










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.3 Madrid Mar. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Combined endoscopic resolution of iatrogenic stricture in an ureterosigmoidostomy
Resolución endoscópica combinada de una estenosis yatrógena en una ureterosigmoidostomía
Alberto Mir-Subías, Mónica Navarro-Dourdil, Mara Charro-Calvillo and Juan José Sebastián-Domingo
Department of Digestive Diseases. Hospital Royo Villanova. Zaragoza, Spain
Introduction
Ureteroenterostomy allows the replacement of the bladder role after radical cystectomy. Anastomotic stricture is a relatively common complication that may require surgical repair. We report a case of iatrogenic stricture in a Mainz-II ureterosigmoidostomy (1) that was satisfactorily resolved using a combined endoscopic-urological approach (2,3).
Case report
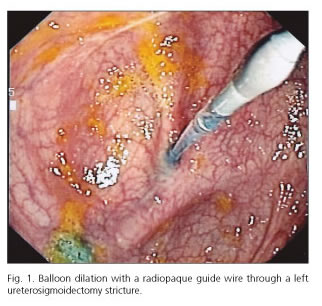
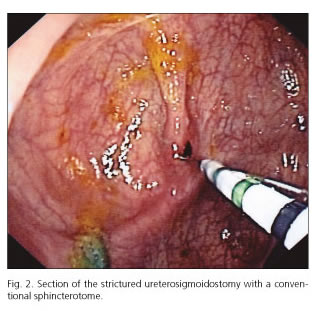
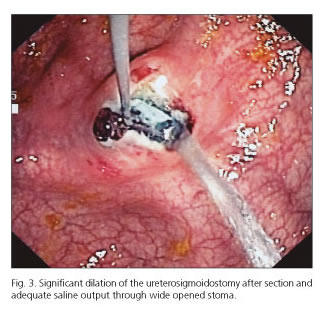
A 47-year-old male diagnosed with bladder adenocarcinoma was treated with intestinal bypass, Mainz II type. During a subsequent colonoscopy, two sessile polypoid lesions were excised, which were eventually identified as ureterosigmoidostomy-related granulomas. Follow-up revealed a ureteral dilation and anastomotic stricture in the left ureter secondary to "polypectomy"-associated scarring. Radio-guided surgery using a combined urologic-endoscopic approach was selected for treatment. A radiopaque guidewire was passed via a left nephrostomy through the strictured stoma to the sigmoid colon. Endoscopically, a 6-mm-in-diameter dilation balloon was passed over the wire, which failed to significantly increase the stricture caliber. Eventually, a decision was made to widen the stricture using a conventional sphincterotome, which significantly opened the anastomosis and allowed verification of saline output. The patient had a very satisfactory outcome.
Discussion
In cases of ureterosigmoidostomy-related stricture, in this case iatrogenically induced by a "polypectomy" of scarring tissue (granuloma) at the anastomosis, which resulted in progressive fibrosis and stenosis at the stoma, repair may be attempted with a combined endoscopic technique, rendering repeated surgery unnecessary.
References
1. Fisch M, Wammack R, Hohenfellner R. The sigma rectum pouch (Mainz pouch II). World J Urol 1996;14(2):68-72. DOI: 10.1007/BF00182560. [ Links ]
2. Del Hoyo Campos J, Burgos Revilla FJ, Lovaco Castellano F, et al. Endourologic treatment of uretero-ileal stenosis. Arch Esp Urol 1995;48(7):735-40. [ Links ]
3. Kurzer E, Leveillee RJ. Endoscopic management of ureterointestinal strictures after radical cystectomy. J Endourol 2005;19(6):677-82. DOI: 10.1089/end.2005.19.677. [ Links ]
