anxiety-producing situations and identification of associated symptoms, construction of a hierarchy of anxiety-provoking situations, analysis through self-recording mechanisms, gradual interoceptive and life exposure, and work on problem-solving techniques aimed at enhancing decision making.
The experimental group intervention incorporated techniques based on other theoretical orientations (technical eclecticism) with the goal of addressing emotions. The techniques included family sculptures (Onnis, 2007), the empty chair (Greenberg et al., 1996; Greenberg & Paivio, 2000), emotion corners (Lizeretti, 2012) and the timeline (James & Woodsmall, 1988).
The final session for both groups consisted of a review, designed to help prevent relapses and to give participants an opportunity to reflect on the life lessons they had learned.
Both the experimental and control interventions were carried out in the form of group therapy. Each group completed a total of 20 sessions of 90 minutes in length over a period of five months, meeting once a week. The sessions were led by an experienced therapist and a co-therapist (both with university degrees in Psychology). The same therapists led both the CEBT and the CBT group (in the same way as other studies, for example Barlow et al., 2017). In order to ensure that the therapists faithfully carried out the different kinds of intervention protocol, standardized manuals were created for the treatment process (see table 1).
The interventions began in September 2007 and concluded in June 2012.
Instruments
In order to monitor the therapeutic process, the following tests were administered at the start of the intervention (baseline assessment) and at the end (post-treatment assessment): Rosenberg Self Esteem Scale (1965; Spanish translation in Rosenberg, 1973), with an internal consistency of the scales of between α = .76 and α = .87; the State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch & Lushene, 1970; Spanish adaptation by the R&D department TEA Ediciones, 2002), with a reliability for patients with anxiety disorders of between α = .87 and α = .93; the Symptom Checklist-Revised (SCL-90-R; Derogatis, 1977; Spanish version by González de Rivera et al., 1989), with a satisfactory degree of internal consistency of scales, from α = .69 (phobic anxiety) to α = .85 (somatization); and the Trait Meta-Mood Scale (TMMS-24; Salovey, Mayer, Goldman, Turvey & Palfai, 1995; Spanish adaptation by Fernández-Berrocal, Extremera & Ramos, 2004), which displays an internal consistency of de α = .90 for attention, α = .90 for clarity and α = .86 for emotional repair. Participants were also asked about their overall degree of satisfaction with their lives via the Quality of Life Interview-Short Version (QOLI; Lehman, 1988; Spanish translation by Bobes, González & Wallace, 1993), a self-reported scale with a good degree of test-retest reliability (α = .71).
Procedure
Assessment interviews with the participants were carried out at the start of the intervention, once during the process (after 10 sessions had been completed) and at the end of the five-month treatment. After data had been gathered, the data analysis was conducted using the IBM SPSS (v.25) statistical software package.
The present research obtained the authorization and a positive report from the Commission of Ethics and Investigation of the FPCEE Blanquerna and of the Ethical Committee of Clinical Investigation (CEIC 02/09) of Mataró Hospital, part of the Health Consortium of the Maresme.
Results
The final sample consisted of a total of 237 patients who participated in the group psychotherapy process (CEBT n = 139; CBT n = 98). Participants were randomly assigned to either the intervention group (CEBT) or the control group (CBT). Thus, the design of this study is a randomized, controlled, single-blind clinical trial, with two treatment groups.
Group comparison in terms of baseline socio demo graphic variables
The groups were homogenous in terms of the baseline measurements of socio-demographic and clinical variables (see Tables 2 and 3). Of the total number of participants, 25.3% were men and 74.3% were women. They ranged in age from 18 to 79 years old (M = 42.55; SD = 13.169).

Table 3. Group comparison in terms of baseline clinical symptomatology.
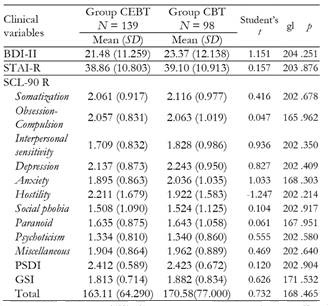
Note.BDI-II: Beck Depression Inventory-II; STAI: State Trait Anxiety Inventory; SCL-90-R: Symptom Checklist-90-R; PSDI: Positive Symptom Distress Index; GSI: Global Severity Index.
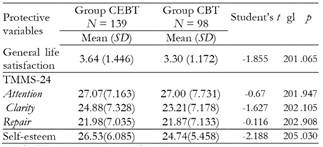
With regard to variables that protect against anxiety, such as emotional intelligence and overall life satisfaction, the groups were also homogeneous upon the baseline assessment, with the exception of the measurement of self-esteem, which was higher in the initial assessment of the CEBT group, according to the analysis of variance of this variable (p = .03) (see Table 4).
