










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.6 Madrid Jun. 2015
PICTURES IN DIGESTIVE PATHOLOGY
Pseudoaneurysm of the cystic artery: An uncommon cause of upper gastrointestinal bleeding in a case of xanthogranulomatous cholecystitis
A propósito de un caso de pseudoaneurisma de la arteria cística: causa infrecuente de hemorragia digestiva alta en un cuadro de colecistitis xantogranulomatosa
Carmen Muñoz-Villafranca1, Íñigo García-Kamirruaga1, Pilar Gómez-García2, Víctor Atín-del-Campo2, Victoria Bárcena-Robredo3, Alexander Aguinaga-Alesanco4 and Ángel Calderón-García1
Departments of 1Gastroenterology, 2Surgery and 3Diagnostic Radiology. Hospital Universitario de Basurto. Bilbao, Vizcaya. Spain.
4Department of Diagnostic Radiology. Hospital Universitario de Cruces. Baracaldo, Vizcaya. Spain
Pseudoaneurysm of the cystic artery is a very rare entity; only a few cases have been reported in the literature (1).
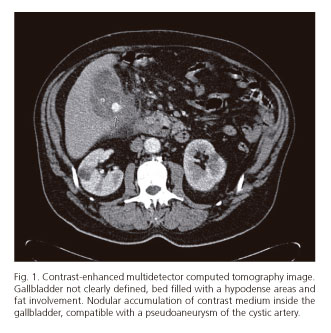
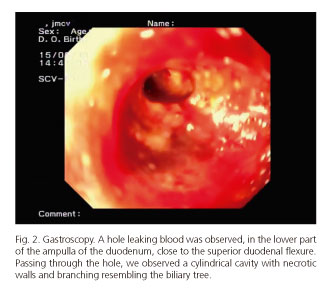
We present the case of a 74-year-old male admitted for pain in the right lower quadrant of the abdomen. The emergency abdominal CT scan showed abnormal structural findings in the gallbladder, with hypodense area, cholelithiasis, and involvement of the fat around the gallbladder. The findings suggesting xanthogranulomatous cholecystitis were confirmed by needle aspiration cytology. His course was unsatisfactory and, on day 14, he had an episode of pain in the upper gastrointestinal tract and melaena. The suspicion of haemobilia was confirmed by endoscopy. In the lower part of the ampulla of the duodenum, we identified a leaky hole into a cylindrical cavity and observed branching compatible with the biliary tree (Fig. 2).
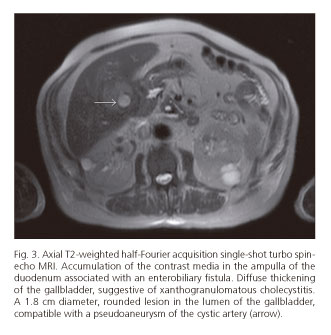
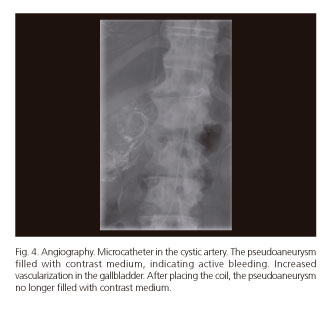
Magnetic resonance imaging showed a 1.8 cm lesion compatible with a pseudoaneurysm of the cystic artery (Fig. 3). Given the severity of the bleeding, selective embolisation of the cystic artery was performed on an emergency basis, by selective catheterisation of the hepatic artery and supraselective catheterisation of the cystic artery. We used 500 to 700 µm Contour Microspheres and three coils (Fig. 4), and succeeded in stopping the haemorrhage immediately.
Despite the high incidence of biliary diseases in our setting, there are very few cases of digestive haemorrhage due to haemobilia (2). Although the origin of the pseudoaneurysm is not clear, it seems that erosion of the artery wall, due to inflammatory processes associated with cholecystitis, could have led its formation (3). As for the treatment of choice, most authors recommend arteriography with selective embolisation by interventional radiology (4).
References
1. Komatsu Y, OritoH, Sakurada M, et al. Report of a case: Pseudoaneurysm of the cystic artery with hemobilia treated by arterial embolization. Journal of Medical Cases 2011;2:178-83. [ Links ]
2. Sousa HT, Amaro P, Brito J, et al. Hemobilia due to pseudoaneurysm of the cystic artery. Gastroentérologie Clinique et Biologique 2009;33:80-2. [ Links ]
3. Anand U, Kumar ThaKur S, Kumar S, et al. Idiopathic cystic artery aneurysm complicaded with hemobilia. Annals Of Gastroenterology 2011;24:134-6. [ Links ]
4. Ahmed I, Tanveer UH, Sajjad Z, et al. Cystic artery pseudoaneurysm: A complication of xantogranulomatous cholecystitis. B J Radiology 2010;83:165-7. [ Links ]

