










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Orbital fractures are frequently associated with complications, such as persistent diplopia, enophthalmos and decreased globe motility1. There is evidence that exact bony reconstruction and repositioning of orbital soft tissues will correct, or at least considerably improve clinical symptoms2. Nevertheless, restoration of normal orbital volume and globe position following traumatic injury is often difficult. In orbital fracture surgery the visibility is often reduced, and the surgical field is small. Due to this, verifying proper implant position during the operation is often hard. Intraoperative navigation has emerged as a tool to allow the visualization of the implant position intraoperatively, by means of the planification in the preoperative CT scan1,2,3,4. Navigation-assisted orbital reconstruction was introduced by Gellrich et al. in 20025, and in recent years, many studies have demonstrated the feasibility of this technique6,7.
The aim of this study was to compare the postoperative changes in orbital volume between two groups of study: one group that underwent surgical intervention before the implementation of intraoperative navigation (control group), and other group of patients which had undergone surgery with the aid of a navigation system (navigation group). Another endpoint of our study was to determine if the presurgical planification and intraoperative navigation aided to position the implant. For that purpose, we determined the implant position with respect to the orbital floor and medial orbital wall and compared it between both groups of study. As secondary endpoints, we compared the rate of postoperative outcomes and reintervention rate between both groups.
MATERIALS AND METHODS
A retrospective cohort study was designed. We selected a total of 35 consecutive orbital operations for unilateral orbital fractures performed between 2015 and 2018 at the Department of Oral and Maxillofacial Surgery in La Paz Hospital (Madrid), Spain. The inclusion criteria were: 1) adult patients with unilateral orbital fracture involving the orbital floor and/or the medial wall with defect size larger than 2 cm2, extending into the posterior third of the orbit; 2) associated diplopia, or ocular motility impairment, or abnormal globe position (enophthalmos clinically evident [>2 mm] by estimating the projection of the eyes by viewing from above and below)8; 3) preoperative and postoperative CT scan with 0.625- to 1.0- mm slice thickness; 4) preoperative and postoperative surgical records; 5) minimum of 6 months follow-up. Patients who did not fulfilled these criteria were excluded.
We collected information regarding: demographic data, cause of the fracture, time elapsed between diagnosis and surgical treatment, symptoms at diagnosis (diplopia, globe position, ocular motility impairment), radiological findings (affected wall, muscular entrapment, herniation of the periorbital structures), and outcomes after surgical treatment (diplopia, globe position, ocular motility impairment, reintervention).
We divided the sample into two groups:
The navigation group (with the aid of presurgical planification and intraoperative navigation) consisted of a consecutive cohort of 18 patients that fulfilled the inclusion criteria. These patients underwent surgery between 2016-2018, after the implementation of the navigation system. In this group of patients, the postoperative CT scans were done 24 h after the surgery.
The control group (without the aid of presurgical planification and intraoperative navigation) consisted of a consecutive cohort of 17 that fulfilled the inclusion criteria. These patients underwent surgery prior to the implementation of the navigation system in our department (2015-2016). In this group of patients, the postoperative CT scans were done one week after the surgery.
Surgical technique
All patients were operated on under general anaesthesia. Preoperative antibiotic prophylaxis (2 g amoxicillin with clavulanic acid) was given perioperatively (2 g) and postoperatively (1 g/8 h) for 7 days. A transconjunctival incision was used in all cases. The bony perimeter of the fracture was isolated.
In the control group, a pre-bent titanium orbital mesh was used (Synthes). The mesh was placed freehand under direct vision and fixed with two monocortical screws to the inferior orbital rim. Forced duction testing was performed to confirm normal ocular mobility in all patients. The conjunctiva was closed with resorbable 5/0 uninterrupted suture.
In the navigation group, a navigation system Software iPlan CMF (version 3.0.5, Brainlab (r), Feldkirchen, Germany) was used for presurgical planning and intraoperative control of orbital contours and mesh positioning. The preoperative CT scan was loaded into the navigation computer. Mirroring of the unaffected orbit into the fractured side was created. This template was used for navigation during surgery, and navigation was used to verify both the posterior ledges of the fracture and the position and shape of the implant. A pre-bent titanium orbital mesh was used (Synthes). Additionally, to make sure a correct plate positioning during surgery, we carried out the printing of a stereolitographic model through our 3D printer (UP studio) (Figure 1) and we adapted the pre-bent titanium orbital mesh presurgically. The stereolitographic model impression was carried out only in the navigation group (Figure 2).


Measurement of the orbital volume
By means of the iPlan CMF software, the orbital volume of the affected, unaffected and reconstructed side was determined with the smart brush tool, by means of which the limits of the orbit were determined manually (including the herniated soft tissue in the affected side) and were corrected by coronal and axial position (Figure 3 and Figure 4). Volume measurements were reported in cubic centimetres.
