










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.5 Madrid May. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Hepatocellular carcinoma in a non-failing Fontan circulation
Efrén Martínez-Quintana1, Alberto Monescillo2 and Fayna Rodríguez-González3
1Department of Cardiology. Complejo Hospitalario Universitario Insular-Materno Infantil. Las Palmas de Gran Canaria, Spain.
2Department of Digestive Diseases. Complejo Hospitalario Universitario Insular-Materno Infantil. Las Palmas de Gran Canaria, Spain.
3Hospital Universitario de Gran Canaria de Gran Canaria Doctor Negrín. Las Palmas de Gran Canaria, Spain
Case report
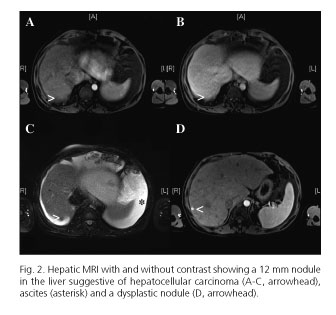
A 41-year-old woman with a tricuspid atresia and a pulmonary stenosis operated on at eight years old with a classic Fontan operation was referred for evaluation due to ascites without limb edemas. Cardiac magnetic resonance imaging (MRI) showed a rudimentary right ventricle (RV) and a giant right atria (RA) with the right atrial appendage (arrowhead) connected to the pulmonary artery (PA) (Fig. 1A). Abdominal MRI showed the liver with parenchymal heterogeneity, dilatation of the suprahepatic veins (SHV) and ascites (asterisk) (Fig. 1B). Hepatic MRI with and without contrast showed a 12 mm nodule in the liver suggestive of hepatocellular carcinoma (Fig. 2 A-C, arrowhead) according to the European Association for the Study of the Liver (1), ascites (asterisk) and a dysplastic nodule (Fig. 2D, arrowhead). No significant gastro-esophageal varices were seen. Hemodynamic evaluation showed a SHV pressure of 14 mmHg and a hepatic venous pressure gradient of 2 mmHg with no stenoses in the Fontan pathway. Serum-ascites albumin gradient was < 1. Liver biopsy was rejected due to the high risk of bleeding. Unfortunately, whilst waiting for chemotherapy embolization the patient died.

Discussion
Patients after a Fontan operation exhibit some degree of fibrosis which are primarily located in a sinusoidal or centrilobular pattern. Cirrhosis may develop years later and the incidence of cancer is up to 5% (2). That is why some authors recommend that patients who are > 10 years out from their Fontan operation should undergo cardiac assessment as well as the determination of alpha-fetoprotein level, the realization of liver imaging tests or even liver biopsy (3) to stay ahead of neoplastic transformation.
References
1. Llovet JM, Ducreux M, Lencioni R, et al. European Association for Study of Liver; European Organization for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. Eur J Cancer 2012;48:599-641. DOI: 10.1016/j.ejca.2011.12.021. [ Links ]
2. Asrani SK, Warnes CA, Kamath PS. Hepatocellular carcinoma after the Fontan procedure. N Engl J Med 2013;368:1756-7. DOI: 10.1056/NEJMc1214222. [ Links ]
3 Rychik J, Veldtman G, Rand E, et al. The precarious state of the liver after a Fontan operation: Summary of a multidisciplinary symposium. Pediatr Cardiol 2012;33(7):1001-12. DOI: 10.1007/s00246-012-0315-7. [ Links ]
