










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 n.3 Madrid Mar. 2011
LETTERS TO THE EDITOR
Exceptional vascular complication during ERCP: cannulation of the hepatic artery
Complicación vascular excepcional durante la colangiopancreatografía retrógrada endoscópica: canulación de la arteria hepática
Key words: ERCP. Hepatic artery. Pancreatic cancer. Bleeding. Hemobilia. Haemostasis.
Dear Editor,
The most frequent complications of endoscopic retrogra-de cholangiopancreatography (ERCP) and endoscopic biliary sphincterotomy are pancreatitis, cholangitis, hemorrhage, and duodenal perforation. A number of less common complications have also been described including vascular (portal vein, periampullary lymphatic system, hepatic artery) opacification in only small numbers of patients or in individual cases (1-6). The present case report describes an accidental hepatic artery cannulation following ERCP. We discuss the possible pathogenic mechanism, the risks and the endoscopic management to achieve the hemostasis.
Case report
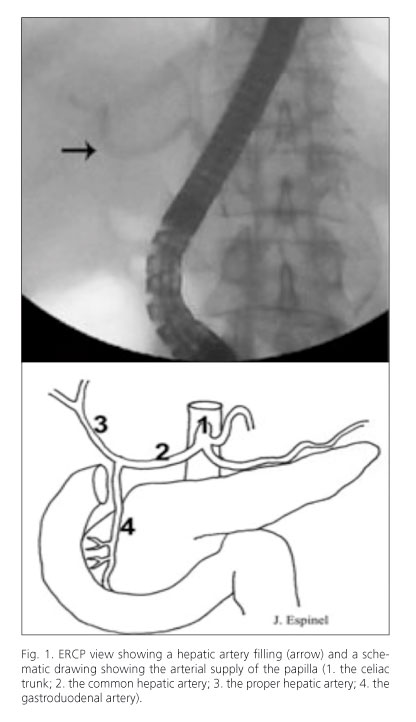
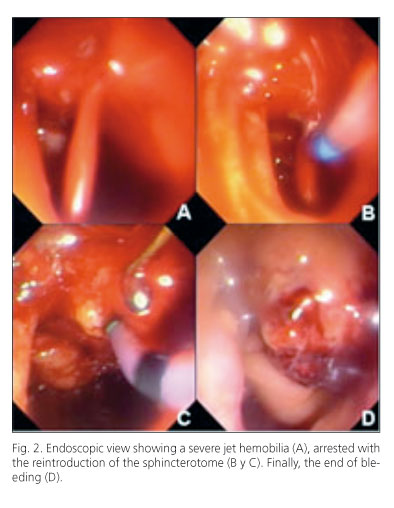
An 84-year-old man with a history of diabetes mellitus, severe chronic obstructive lung disease, arterial hypertension, abdominal aneurysm, cholecistectomized, was admitted to hospital due to a biliary obstruction. A computerized tomography (CT) scan revealed a pancreatic mass and a fine-needle aspiration (FNA) confirmed an adenocarcinoma. ERCP showed a papilla with infiltrative aspect. Papilla was cannulated with a sphincterotome wire-guided (sphincterotome CT-25M, Cook; and Jagwire 0,35 in. Boston Scientific). A small amount of contrast dye was injected and the hepatic artery was opacified (Fig. 1). The retrieval of the sphincterotome was followed by a severe spurting hemobilia, stopped with the reintroduction of the sphincterotome (Fig. 2). Two minutes afterwards, a new retrieval of the sphincterotome caused an important rebleeding which required a new reintroduction of the sphincterotome in the papilla during 20 minutes long. In the last retrieval, rebleeding was not observed. The patient was monitored, remaining stable during the next days. He was discharged six days afterwards, with a biliary metal stent drainage performed percutaneously.
Discussion
The celiac trunk is the common output from the abdominal aorta of three arteries: the left gastric artery, the splenic artery and the common hepatic artery. The common hepatic artery extends to the liver by partially irrigating the stomach, duodenum and pancreas. This artery gives rise to the gastroduodenal artery and proper hepatic artery. The arterial supply of the papilla derives from branches of the gastroduodenal artery (Fig. 1). Vascular cannulations during ERCP, mainly of the portal system (1-5) have been exceptionally reported. In these cases, most of the patients had pancreatic cancer. It is possible that the presence of aberrant vessels due to a neoplasia may favour this complication. Only one case of accidental cannulation of the hepatic artery during ERCP (6), similar to ours, has been described in the literature until now. Our patient had a pancreatic cancer. The presence of aberrant vessels and/or the anatomic alteration resulting from the cancer, or a direct trauma to the papilla (precut, wire, etc.) may explain the hepatic artery cannulation with the wire through the gastroduodenal artery. Mechanical haemostasis with the sphincterotome permits a successful control of the bleeding. Filling of arterial, portal, or lymphatic vessels has several potential risks like sepsis, air embolism, bleeding, or thrombosis. Failed prompt recognition of contrast in vascular structures may cause confusion leading to the prolongation of the procedure, thereby increasing the risk of further complications. An opacified hepatic artery may be misinterpreted as an incompletely filled bile duct. Insertion of a stent into the hepatic artery may worsen the consequences. Aspiration of the duct before the contrast injection and image recording might aid for immediate diagnosis.
Jesús Espinel1, Eugenia Pinedo2, Gabriela Rascarachi1 and Carmen Bailador3
Departments of 1Endoscopy and 2Radiology. Hospital de León. Spain. 3Department of Endoscopy. Hospital Virgen de la Concha. Zamora, Spain
References
1. Huibregtse K, Gish R, Tytgat GN. A frightening event during endoscopic papillotomy. Gastrointest Endosc 1988;34:67-8. [ Links ]
2. Ben-Zvi JS, Siegel JH, Yatto R. Opacification of the portal system during ERCP: demonstration of an anomalous pancreatico-portal connection in a patient with pancreatic carcinoma. Gastrointest Endosc 1989;35:445-7. [ Links ]
3. Ricci E, Mortilla MG, Conigliaro R, Bertoni G, Bedogni G, Chilovi F. Portal vein filling: a rare complication associated with ERCP for endoscopic biliary stent placement. Gastrointest Endosc 1992;38:524-5. [ Links ]
4. Cotton PB. Portal vein filling during ERCP. Gastrointest Endosc 1994;40:120-1. [ Links ]
5. Espinel J, Pinedo ME, Calleja JL. Portal vein filling: an unusual complication of needle-knife sphincterotomy. Endoscopy 2007;39(Supl. 1):E245. [ Links ]
6. Gottschalk U, Morgenstern C, Kadow K. Accidental cannulation of the hepatic artery following needle-knife sphincterotomy. Z Gastroenterol 2007;45:702. [ Links ]

