










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.5 Madrid May. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Cystic duct cyst lesions (type VI)
Lesiones quísticas del conducto cístico (lesiones tipo VI)
Gloria Paseiro-Crespo, María García-Nebreda, Elia Marqués-Medina and Edurne Álvaro-Cifuentes
Department of General Surgery and Digestive Diseases. Hospital Universitario Infanta Leonor. Madrid, Spain
Case report
A 60-year-old woman with no past medical history was diagnosed with an extrahepatic bile duct dilatation by ultrasound. The study was completed with a computed tomography (CT) scan that confirmed the existence of a cystic image of 2 cm in diameter near the gallbladder, with proximal extrahepatic bile duct dilatation.
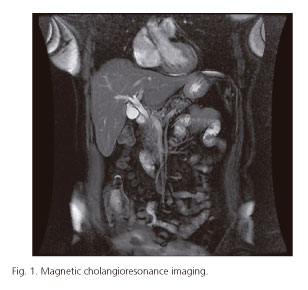
The magnetic resonance imaging also showed dilatation of the bile duct without any apparent reason. The cystic duct was slightly beaded, and a cystic lesion of approximately 2 cm in diameter was identified behind the gallbladder. It reached the cystic bile duct, but it did not communicate with it (Fig. 1).
Exploratory laparoscopy was performed, finding a normal gallbladder with saccular cystic dilatation, which affected only its origin without distal involvement. The histopathologic study led to a diagnosis of a cystic duct cyst (Fig. 2).

Discussion
Todani proposed the most accepted classification for cystic lesions of the bile duct, including five types (1). Serena described another one, type VI, which includes cystic lesions of the isolated cystic duct, of which there are less than 20 reported cases. They differ from type II in terms of the distal cystic caliber, which is normal in type VI, and in the diagnosis, which is performed intra-operatively in most of the cases (2).
Neoplastic degeneration has an incidence of 10-30% in all these lesions, which is the reason why the most widely accepted treatment is cholecystectomy with resection of the cystic duct cyst dilatation and preservation of the main bile duct by laparoscopic approach (3).
References
1. Todani T, Watnabe Y, Narusue M, et al. Congenital bile duct cysts. Classification, operative procedures and review of thirty seven cases including cancer arising from choledochal cyst. Am J Surg 1977;134:233-69. [ Links ]
2. Serena Serradel AF, Santamaría LE, Herrera GR. Cystic dilatation of the cystic duct: A new type of biliary cyst. Surgery 1991;109:320-2. [ Links ]
3. Maheshwari P. Cystic malformation of cystic duct: 10 cases and review of literature. World J Radiol 2012;28:4(9):413-7. DOI: 10.4329/wjr.v4.i9.413. [ Links ]
