










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Cirugía Oral y Maxilofacial
On-line version ISSN 2173-9161Print version ISSN 1130-0558
Rev Esp Cirug Oral y Maxilofac vol.27 n.3 Madrid May./Jun. 2005
Artículo Clínico
A clinical and radiographic evaluation of the distraction osteogenesis technique for the reconstruction of atrophic alveolar ridges in the anterior region of the upper maxilla
Evaluación clínica y radiográfica de la técnica de distracción osteogénica en la reconstrucción
de rebordes alveolares atróficos en la región anterior del maxilar superior
M.E. Allais de Maurette, DDS, MSc,1 P.E. Maurette OBrien, DDS, MSc,1 R. Mazzonetto, Msc, PhD2
|
Abstract: This study evaluates clinically and radiographically the distraction osteogenesis technique for the reconstruction of atrophic alveolar ridges in the anterior maxilla region, and the possible complications that arise during treatment. Fifteen patients were evaluated, clinically and radiographically, that had been treated with alveolar distraction osteogenesis in the anterior region, using a juxta-osseous distractor. In 13 patients (86.6%) the technique was completely successful, there being an effective bone gain of 7,04 mm. In 1 patient (6.66%) this was partial (2.62 mm) and in 1 patient (6.66%) the technique failed, as there was a gain of just 0,76 mm because of problems during the activation. The complications arising during the alveolar distraction osteogenesis were divided into minor complications that did not compromise the success of the technique, and which were found in 8 patients (53.33%), and major complications that did not permit rehabilitation, which were found in 1 patient (6.66%). The alveolar distraction osteogenesis technique proved to be an effective technique for the reconstruction of atrophic alveolar ridges with a success rate of 93.33%. There were minor complications but the surgeon intervened in time and these were solved. Key words: Alveolar distraction osteogenesis, Osseointegrated implants. |
Resumen: Este estudio tiene como objetivo evaluar clínica y radiográficamente la técnica de distracción osteogénica alveolar en la región anterior del maxilar superior y las posibles complicaciones que pueden aparecer durante el tratamiento. Fueron evaluados 15 pacientes, sometidos a reconstrucción alveolar del maxilar superior en la región anterior con distracción osteogénica, usando un distractor yuxtaóseo. Del total de 15 pacientes encontramos que 13 pacientes (86,6%) obtuvieron un éxito total de la técnica, obteniendo una ganancia ósea real media de 7,04 mm; en 1 paciente (6,66%) fue parcial (2,62 mm) y en 1 paciente (6,66%) se evidenció un fracaso en la técnica, al alcanzar solo 0,76 mm debido a problemas en la activación del distractor. En cuanto a las complicaciones surgidas durante el tratamiento fueron divididas en complicaciones menores, toda aquella que no interfirió en el éxito del tratamiento, y que estuvieron presentes en 8 pacientes (53,33%), y complicaciones mayores aquellas que no permitieron la rehabilitación con implantes, y que fue encontrado solo en 1 paciente (6,66%). La técnica de distracción osteogénica alveolar, demostró ser eficaz en la reconstrucción de rebordes alveolares atróficos con un éxito de 93,33%, presentado pequeñas complicaciones que pueden ser solventadas por medio de un seguimiento por parte del profesional. Palabras clave: Distracción ósea alveolar; Implantes Oseointegrados. |
Recibido: 24 de agosto 2004
Aceptado: 28 de marzo 2005
1 Odontólogo USM. Caracas -Venezuela. MSc en Cirugía y
Traumatología Buco- Maxilofacial de la
Facultad de Odontología de Piracicaba. Universidad Estadual de Campinas
(FOP-Unicamp).
Piracicaba-SP-Brasil. Residente del Doctorado en Cirugía y Traumatología
Buco-Maxilofacial de la
Facultad de Odontología de Pernambuco. Universidad de Pernambuco (FOP-UPE).
Recife-PE-Brasil.
2 Odontólogo, Cirujano Buco-Maxilofacial. Profesor Asociado.
Área de Cirugía y Traumatología Buco-Maxilofacial y
Director del Curso de Especialización en Implantología de la Facultad de
Odontología de Piracicaba.
Universidad Estadual de Campinas (FOP-Unicamp). Piracicaba-SP-Brasil.
Correspondencia:
Dra. Marvis Allais de Maurette
Rua Luis de Farias Barboza. N 271. ap 50
Boa Viagem- Recife. Pernambuco-Brasil
CEP: 51020110
Email: marvisallais@cirugia-maxilofacial.net
Introduction
As a result of developments in the area of implantology, the proper establishment of recipient beds became a fundamental requirement for the success of treatment with osseointegrated implants. The amount and quality of the alveolar ridge directly influences biomechanical and aesthetic results as well as the stability of the implantsupported prosthesis and the health of adjacent teeth.
Over the last years bone grafts,1,2 biomaterials,3,4 and guided bone regeneration,5,6 have been used for achieving alveolar ridge augmentation. Distraction osteogenesis is a technique allowing gradual bone growth that makes the formation of new bone possible in a fast and predictable way by means of natural bone regeneration mechanisms, thus preparing the bed suitably before the placement of osteointegrated implants.
