










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.2 Madrid Feb. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Endoscopic removal of multiple sharp gastro-duodenal foreign bodies
Samuel Costa1, Raquel Gonçalves1 and Carla Rolanda1,2,3
1Department of Gastroenterology. Hospital de Braga. Braga, Portugal.
2Life and Health Sciences Research Institute. University of Minho. Braga, Portugal.
3ICVS/3B's-PT Government Associate Laboratory. Braga-Guimarães, Portugal
Case report
A 45-year-old female, with bipolar disorder, was brought to the Emergency Department with abdominal pain. The patient was hemodynamically stable, with no signs of respiratory distress. On abdominal examination, she had pain in the upper quadrants without peritoneal irritation.
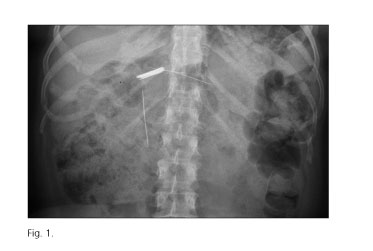
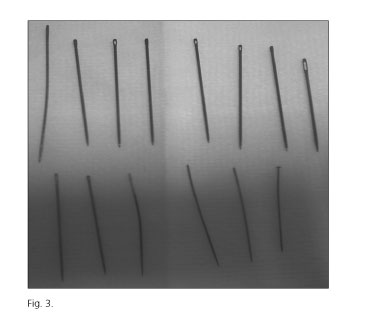
A plain abdominal X-ray revealed multiple linear opacities in the epigastric region, one of them in a more distal position, with no evidence of pneumoperitoneum (Fig. 1). Upper GI endoscopy displayed linear ulcerations scattered throughout the esophagus and the stomach; it also confirmed the presence of several needles and a pin huddled in the gastric body (Fig. 2), as well as another needle stuck in the second duodenal portion. With the patient under anesthesia, thirteen sewing needles and a pin were endoscopically removed (Fig. 3). The sharp end of the needle was grasped, aligned with the endoscope working channel, using smooth movements and suction; once inside it was removed all in block under continuous suction. The patient started liquids 12 hours after the procedure and was referred for further psychiatric evaluation.

Discussion
Successful endoscopic removal decreases in case of delayed approach, beyond 12 hours, and sharp objects (1). Besides, sharp objects, even if already into the stomach or duodenum, should be retrieved endoscopically as long as it can be accomplished safely, because the risk of a complication during their natural exteriorization is as high as 35% (2). Extreme caution is required as the wall of the gastrointestinal tract can be easily injured. For this purpose one method involves using an overtube to protect the esophagus and another technique fashioning a protective hood. Instead, we were able to remove all the needles without complication using the method described above. Lately we found in literature a similar description although using a sheath (3), which is a good option to obviate any risk for the endoscope.
References
1. Hong KH, Kim YJ, Kim JH, et al. Risk factors for complications associated with upper gastrointestinal foreign bodies. World J Gastroenterol 2015;21:8125-31. [ Links ]
2. ASGE Standards of Practice Committee, Ikenberry SO, Jue TL, et al. Management of ingested foreign bodies and food impactions. Gastrointest Endosc 2011;73:1085-91. DOI: 10.1016/j.gie.2010. 11.010. [ Links ]
3. Enjoji A1, Nagata Y, Furuichi A, et al. Successful removal from the duodenum of swallowed sewing needles using devised endoscopic forceps. Endoscopy 2004;36:193. DOI: 10.1055/s-2004-814194. [ Links ]
