










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.96 n.3 Madrid Mar. 2004
| PICTURES IN DIGESTIVE PATHOLOGY |
Primary biliary cirrhosis and CREST syndrome
J. C. Marín Gabriel and J. A. Solís Herruzo
Department of Digestive Diseases. Hospital Universitario 12 de Octubre. Madrid, Spain
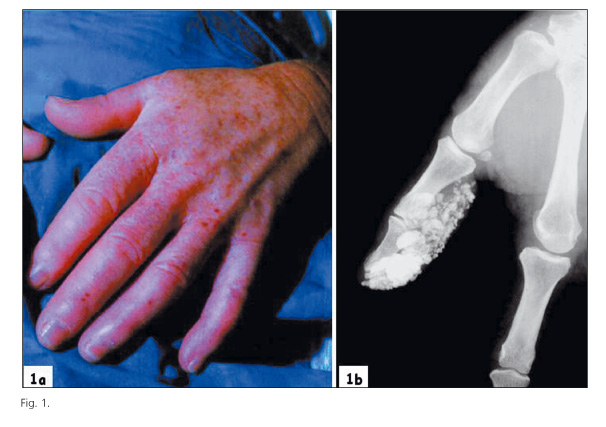
A 54-year-old woman suffering from Raynaud's phenomenon for many years. She had noticed a gradual disappearance of the skin folds of her face and a lack of ability to open her mouth. Her limbs showed sclerodactyly and isolated telangiectases (Fig. 1a). She had positive anticentromere antibody.
She was evaluated because of dysphagia with solids, pyrosis and regurgitation. The esophageal manometry showed a hypotensive lower esophageal sphincter and peristaltic waves of low amplitude in the body of the esophagus. The upper gastrointestinal endoscopy was normal.
She referred fatigue and liver tests showed a cholestatic pattern with high serum levels of alkaline phosphatase and gamma glutamyl transpeptidasa. She had high titers (1:320) of antimitochondrial antibody (AMA) and the serum levels of IgM were also elevated (512 mg/dL). Liver biopsy revealed a moderate periportal inflammatory infiltration and bile duct proliferation consistent with the stage II of the Scheuer's classification of primary biliary cirrhosis (PBC).
The hands X-ray showed massive deposits of material of calcium density inside the thumb (Fig. 1b).
In the limited cutaneous systemic sclerosis (CREST syndrome -calcinosis, Raynaud's phenomenon, esophageal dysfunction, sclerodactyly and telangiectasia), there is an excessive amount of collagen deposited mainly in the skin. In advanced stages of the disease, the synovial membrane of the joints, the tendon sheaths and the fascias, develop fibrin deposits that trend to evolve to fibrosis and finally to produce dystrophic calcifications (calcinosis). The occurrence of calcinosis and telangiectasia have been more frequently described in patients with CREST syndrome when it was associated with PBC in comparison with those who did not show this syndrome.
The sclerodermic patients who develop PBC usually present the limited cutaneous form. In the other hand, the association of PBC with other autoimmune diseases has been reported in up to 60% of the cases, being the CREST syndrome nearly 15% of the total amount.
The association of CREST syndrome and PBC has been called Reynolds' syndrome and some authors suggest that it could represent a subgroup of patients with well-distinguished clinical features and a better prognosis.REFERENCES
1. Tojo J, Ohira H, Suzuki T, Takeda I, Shoji I, Kojima T, et al. Clinicolaboratory characteristics of patients with primary biliary cirrhosis associated with CREST symptoms. Hepatol Res 2002; 22: 187-95.
2. Akiyama Y, Tanaka M, Takeishi M, Adachi D, Mimori A, Suzuki T. Clinical, serological and genetic study in patients with CREST syndrome. Intern Med 2000; 39: 451-6.
3. Akimoto S, Ishikawa O, Muro Y, Takagi H, Tamura T, Miyachi Y. Clinical and immunological characterization of patients with systemic sclerosis overlapping primary biliary cirrhosis: a comparison with patients with systemic sclerosis alone. J Dermatol 1999; 26: 18-22.
4. Márquez F, López L, Alfonso MJ, González-Gay MA, Pérez A. Reynolds syndrome: primary biliary cirrhosis associated with CREST syndrome. Rev Esp Enferm Dig 1990; 78: 311-3.