Pre and post results in the total sample
At the end of the treatment, the results showed that both groups, analyzed together, showed significant improvements in their levels of depression (Student's t = 3.496; p = .001), overall life satisfaction (Student's t = -4.698; p < .001) and anxiety trait (Student's t = 5.269; p < .001). In fact, these improvements were already appreciable in both groups at the halfway point of the process (after 10 sessions). At that point, there was no difference between the groups, as up to then they had both received the same type of CBT treatment.
Meanwhile, the participants overall recorded significant improvements for all the variables measured by the SCL-90-R, with the exception of hostility (Student's t = 1.45; p = .15), for which the scores worsened slightly but remained in the intermediate range at the end of the intervention.
In terms of the protective variables, both groups displayed improvements at the end of the group therapy process, but the only statistically significant change was in overall life satisfaction (Student's t = -6,887; p < .001). No statistically significant differences were found for attention (p = .066), clarity (p = .636) or emotional repair (p = .368).
Group differences
There was a significantly smaller rate of adherence over the course of the treatment in the CBT group (64.3%, 35 patients) than in the CEBT group (51.07%, 68 patients) (Chi = 5.489; p = .019), but the number of participants who failed to complete the treatment was high in both groups.
The analysis of covariance was done via a multivariate analysis (MANCOVA), with self-esteem included as a co-variable in the measurement of the main results. No differences were found between the groups with regard to the baseline levels of depression (p = .957), anxiety (p = .585) or overall life satisfaction (p = .905). The overall score on the STAI-R scale for the two groups taken together fell by about six points, but this decrease was not significant. This change was mediated by the scores for self-esteem (p=.049). However, this mediating role for self-esteem was not found in the comparison between the two groups in the cases of depression or overall life satisfaction.
Among the protective variables, only overall life satisfaction saw a significantly greater change in the CEBT group, but even for this variable the effect size was small and the power was moderate (see Table 5). It is worth noting that the difference detected between the groups, with a greater improvement for the CEBT group (p = .017), had not been significant when data were collected halfway through the intervention (during the tenth session) (p = .905).
Table 5. Clinical results and protective variables for patients in experimental and control groups, before and after treatment.
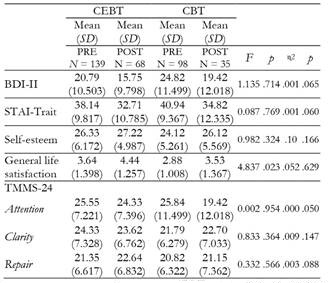
Note.TMMS-24: Trait Meta-Mood Scale; BDI-II: Beck Depression Inventory-II; STAI: State Trait Anxiety Inventory
Self-esteem had a mediating effect associated with greater emotional repair in both groups (p < .001), with a small effect size (η2 = .169) but a high statistical power (P = .992). The same was the case of the scores for depression, as no differences were found between the groups but, once again, self-esteem positively mediates the effect of treatment (p < .001), with a small effect size (η2 = .229) and a high degree of power (P = 1).
Self-esteem also played an important role with regard to changes in anxiety levels. This mediating effect on the patients' evolution over the course of the treatment was visible in both the experimental group and the control group (p < .001). Here, too, there was a small effect size (η2 = .322) and a high degree of power (P = 1).
When it comes to overall symptomatology as measured by the SCL-90 R, no differences were found between the groups for any of the subscales (p <. 05).
In light of the mediating role played by self-esteem found in the results of both groups, a study of the correlations between this variable and the patients' main symptoms was carried out. This analysis showed a significant inverse correlation with levels of depression (r = -.640; p<.001) and anxiety trait (r = -0669; p < .001).
Discussion
This study compares the effectiveness of cognitive-behavioral group therapy treatment with eclectic techniques (including emotional techniques) (CEBT) with more traditional cognitive-behavior group therapy (CBT) for people with anxiety disorders. As was expected, the participants in both groups achieved significant improvements in anxiety and depression after the interventions, a result that confirms the findings in the literature (Barlow et al., 2017; Carpenter et al., 2018; Kaczkurkin & Foa, 2015; Twomey et al., 2015; Zhang et al., 2019). There were also improvements in the rest of the general clinical symptoms assessed in the study (with the sole exception of hostility, which remained at moderate levels).
The participants also attained significant improvements in their overall degree of satisfaction with their lives, with the greater improvement occurring in the CEBT group at the end of the intervention, after 20 sessions. This greater improvement in the group treated with emotional techniques was not apparent after the tenth session. This result is coherent with the design of this study, as up until the tenth session the two groups received the same treatment. It was only starting in the 11th session that the therapists began to implement the emotional techniques in the CEBT group. Thus, the greater increase in life satisfaction could be attributable to the use of these techniques. This difference was mediated by the protective variable of self-esteem, a finding that also echoes prior research that has pointed to the modulating role that this variable can play in anxiety disorders (Bajaj et al., 2016; Iancu et al., 2015; Rossi et al., 2020 ). Kaczkurkin and Foa (2015) have argued in favor of taking a deeper look at the kinds of patients who might be most likely to benefit from these treatments, and they stressed the need to identify the most important factors that influence the results of CBT and other kinds of treatment. One potential answer to the issues they raise could be connected to the role of self-esteem, as it might be one of the most important assets to consider in psychological intervention because of its moderating role in anxiety disorders (Iancu et al., 2015; Manna et al., 2016). This variable played an especially central role in our study, as it served as a protective factor against both anxiety and depression. These findings suggest that more explicit attempts to address this variable could make a vital contribution to therapy programs.