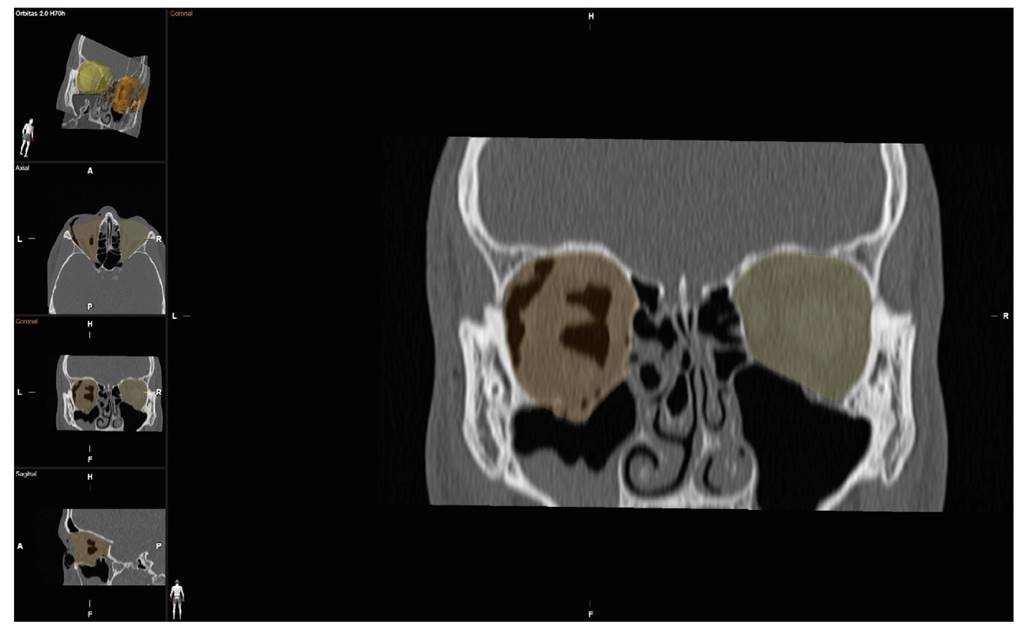
Figure 3. Measurement of the orbital volume of the affected side with the smart brush tool, including the herniated soft tissue in the affected side.

Measurement of implant positioning
By using the image fusion tool of the iPlan CMF software, the preoperative and postoperative CT scans were overlapped automatically. The plate position was determined by measuring three points:

Figure 5. Distance between the plate and the orbital rim. Only the sagital plane was used for measurement.

Figure 6. Distance between the plate and the residual posterior intact bony ledge. Only the sagital plane was used for measurement.
By using the iPlan CMF software, measurements are performed automatically in the three planes of space, although we used the sagital plane to measure the distance between the plate and the orbital rim and between the plate and the residual posterior intact bony ledge. To measure the distance between the plate and the medial orbital wall we used the axial plane. Distance was measured in milimeters.
RESULTS
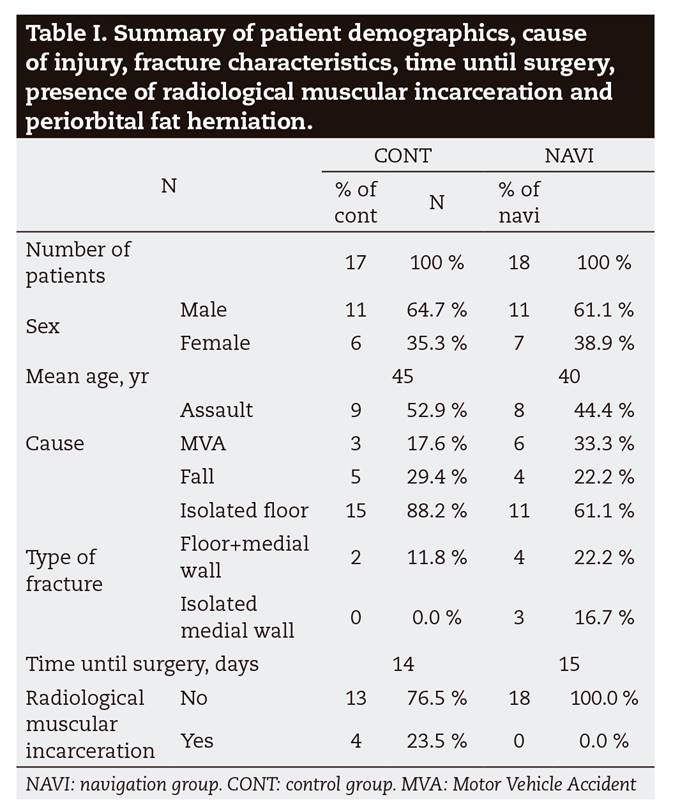
35 orbital operations performed in the department of Oral and Maxillofacial surgery in La Paz Hospital between 2015 and 2018 were selected. Clinical and demographic characteristics of the sample are summarized in Table 1. 18 cases were performed between January 2016 and December 2018, using the navigation system (navigation group) and 17 cases were performed before January 2016 without it (control group). The time elapsed between the diagnosis and the surgery was 14 days in the control group and 15 days in the navigation group. The average age was 45 years old in the control group and 40 years old in the navigation group. Patient demographics, cause of injury, fracture characteristics, reintervention and CT scan characteristics are summarized in Table 1.