This technique has some advantages when compared with autogenous grafts such as: a second surgical site is not required for obtaining a graft, bone growth is not limited, there is a simultaneous expansion of soft tissues, blood vessels and nerves during the complete bone growth process,9- 18 there is less likelihood of resorption, a lower rate of morbidity and infection, and in addition the time required for placing the implants (10 weeks after distraction) is reduced.
The purpose of this study was to evaluate clinically and radiographically the technique for alveolar distraction osteogenesis in the anterior portion of the upper maxilla, in 15 patients operated on by the Faculty of Dentistry of Piracicaba- Unicamp between January 2003 and July 2004.
Material and Method
The medical histories of 15 patients that had undergone reconstructive surgery of the anterior portion of the upper alveolar ridge by means of distraction osteogenesis were chosen. A panoramic radiograph was taken of each of the patients seven days into the postoperative period before the activation of the device and another 90 days later, before removal of the device in order to evaluate how effective the vertical bone gain had been. In order to obtain these values it was necessary to identify the real bone gain by means of the following protocol:
A. Definition of the Amplification Factor (AF): the real size of the activation rod (RS) was measured in the device itself (Fig. 1) and the image size of the activation rod (IS) in the panoramic radiograph itself (Fig. 2). The AF is obtained using the following formula: AF = IS/RS. This variable was determined with each of the panoramic radiographs, during the pre-activation stage as well as on completion.
B. Definition of the Real Bone Gain (RBG): Initially this was the radiographical distraction amount (RDA1) pre-distraction that was taken from the radiographs a week later by measuring the distance between the upper portion of the activation rod (a) to the upper portion of the transport rod (Fig. 3) (b) multiplied by the AF obtained in each of the radiographs.
The radiographical distraction amount post-activation (RDA2) was immediately obtained using the same technique with radiographs taken at 90 days (Fig. 4).
The definition of RBG was obtained by the following formula RBG = RDA2-RDA1.
A weekly following of the patients was carried out in order to detect rapidly any complications arising during this period. The complications were divided according to the extent of the repercussions to the technique. Those not adversely affecting the result of the technique, such as edema, dehiscence, infection and lingual displacement of the transport disk were classified as minor problems, and those such as fracture of the transport disk or an inadequate height of the device were classified as major problems.
Results
Radiographic evaluation was carried out in 15 patients that underwent reconstructive surgery of the anterior portion of the upper alveolar ridge by means of alveolar distraction osteogenesis with 9 mm juxta-osseous osteogenic distractors.
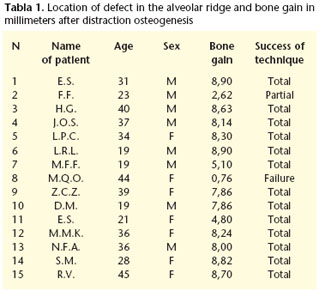
The results included: 8 male patients, 7 female patients with a mean age of 31. In 13 patients (86%) the technique was completely successful, with a average real bone gain of 7.73 mm; in 1 patient (6.66%) this was partial (2.62 mm) as the patient had problems in activating the device and the maximum opening was not achieved, but there was enough bone height for implant rehabilitation on removing the distractor, and lastly the technique failed with 1 patient (6.66%) as only 0.76 mm was reached due to problems in activating the device (Table 1).
With regard to complications we found that 9 patients (60%) presented some type of complication. In 8 (88.88%) the complication was minor, there being mainly dehiscence and infection in 4 patients (35.71%) and in 1 patient (6.66%) there was a major complication due to the device blocking (Figure 5).
Discussion
Using the distraction osteogenesis technique for the reconstruction of atrophic alveolar ridges proved to be an effective method that provided an increase in alveolar bone height together with expansion of the adjacent soft tissue (93.33%). When distraction osteogenesis is compared with other surgical techniques such as bone grafts or guided bone regeneration, dealing with soft tissue becomes difficult when a large amount of bone is required, as this normally leads to dehiscence of the wound.
It is important to stress the predictability of this bone gain, and this should be noted as another of the great advantages of this technique. Lazar et al. (1999)14 observed a low bone resorption rate due mainly to the periosteum of the osteotomized segment receiving nourishment.
As a result of the shorter treatment time required for distraction osteogenesis, the placement of osteointegrated implants can be brought forward, and these can be placed 10 weeks after the initial surgery.
It should be stressed that in spite of these advantages, there are some cases where this technique is contraindicated, mainly when the area of remaining bone is insufficient for carrying out distraction, and when there is a high risk of harming the bone base and the transport disk, with a fracture occurring on activating the distractor. For this not to occur, the alveolar ridge that is to be distracted should have a minimum height of 7 to 8 mm. (Maurette et al 2004).15
Some complications associated with distraction osteogenesis can occur when the recommended surgical protocol is not carried out, or when patient collaboration or the follow- up by the surgeon is not correct. Among the more common complications we find: edema, dehiscence, infection, lingual displacement of the transport disk that are complications not directly affecting the success of the technique. We can also find major complications that affect treatment such as the fracture of the distraction rod or of the transport disk. (Mazzonetto y Torrezan, 2003).16
The patient needs to be instructed and accompanied by the professional during the complete activation period. In the event of any complications, these can be evaluated and treated immediately so that the success of the technique is not affected.