Meanwhile, the use of emotional regulation strategies by people with anxiety disorders has been shown to be associated with greater life satisfaction, and studies have recommended the inclusion of these strategies in treatment programs for these disorders (Jazaieri et al., 2017). Following this suggestion, this study implemented emotional regulation techniques, but the participants did not display any significant improvements in emotional intelligence. One possible explanation for the lack of differences between the groups in this regard might be that more sessions are needed to fully develop these strategies. Here, they were used only in the second half of the treatment for the CEBT group. It seems, then, that it might take more than the 10 sessions completed here to achieve significant changes in emotional intelligence, as our participants did not record significant results with this amount of treatment. Indeed, another study of participants with anxiety disorders (Lizeretti, 2009) or depression (Calzada, 2020) did find significant changes in emotional intelligence after a larger number of sessions devoted to emotional regulation strategies. It would be of interest to examine the number of therapeutic sessions that are needed to produce appreciable changes in this regard.
The promising results of this study add to the evidence in favor of the presence of psychologists in the primary care setting. It is worth underlining that the treatment rates for people with AP in this context remain low, especially given that people with anxiety often prefer to be treated in primary care centers (Shepardson & Funderburk, 2016). It would be desirable, then, to continue to expand the presence of psychologists at primary care facilities. This would not only help to meet growing demand for psychological treatment, but would also restore some necessary balance to the National Health System, as primary care doctors currently bear an outsized burden, and as many as 25 - 50% of patients who visit primary care services might do so for reasons related to mental health (Remes et al., 2016). One efficient model that could be adjusted to meet the needs of patients with anxiety disorder can be found in the transdiagnostic treatment protocols (Barlow et al., 2017; Cano-Vindel et al., 2016, 2021) currently used for emotional disorders. This approach would make it possible to treat more people in the primary care setting and to meet the growing demand for care.
It is inevitable that in this context some care will be offered in the form of group therapy. As shown in this study, this approach to therapy can contribute to significant improvements in anxiety disorders, and it is a more efficient way to achieve these results. This is an important concern for public health services. At the same time, group therapy fosters interpersonal learning and mutual recognition of shared experiences among participants (Cordero-Andrés et al., 2017). This can engender greater feelings of universality and compassion among the members of a group, and it can help inspire a more positive attitude.
Nonetheless, it is important to mention some of the methodological and psychological limitations of this study. Firstly, a large proportion of the sample was lost over the course of the study. This loss was mainly due to the difficulties involved in gathering the patients' responses to all the instruments. This issue affected both groups, but it was more pronounced in the control group. The patients' motivation and adherence to the treatment was greater in the group using emotional techniques, as this approach addresses an issue at the heart of anxiety disorders. Another significant limitation is the lack of long-term follow-up assessments, which have been carried out in other studies (Cano-Vindel et al., 2021; Eustis, 2020), illustrating the extent to which clinical improvements are maintained over time.
Group psychotherapy interventions for people with anxiety disorders have continued to prove effective at reducing clinical symptomatology and at fostering an active attitude and a climate of mutual support in public health. This study obtained positive results in terms of a reduction in the symptoms of anxiety and depression and overall clinical symptoms, and the participants achieved a significant improvement in their overall satisfaction with their lives (with a greater difference in the experimental group). In light of all of this, we can conclude, in accordance with prior studies (Gallagher et al., 2020), that group cognitive-behavioral therapy with eclectic techniques, including emotional techniques, is an effective way for primary care centers to meet the demands of people suffering from anxiety disorders. Meanwhile, the study also shed light on the relationship between self-esteem and the intensity of anxiety and depression symptomatology, showing a negative correlation between self-esteem and symptoms. This finding underlines the importance of working specifically on self-esteem as a protective factor.
The fact that no significant improvements were recorded in emotional intelligence suggests that more than 10 sessions devoted to emotional techniques should be conducted, as has been the case in previous studies (Calzada, 2020; Lizeretti, 2009).
One limitation of the study is that the age range is very wide, so no general conclusions about a specific age group can be asserted. It would be beneficial for future research to use instruments capable of measuring other variables such as resilience. It would also be of interest to continue to compare different kinds of psychological interventions with one another, not only with TAU as this study and others have done (Barlow et al., 2017). This would make it possible to continue to offer more efficient group therapy programs.