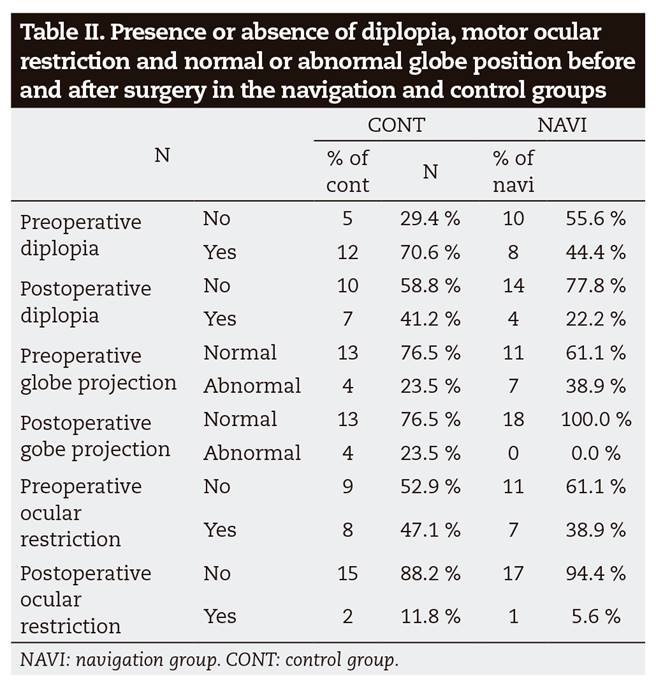
In the control group, of the 12 patients with diplopia at diagnosis, 7 patients recovered and 5 persisted with diplopia in the postoperative period. 2 patients in the control group developed diplopia in the postoperative period. In the navigation group, of the 8 patients with diplopia at diagnosis, 5 patients recovered and 3 persisted with diplopia in the postoperative period. 1 patient in the navigation group developed diplopia in the postoperative period. In the control group, of the 4 patients with abnormal globe position at diagnosis, 1 patient recovered and 3 persisted with abnormal globe position in the postoperative period. 1 patient in the control group developed abnormal globe position in the postoperative period. In the navigation group, all the 7 patients with abnormal globe position recovered. In the control group, of the 8 patients with ocular motility impairment at diagnosis, 7 patients recovered and 1 persisted with ocular motility impairment in the postoperative period. 1 patient in the control group developed ocular motility impairment in the postoperative period. In the navigation group, of the 7 patients with ocular motility impairment at diagnosis, 6 patients recovered and 1 persisted with ocular motility impairment in the postoperative period (Table 2). Both groups were homogeneous (p > 0.05) in terms of ocular motility impairment, diplopia, and globe position outcomes before surgery. After surgery, we observed that abnormal globe position was significatively less frequent in the navigation group than in the control group (p = 0.029), as no patients persisted with abnormal globe position after surgery in the navigation group (Table 3).

In the control group, 6 patients required reintervention, and in the navigation group only 2 patients required reintervention (Table 3). The reoperation rate was 11% in the navigation group and 35% in the control group (p = 0.071). Of the 6 patients requiring a secondary operation in the control group, 4 were due to persistence of diplopia and abnormal globe projection and 2 were due to persistence of diplopia. Of the 2 patients requiring secondary operation in the navigation group, one was due to persistence of diplopia and the other one required a blepharoplasty due to postoperative palpebral retraction.
When we analysed the measurements of the orbital volume of the whole sample, we saw that the mean orbital volume of the affected side was significatively bigger that the mean volume of the reconstructed side (mean volume reduction 4,32 cm3, p < 0.00001), and that the mean orbital volume of the reconstructed side did not differ significatively from the mean orbital volume of the unaffected side (difference in volume between unaffected side and reconstructed side -0.19 cm3, p = 0.57). Nevertheless, when we compared both groups separately, the mean volume reduction and the mean difference in volume between unaffected and reconstructed side did not show significative differences. Mean orbital volume of the unaffected orbit was 29.32 ± 2.64 cm3 in the navigation group and 28.64 ± 2.68 cm3 in the control group. Mean orbital volume of the affected orbit was 34.19 ± 3.67 cm3 in the navigation group and 32.78 ± 3.09 cm3 in the control group. The mean reconstructed orbital volume was 29,47 ± 2,75 cm3 in the navigation group and 28.88 ± 3.72 cm3 in the control group (Table 4).
