










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.5 Madrid May. 2015
PICTURES IN DIGESTIVE PATHOLOGY
Poorly differentiated early gastric adenocarcinoma of mixed type with "crawling" pattern of extension
Alejandro Rubio-Fernández1, Mario Díaz-Delgado1, Alicia Hernández-Amate1 and Tomás García-Guerrero2
Department of 1Pathology and 2Gastroenterology. Complejo Hospitalario Universitario de Badajoz. Badajoz, Spain
Case report
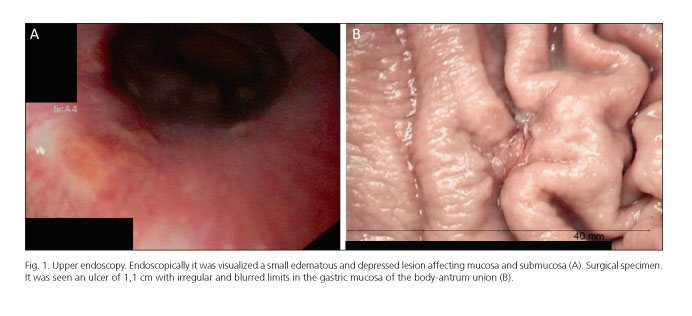
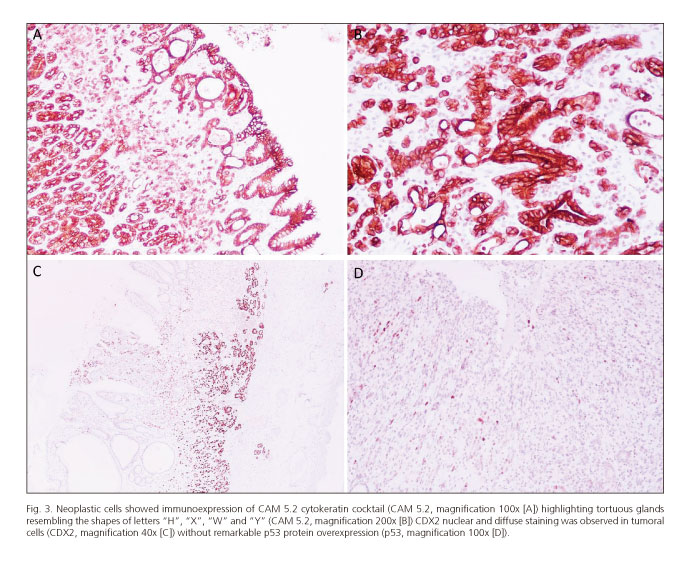
We report a case of a 56-year-old female patient with a gastric ulcer at study with an associated gastroesophageal reflux. There was no previous familiar history of interest. Endoscopically, it was visualized an edematous and ulcerated lesion affecting mucosa and submucosa (Fig. 1A). A first biopsy was performed showing nearly normal gastric mucosa with scant infiltrating cells with vacuolated cytoplasm and polarized hyperchromatic nuclei, with signet ring cell morphology, occupying the lamina propria. Moreover, some glands were dilated displaying a branching pattern with intraluminal neutrophilic abscesses. The diagnosis was suspicious for adenocarcinoma. Four months later, a new endoscopic study and a biopsy were performed. At this time, the lesion showed dilated and branching glands admixed with poorly formed glands creating complex shapes ("H", "X", "W", "Y") which were intermingled with cords of vacuolated signet ring cells. The diagnosis was adenocarcinoma with signet ring cell features. Finally, a partial gastric resection was done. In the gastric mucosa of the posterior aspect of the body-antrum union it was seen an ulcerated lesion of 1.1 cm with irregular and blurred limits (Fig. 1B). Histologically, it was observed a proliferation of poorly defined glands with lateral spreading along the mucosa (Fig. 2A, arrows) and focally infiltrating the submucosa. The superficial glands were distended with intraluminal neutrophilic abscesses and were branched delimiting anastomosing and tortuous structures with focal spiky borders (Fig. 2 B and C). The glands, which presented dystrophic goblet cells and hyperchromatic nuclei, were intimately admixed with single cells with signet ring features (Fig. 2D). Several mitotic figures were observed. Immunohistochemically, the neoplastic cells expressed CAM 5.2 (Fig. 3 A and B), E-cadherin, Heppar-1, Glypican-3 and CDX2 (Fig. 3C) defining an intestinal phenotype. p53 was not overexpressed in tumor cells (Fig. 3D). No signs of chronic gastritis, intestinal metaplasia or H. pylori were seen. The final diagnosis was poorly differentiated early gastric adenocarcinoma of mixed type (Lauren classification) with crawling lateral extension (pT1b).

