










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.5 Madrid May. 2015
LETTERS TO THE EDITOR
Primary hepatic neuroendocrine tumor in a patient with acute HBV hepatitis: An unusual neoplasia
Tumor neuroendocrino primario hepático en paciente con hepatitis aguda VHB: una neoplasia inusual
Key words: Primary hepatic neuroendocrine tumor. Hepatitis B. Liver tumor.
Palabras clave: Tumor neuroendocrino primario hepático. Hepatitis B. Tumor hepático.
Dear Editor,
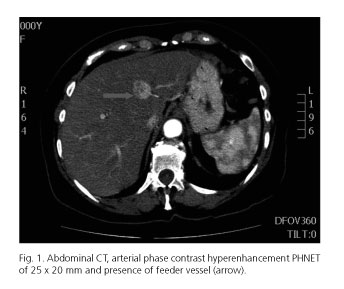
We present the case of a 67-year-old woman with no previous medical history, with a flu-like clinic of 14 days, associated with arthralgia and jaundice. Additional tests showed hyperbilirubinemia (TB: 12.03 mg/dL) and liver enzymes with a hepatocellular injury pattern (AST: 1906 IU/L, ALT: 1611 IU/L). Studies were conducted, with viral markers: HBsAg: 1351; HBeAg: 12.39; HBc IgM: 27.17 and HBV DNA-426, and abdominal ultrasonographic: Solid liver lesion (SLL) in segment IV adjacent to the portal vein of 21x17 mm. With the diagnosis of acute VHB hepatitis and SLL, diagnostic tests were extended. The abdominal CT (Fig. 1) and MRI showed the lesion described between segments III and IV suggestive of hepatocellular carcinoma.
Liver biopsy (FNA) was performed giving a result of periportal and lobular chronic hepatitis, the SLL biopsy could not be performed due to its location.
After the conversion to negative of HBsAg and HBc, the anti-HBs positivity (acute hepatitis cured) and facing the suggestive HCC lesion, resection of segment IVa was performed, with intraoperative ultrasound that ruled out cirrhosis and other intrahepatic tumors. Highly favorable postoperative course, patient discharged on the fourth postoperative day. Pathology described a 3x3x2.5 cm tumor with poorly defined edges and free margins. Histological examination showed organoid architecture and travecular areas with cellular elements of round nuclei with clumped chromatin, and immunohistochemical techniques showed synaptophysin +, chromogranin -, and a proliferation rate of 5% compatible with a nonfunctioning primary hepatic neuroendocrine tumor (PHNT).
Given the findings, a PET-SCAN was made without observing other injuries and chromogranin A was in normal range.
Two years after surgery, the patient has had no recurrence.
Discussion
The primary location in the liver of neuroendocrine tumors is rare, because when the liver presents such tumors, the disease is usually metastatic (more than 80% are metastases) (1). The PHNT represents 0.3% of neuroendocrine tumors (2). They appear in middle-aged population (40-50 years) with no sex predilection. Usually at diagnosis, the tumors are large because most are asymptomatic; if there are symptoms, these are strain or right upper quadrant pain, weight loss, fatigue and fever (3) and they do not usually have carcinoid syndrome (4).
Some authors have reported cases of PHNT in patients with previous liver disease (hepatitis B or cirrhosis), but an association between the two has not been demonstrated (5,6).
The differential diagnosis is made with hepatocellular carcinoma and intrahepatic cholangiocarcinoma, showing negativity for markers such as AFP, CEA and CA 19-9 (3). Blood serotonin, chromogranin A, or 5-hydroxyindoleacetic acid in urine may be high (6). The imaging tests most commonly used are ultrasound, CT and MRI. The octreoscan and PET-CT with 18F-FDG can detect tumors up to 2 mm and occult foci (6). The final diagnosis needs histological confirmation with generally positive immunohistochemistry for chromogranin A, neuro-specific enolase, and synaptophysin (7,8) and requires to fulfill another premise: exclude extrahepatic localization, since in that case it would then be a metastasis (3,5,9).
Surgery with complete resection is the accepted treatment for PHNT, with recurrences of 18% and survival at 5 years of 74-78% (3,9,10).
Germán Mínguez-Ruiz1, Carmen García-Bernardo1, Jimi Harold Jara-Quezada1,
Raquel Rodríguez-Uria1, M.a Luisa González-Diéguez1 and Lino Vázquez-Velasco1
Departments of 1General Surgery and 2Digestive Diseases.
Hospital Universitario Central de Asturias. Oviedo, Spain
References
1. Modlin IM, Sandor A. An analysis of 8305 cases of carcinoid tumors. Cancer 1997;79:813-29. [ Links ]
2. Fenoglio LM, Severini S, Ferrigno D, et al. Primary hepatic carcinoid: A case report and literature review. World J Gastroenterol 2009; 15:2418-22. [ Links ]
3. Zhu H, Sun K, Ward SC, et al. Primary hepatic signet ring cell neuroendocrine tumor: A case report with literature review. Semin Liver Dis 2010;30:422-8. [ Links ]
4. Modlin IM, Kidd M, Latich I, et al. Current status of gastrointestinal carcinoids. Gastroenterology 2005;128:1717-51. [ Links ]
5. Jia C, Zhang Y, Xu J, et al. Experience in primary hepatic neuroendocrine tumor. Turk J Gastroenterol 2012;23:546-51. [ Links ]
6. Huang YQ, Xu F, Yang JM, et al. Primary hepatic neuroendocrine carcinoma: Clinical analysis of 11 cases. Hepatobiliary Pancreat Dis Int 2010;9:44-8. [ Links ]
7. Dala R, Shoosmith J, Lilenbaum R, et al. Primary hepatic neuroendocrine carcinoma: An underdiagnosed entity. Ann Diagn Pathol 2006;10:28-31. [ Links ]
8. Erickson LA, Lloyd RV. Practical markers used in the diagnosis of endocrine tumors. Adv Anat Pathol 2004;11:175-89. [ Links ]
9. Knox CD, Anderson CD, Lamps LW, et al. Long-term survival after resection for primary hepatic carcinoid tumor. Ann Surg Oncol 2003;10:1171-5. [ Links ]
10. Woodside KJ, Townsend CM, Evers BM. Current management of gastrointestinal carcinoid tumors. J Gastrointest Surg 2004;8:742-56. [ Links ]

