










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 n.1 Madrid Jan. 2011
LETTERS TO THE EDITOR
Obturator hernia, an uncommon cause of intestinal obstruction
Hernia obturatriz, una causa poco común de obstrucción intestinal
Palabras clave: Hernia, obturatriz. Obstrucción intestinal. Hernia.
Key words: Hernia, obturator. Intestinal obstruction. Hernia.
Dear Director:
Intestinal obstruction is one of the most common diseases worldwide. In the elderly, intestinal obstruction carries a high mortality and its causes are different from those found in younger individuals. One of such causes is obturator hernia, which usually occurs in elderly women and is very easily to detect without imaging studies. Due to its rarity and high mortality, every clinician facing patients with intestinal obstruction should consider it as a differential diagnosis.
Case presentation
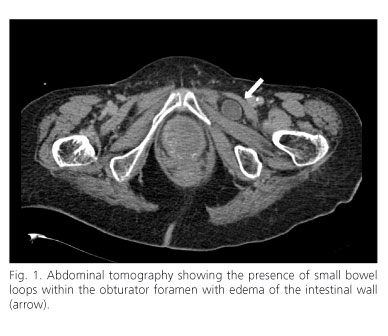
We present the case of an 87 year old woman with a history of ischemic heart disease, hypothyrodism and chronic obstructive pulmonary disease. She presented to our emergency department with abdominal pain located in the left iliac fossa, radiating to the thigh and accompanied by nausea and constipation. Physical examination revealed abdominal distension, tympanism and absence of peristaltic movements. Plain abdominal films showed dilated loops of small bowel with air fluid levels and absence of distal air. A nasogastric tube was inserted and intravenous fluids were administered without clinical improvement. Due to the lack of improvement, an abdominal tomography was performed, showing a hernia of the obturator canal filled with intestinal loops (Figure 1). The patient was operated by means of a medial incision with liberation of the ileum, sac dissection and placement of a mesh in the defect. No complications were reported and there was no evidence of intestinal ischemia. The patient was moved to a hospital ward, where she had an uneventful recovery, and she was discharged home.
Discussion
Obturator hernia, also known as the "skinny old lady hernia" is usually found among septuagenarian women1. This hernia consists of a protrusion of the intestine through the obturator foramen in the pelvic floor. The obturator foramen is located between the two ramus of the ischium and the pubis, and represents a 0.5 centimeter wide and 3 centimeter long tunnel that contains the obturator artery, vein and nerve. In women this foramen is wider, and because of that this hernia is more frequent in female patients. A body mass index below 18.5 and multiparity, which increases the diameter of the obturator foramen, are among the most important risk factors for this hernia2.
The most common clinical presentation of obturator hernia is intestinal obstruction. The pain experienced by our patient, originating from the lower abdomen and radiating to the anterior thigh, is usual in this entity. The most characteristic sign is the Howship-Romberg sign, which consists in a worsening of the pain with the extension, adduction and internal rotation of the extremity due to the compression of the obturator nerve1. Another classic sign is the Hannington-Kiff sign, characterized by the absence of the adductor reflex (which is elicited by tapping on the adductor muscle 5 centimeters above the knee) (3). Abdominal computed tomography is the imaging study of choice for the diagnosis of obturator hernia4. Due to the lack of specific clinical data, only 10-30% of these hernias are diagnosed before a surgical intervention is performed for the treatment of intestinal obstruction lacking response to conservative management (2,5). Once the defect is identified, it should be repaired urgently via an open or laparoscopic approach2.
The mortality of obturator hernia approaches 70% (1, 2, 3). This is due to the delay in diagnosis, the high incidence of intestinal ischemia and perforation, and the affected demographics. Obturator hernia should always be considered as a differential diagnosis in elderly women with intestinal obstruction, and a thorough physical examination directed towards this entity should be performed. At the same time, this case illustrates the importance of abdominal tomography in select patients presenting to the emergency room with the acute abdomen or intestinal obstruction.
E. Soto-Pérez-de-Celis1 y I. González-Pezzat2
1Departamento de Medicina Interna. Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. Ciudad de México. México.
2División de Cirugía. Hospital Ángeles Pedregal. Ciudad de México. México
References
1. Losanoff JE, Richman BW, Jones JW. Obturator hernia. J Am Coll Surg. 2002;194(5):657-63. [ Links ]
2. Rodríguez-Hermosa JI, Codina-Cazador A, Maroto-Genover A, Puig-Alcántara J, Sirvent-Calvera JM, Garsot-Savall E, Roig-García J. Obturator hernia: clinical analysis of 16 cases and algorithm for its diagnosis and treatment. Hernia. 2008;12(3):289-97. [ Links ]
3. Haraguchi M, Matsuo S, Kanetaka K, Tokai H, Azuma T, Yamaguchi S, Kanematsu T. Obturator hernia in an ageing society. Ann Acad Med Singapore. 2007;36(6):413-5. [ Links ]
4. Pandey R, Maqbool A, Jayachandran N. Obturator hernia: a diagnostic challenge. Hernia. 2009;13(1):97-9. [ Links ]
5. Nakayama T, Kobayashi S, Shiraishi K, Nishiumi T, Mori S, Isobe K, Furuta Y. Diagnosis and treatment of obturator hernia. Keio J Med. 2002;51(3):129-32. [ Links ]