Conclusions
We can affirm that this technique provides a reliable and predictable method for reconstructing atrophic alveolar ridges and that, as a result, bone augmentation is adequate, and treatment time is shorter while complication rates are low.
In the aesthetic areas of the upper maxilla there is a greater need for associating techniques in order to gain greater width. There are strong indications for associating distraction osteogenesis techniques with block grafts, as with distraction we only resolve in a foreseeable way, large vertical ridge deficiencies. In some cases thickness augmentation is necessary, and this is when the autogenous graft becomes the ideal treatment. In addition, this soft tissue augmentation generated by the distraction has proved to be one the great aesthetic advantages of the technique, also contributing to better tissue covering in autogenous graft cases.
Aknowledgments
We would like to thank the Foreign Affairs Ministry of Brazil and the «Coordinación de Perfeccionamiento del Nivel Superior» (CAPES) for the study grants during the magister, as part of the program «Estudiante Convenio de Postgrado» (PEC-PG), which enabled carrying out this investigation work.
References
1. Artzi Z, Nemcovsky CE. The application of deproteinized bovine bone mineral for ride preservation prior to implantation: Clinical and histological observations in a case report. J Periodontol 1998;69:1062-7. [ Links ]
2. Betts NJ, Vanarsdall RL, Barber HD, Hibbins-Barber K, Fonseca RJ. Diagnosis and treatment of transverse maxillary deficiency. Int J Adult Orthod Orthognath Surg 1995;10:75-96. [ Links ]
3. Block MS, Chang A, Crawford C. Mandibular alveolar ride augmentation in the dog using distraction osteogenesis. J Oral Maxillofac Surg 1996;54:309-14. [ Links ]
4. Carls FR, Sailer HF. Seven years clinical experience with mandibular distraction in children. J Craniomaxillofac Surg 1998;26:197-208. [ Links ]
5. Chin M, Toth B. Distraction osteogenesis in maxillofacial surgery using internal devices: Review of five cases. J Oral Maxillofac Surg 1996;54:45-53. [ Links ]
6. Chin M, Distraction osteogenesis for dental implants. Atlas Oral Maxillofac Surg Clin North Am 1999;7:41-63. [ Links ]
7. Gaggl A, Schultes G, Karcher H. Vertical alveolar ridge distraction with prosthetic treatable distractor: A clinical investigation. Int J Oral Maxillofac Implants 2000;15:701-10. [ Links ]
8. Guerrero CA, Bell WH, Contasti GI, Rodriguez AM. Mandibular Widening by Intraoral distraction osteogenesis. Br J Oral Maxillofac Surg 1997;35:383-92. [ Links ]
9. Horiuchi K, Uchida H, Yamamoto K, Hatano N. Anteroinferior distraction of the atrophic subtotal maxillary alveolus for implant placement: A Case Report. Int J Oral Maxillofac Implants 2002;17:416-23. [ Links ]
10. Ilizarov GA. The principles of the Ilizarov method. Bull Hosp Jt Dis Orthop Inst 1988;48:1-11. [ Links ]
11. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues. Part 1: The influence of stability fixation and soft tissue preservation. Clin Orthop Rel Res 1989:249-81. [ Links ]
12. Ilizarov GA. The tension-stress effect on the genesis and growth of tissues. Part 2: The influence of the rate and frequency of distraction. Clin Orthop Rel Res 1989:263-85. [ Links ]
13. Klen C, Papageorge M, Kovacs A, Carchidi JE. Initial experiences with a new distraction implant system for alveolar ridge augmentation. Mund Kiefer Gesichtschir 1999;3:S74-S78. [ Links ]
14. Lazar F, y cols. Knocherne Regeneration Des Unterrieferalveolarfortsatzes Mit Hilfe Der Vertiralen Rallusdistrartion. Dtsch Zahnarzil Z, v. 54, p. 51-54, 1999. [ Links ]
15. Maurette PE, Allais de Maurette M, Mazzonetto R. Distracción ostetogénica alveolar: una alternativa en la reconstrucción de rebordes alveolares atróficos. Descripción de 10 casos. Rev Esp Cir Oral Maxilofac 2004;26:41-7. [ Links ]
16. Mazzonetto R, Torezan JF. Potencial complications during alveolar distraction osteogenesis. J Oral Maxillofac Surg, Philadelphia, v.61, n.8, p.85. 2003. [ Links ]
17. Polly JW, Figueroa AA. Management of severe maxillary deficiency in childhood and adolescence through distraction osteogenesis with an external, adjustable, rigid distraction device. J Craniofac Surg 1997;8:181-6. [ Links ]
18. Rachmiel A, Srouji S, Peled M. Alveolar ridge augmentation by distraction osteogenesis. Int J Oral Maxillofac Surg 2001;30:510-7. [ Links ]
19. Tavaloki K, Stewart KJ, Michael DP. Distraction osteogenesis in craniofacial surgery: A review. Ann Plast Surg 1998;40:88-99. [ Links ]