Discussion
Early gastric cancer (EGC) is a type of gastric carcinoma (GC) defined as the one that is confined to the mucosa or submucosa, irrespective of lymph node status, corresponding to pT1a (lamina propria and muscularis mucosae) and pT1b (submucosa). This term relates to a gastric cancer in a potentially curable stage with an average 5-year survival after surgery of nearly 95% (1). Although the real incidence of EGC in Western countries is actually unknown, in the last decades several studies have reported incidence rates of 20.8%-37,8% of all gastric carcinomas (2). Although this type of cancer has been extensively studied in Japanese population the occidental pathologists have less experience diagnosing such kind of lesions. Besides, the recent paper of Ushiku et al. (3) describe a new variant of GC: The very-well differentiated gastric carcinoma of intestinal type (VWDGC-IT), which accounts only for the 1.9% of EGC. This kind of GC actually presents at endoscopy as an ill-defined lesion with an indistinct border and a slightly depressed or flat appearance without marked mucosal tinctorial alteration. It is characterized by a low grade nuclear atypia and a morphology mimicking intestinal metaplasia with an unique lateral spread of pattern (crawling type) (4). The neoplastic glands frequently show architectural changes such as branching, anastomosis, dilatation, spiky borders, abortive forms, glandular overgrowth and discohesive cells recreating the shapes of letters "H", "X", "W" and "Y". This type of GC is particularly difficult to diagnose in biopsy specimens being easily confused with reactive intestinal metaplasia (3), a magnified situation given that the treatment of EGC is increasingly done by endoscopic biopsy (2). Immunohistochemically it has been reported an intestinal phenotype (MUC2, CD10 and CDX2) in the 52% of cases and a mixed phenotype, with markers of gastric (MUC5AC and MUC6) and intestinal phenotype in the 48% of VWDGC. Although it is thought that VWDGC-IT represents a type of EGC with a low malignant potential with slow growth and good prognosis, there are cases reported with transformation into diffuse-type morphology resulting in a more aggressive behaviour. Moreover, in the review of 58 cases of VWDGC owning to previous series done by Ushiku et al. (3) no examples of intestinal phenotype had discohesive neoplastic cells indicative of a poorly cohesive component, whereas 69% of cases with mixed phenotype presented at least a focus of poorly cohesive carcinoma. Amongst them, 5 of 58 cases with mixed phenotype and a poorly cohesive carcinoma component had concurrent lymph node metastases. Due to the endoscopic and histological difficulties diagnosing this neoplasms with a rate of almost 50% of initial biopsies incorrectly interpreted as "indeterminate for neoplasia" or "reactive intestinal metaplasia" with a delay in diagnosis of 1 year in nearly 17% of cases, it is imperative to become familiar with this rare and peculiar type of EGC (3).
References
1. Fletcher CDM. Diagnostic Histopathology of Tumors. 4th ed. Philadelphia: Elsevier Saunders; 2014. [ Links ]
2. Bollschweiler E, Berlth F, Baltin C, et al. Treatment of early gastric cancer in the Western World. World J Gastroenterol 2014;20:5672-8. [ Links ]
3. Ushiku T, Arnason T, Ban S, et al. Very well-differentiated gastric carcinoma of intestinal type: Analysis of diagnostic criteria. Mod Pathol 2013;26:1620-31. [ Links ]
4. Okamoto N, Kawachi H, Yoshida T, et al. "Crawling-type" adenocarcinoma of the stomach: A distinct entity preceding poorly differentiated adenocarcinoma. Gastric Cancer 2013;16:220-32. [ Links ]

