










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.102 n.10 Madrid Oct. 2010
LETTERS TO THE EDITOR
Incidental finding of cystadenocarcinoma of the appendix
Hallazgo incidental de cistoadenocarcinoma apendicular
Key words: Incidental cystadenocarcinoma. Carcinoma of the appendix. Cystadenocarcinoma of the appendix.
Palabras clave: Cistoadenocarcinoma incidental. Tumores apendiculares. Ciastoadenocarcinoma apendicular.
Dear Editor,
The incidence of appendicular tumours is relatively low (0.5%). Preoperative diagnosis is difficult and in as many as one-half of cases, the macroscopic appearance of the appendix during surgery suggests a diagnosis of appendicular neoplasia. Below, we describe the case of a patient who underwent surgery for infiltrating neoplasia of the bladder with an incidental finding of mucinous adenocarcinoma of the appendix.
Case report
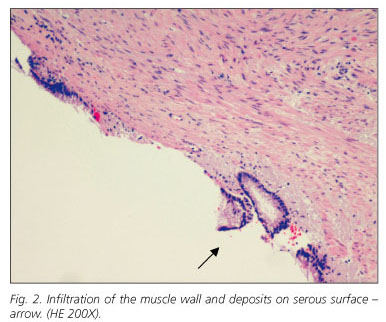
A 73 year-old hypertensive male being followed by urology for hematuria and vesicular neoformation. The findings on abdominal CT with intravenous contrast identify a diffuse parietal enlargement of the bladder wall that extends to the trigone consistent with bladder neoplasia infiltrating the left meatus and secondary obstructive uropathy of the left kidney with no related adenopathies or other tumoral dissemination. With a diagnosis of infiltrating bladder neoplasia, surgery is scheduled. During the surgery, prostatectomy and radical cystectomy with Bricker shunt are performed. The macroscopic appearance of the appendix is normal, performed as part of the appendicectomy. The pathological anatomy of the lesion confirms the diagnosis of transitional cell carcinoma of the bladder and the incidental finding in the appendicular vertex of a cystadenocarinoma of the appendix that infiltrates the serosal membranes with free resection margins and without related adenopathies (Figs. 1 and 2).

Post-operatory recovery without complications and the patient is released eight days after the surgery. After consulting with the hospital's General Surgery Service for histological finding on the appendix, it is decided to perform a colonoscopy and monitor the patient clinically.
Appendicular tumours represent 0.5% of all intestinal tumours. Fifteen to twenty per cent of these tumours are associated with other malignant tumours of the gastrointestinal tract. The most frequent of these are carcinoid tumours (80-90% of appendicular tumours) followed by mucinous cystoadenocarcinoma and adenocarcinoma of the colon.
Preoperative diagnosis is difficult and its clinical presentation mimics acute appendicitis in most patients. Other symptoms are abdominal pain, palpable mass on the lower abdominal quadrant or rectorrhagia. The tomographic finding of a solid-cystic mass dependent upon the appendix with peripheral enhancement or irregularities on the wall and locoregional adenopathies can support the preoperative diagnosis of appendicular tumours (1,2).
Carcinoid tumours less than 1 cm rarely metastasize and simple appendectomy is sufficient. In tumours larger than 2 cm found macroscopically during appendectomy, it is necessary to look for adenopathies and remove them. If metastasis is histologically confirmed, hemicolectomy is recommended (3). In adenocarcinomas of a colonic origin, right hemicolectomy should be performed systematically.
Mucinous cystoadenocarcinoma rarely disseminates lymphatically and grows slower than adenocarcinomas of a colonic origin. However, up to 50% of patients present intraabdominal dissemination, metastasis or pseudomyxoma peritonei. Incidental diagnosis, as occurred in this case, is an infrequent finding and unlike carcinoid tumours, there is no consensus regarding treatment (4,5).
González-Moreno and Sugarbaker (5) retrospectively analysed the long-term survival of 501 patients with epithelial tumours of the appendix. In 198 patients, the surgical technique used was appendicectomy while in 280 patients (55.9%) the technique was right hemicolectomy. According to this study, there were no significant differences between survival and the surgical technique (appendicectomy vs. hemicolectomy) and survival was higher in those cases where intraoperative chemotherapy was applied following the appendicectomy or right hemicolectomy. The authors concluded that right hemicolectomy should be reserved for cases where the mesoappendix or ileocolic ganglia are affected or cases of affected resection margins.
In the case described, the tumour was localised in the appendix; no related adenopathies were identified and the resection margin was free. We consider that oncological surgery is ideal and should be used to rule out other synchronous gastrointestinal tumours.
M. J. Cases-Baldó, D. de Alcalá Martínez-Gómez, M. L. García-García, M. Pérez Ramos1 and J. L. Aguayo-Albasini2
Services of 1Pathological Anatomy and 2General Surgery y Digestive System. Hospital General Universitario Morales Meseguer. Murcia, Spain
References
1. Pickhardt PJ, Levy AP, Rohrmann CA Jr, Dende AI. Primary neoplasm of the appendix: radiologic spectrum of disease with pathologic correlation. Radiographics 2003; 23: 645-62. [ Links ]
2. Pitiakoudis M, Argyropoulou PI, Tsaroucha AK, Prassopoulos P, Simopoulos C. Cystadenocarcinoma of the appendix: an incidental imaging finding in a patient with adenocarcinomas of the ascending and the sigmoid colon. BMC Gastroenterology 2003; 3: 30. [ Links ]
3. Marrie A. Chirurgie de láppendice iléo-caecal. France: Encycl. Méd. Chir. Elsevier ; 1991. [ Links ]
4. Lee J, Gardiner KR, Wilson BG. Incidental mucinous cystadenocarcinoma of the appendix. Postgrad Med J 1996; 72: 55-6. [ Links ]
5. González-Moreno S, Sugarbaker PH. Right hemicolectomy does not confer a survival advantage in patients with mucinous carcinoma of the appendix and peritoneal seeding. BJ Surg 2004; 91: 304-11. [ Links ]

