










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.110 n.12 Madrid Dec. 2018
https://dx.doi.org/10.17235/reed.2018.5642/2018
SCIENTIFIC LETTERS
A giant abdominal collection: when things are not what they seem
1Unidad de Endoscopia Digestiva. Unidad de Gestión Clínica de Enfermedades Digestivas. Hospital Universitario de Valme. Sevilla, Spain
Key words: Drainage. Endoscopic ultrasound; Lumen-apposing metal stents; Hydatid cyst
Dear Editor,
Endoscopic ultrasound-guided transluminal drainage (EUS-TD) has become the standard of care for the treatment of peripancreatic fluid collections (PFCs). New lumen-apposing metal stents (LAMS) have facilitated the drainage technique 1). However, this fact should not cloud our view when planning a EUS-TD, as occasionally things are not what they seem.
Case report
A 53-year-old male heavy drinker was admitted due to abdominal pain and early satiety sensation of a one-year duration. Physical examination revealed a painful massive bulging abdomen. Laboratory studies did not identify anything clinically relevant. Computed tomography (CT) scan identified a 22 x 25 cm encapsulated liquid collection that occupied the entire abdominal cavity (Fig. 1A). Due to the alcoholic nature of the patient, a pancreatic pseudocyst was suspected and a EUS-guided drainage was performed. A 15 mm diameter LAMS (Hot-AXIOS(tm) Boston Scientific, Marlborough, MA, USA) was placed. Biochemical analysis of the liquid revealed amylase levels of 0. A new CT scan showed membranous images inside the lesion, suggestive of a hydatid cyst (Fig. 1B). Treatment with intravenous albendazol at 10 mg/kg/day was started. Greenish membranes that carpeted the wall were identified within the lesion. A nasocystic drainage with a saline hypertonic continuous perfusion was placed and a marked reduction in the number of membranes was observed, although the wall of the cavity did not show major changes (Fig. 1C). Surgery demonstrated the hepatic origin of the cyst and the germinal membrane was removed (Fig. 1D).
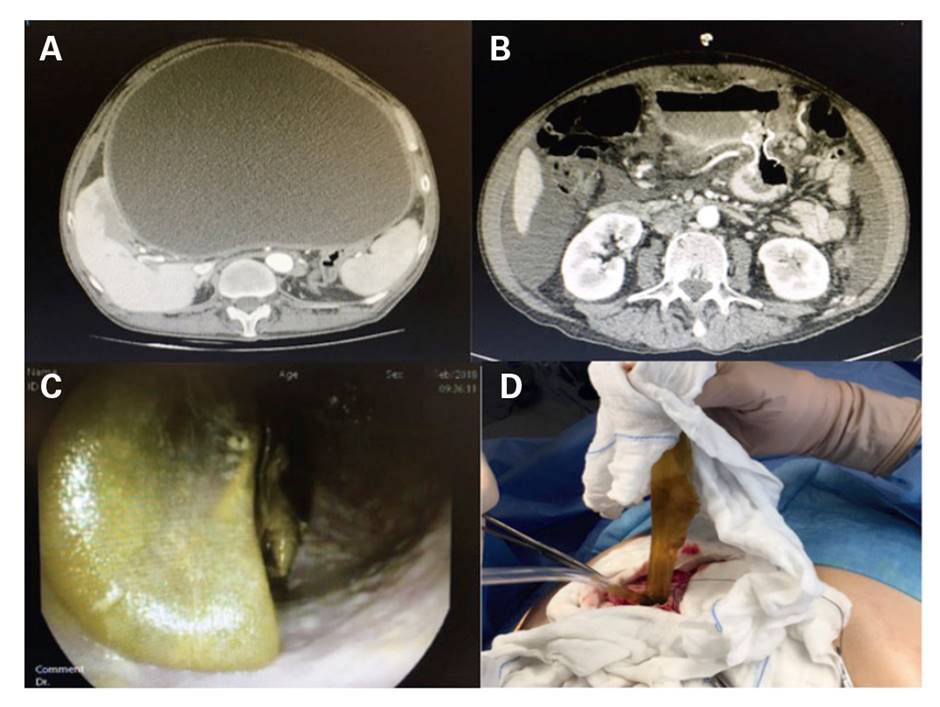
Fig. 1 A. Abdominal collection. B. After drainage via LAMS. C. Interior of the cystic cavity. D. Extraction of the germinal membrane.
We assume that the LAMS instantly sealed the gastro-cystic fistula and avoided any anaphylactic adverse event. Even though surgery is the treatment of choice 2, this approach (even though initially unintended) may open a new window to patients with a massive cyst or those unsuitable for surgery.
Bibliografía
1. Kawakami H, Itoi T, Sakamoto N. Endoscopic ultrasound-guided drainage for peripancreatic fluid collections: where are we now? Gut Liver 2014;8(4):341-55. DOI: 10.5009/gnl.2014.8.4.341 [ Links ]
2. Jaiswal P, Jaiswal R, Attar BM, et al. Hepatobiliary and pancreatic: massive hepatic cystic echinococcosis compressing inferior vena cava. J Gastroenterol Hepatol 2018;33(2):339. DOI: 10.1111/jgh.14038 [ Links ]
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
