










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.110 n.3 Madrid Mar. 2018
https://dx.doi.org/10.17235/reed.2017.5197/2017
PICTURES IN PATOLOGY DIGESTIVE
Chilaiditi syndrome complicated by a sigmoid volvulus and hepatic displacement
1Servicios de Aparato Digestivo. Hospital Universitario La Paz. Madrid, España
2Servicios de Radiodiagnóstico. Hospital Universitario La Paz. Madrid, España
CASE REPORT
A female patient aged 78 years with COPD presented with dyspnea, epigastric pain and a saturation of 86%. A computed tomography (CT) scan showed an obstruction by the sigmoid volvulus which exerted a marked mass effect on the liver, which in turn was displaced towards the left hemi-abdomen. An endoscopic decompression performed by colonoscopy was effective and the patient had a good clinical evolution (Fig. 1, Fig. 2 y Fig. 3).
DISCUSSION
Chilaiditi's sign is an anatomical alteration that consists of the transposition of the small intestine or colon between the liver and the diaphragm. The condition is asymptomatic and is usually an incidental radiological finding. It is a rare entity with an incidence of 0.025% 1 for all radiological examinations. The onset of Chilaiditi syndrome is accompanied by clinical symptoms such as abdominal pain and dyspnea. Moreover, the combination of the sigmoid volvulus and Chilaiditi syndrome is extremely rare, with only 17 previously published cases. The rarity of the aforementioned combination, together with the fact that both conditions share common predisposing factors, suggests a casual association rather than a cause-effect relationship. The factors that favor this association are presumed to include elongation and hypermotility of the colon together with a long mesentery, chronic constipation and prior abdominal surgery 2. The "mobile" liver is an unusual situation where the liver can move in the transversal plane due to the laxity or absence of supporting ligaments 3, which is associated with the conditions described above. Most cases require surgical treatment and endoscopic treatment was successful in this case.
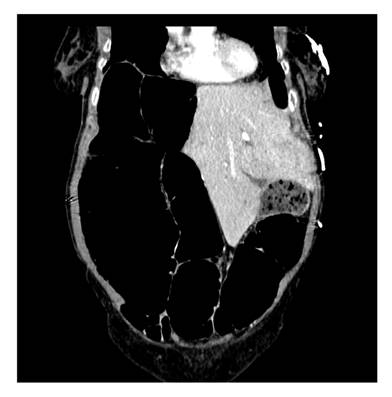
Fig. 1 Abdominal CT scan. Coronal slice. An atypical sigmoid colon can be seen that occupies the entire right flank. The sigmoid volvulus exerts a marked mass effect on the intra-abdominal structures, especially the liver, which is displaced towards the left hemi-abdomen. The wall of the colon structure is thinner, probably due to the marked distension, which exhibits a normal enhancement.

Fig. 2 Abdominal CT scan. Axial slice. A marked distension of the sigmoid colon with thinned colonic walls is noticeable. This results in a significant displacement of the liver towards the left hypochondrium which has caused a complete collapse of the intrahepatic portion of the inferior vena cava.
BIBLIOGRAFÍA
1. Flores N, Ingar C, Sánchez J, et al. The Chilaiditi syndrome and associated volvulus of the transverse colon. Rev Gastrenterol Peru 2005;25(3):279-84. [ Links ]
2. Kurt Y, Demirbas S, Bilgin G, et al. Colonic volvulus associated with Chilaiditi's syndrome: Report of a case. Surg Today 2004;34:613-5. DOI: 10.1007/s00595-004-2751-3 [ Links ]
3. Kaggwa S, Ssenyonjo A, Nassali G, et al. The wandering liver: A case report and review of literature. East Cent African J Surg 2012;17(1)130-5. [ Links ]