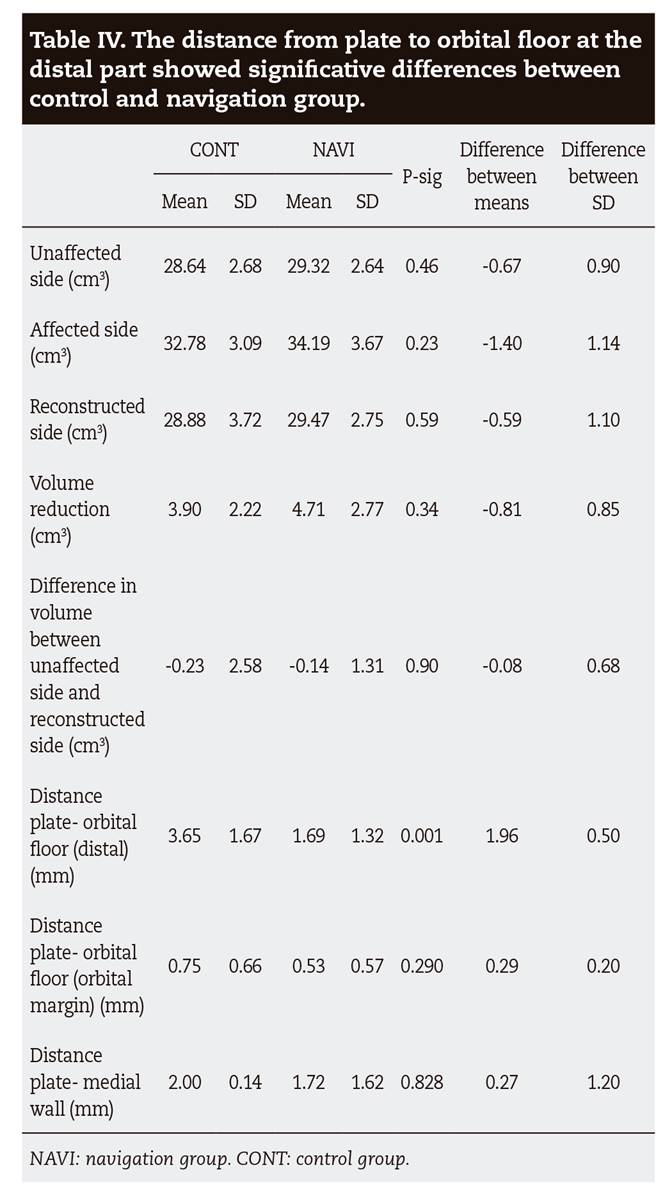
The mean distance from plate to orbital floor at the distal part was 3.65 ± 1.67 cm3 in the control group and 1.69 ± 1.32 cm3 in the navigation group. The mean distance from plate to the orbital floor at the orbital margin was 0.755 ± 0.66 cm3 in the control group and 0.53 ± 0.57 cm3 in the navigation group. The distance from plate to the medial orbital wall was 2 ± 0.14 cm3 in the control group and 1.7 ± 1.62 cm3 in the navigation group. The distance from plate to orbital floor at the residual posterior intact bony ledge showed significative differences (p = 0.001) (Table 4).
DISCUSSION
This retrospective study demonstrated a better control of the positioning of the plate at the residual posterior intact bony ledge of the floor of the orbit in the navigation group compared with the control group. These differences were statistically significative (p = 0.001). The clinical evaluation showed that there was a statistically significant increase in globe projection between the preoperative and postoperative periods in the navigation group compared with the control group (p = 0.039). Furthermore, a greater volume reduction in the navigation group (4.71 cm3) compared with the control group (3.90 cm3) was achieved, although this difference was not statistically significative (p = 0.34). The need for secondary operation was lower in the navigation group compared with the control group, as only one patient required reexploration for implant repositioning in this group. The reoperation rate was 11% in the navigation group and 35% in the control group (p = 0.71). This was not statistically significant, partly because of the small sample size.
Novelli et al.9 reported a correspondence between the post-operative reconstruction mesh position and the presurgical virtual planning with a margin of error of less than 1.3 mm. In a cadaveric study of Jansen et al10 implant position improved significantly for translation (2.6 mm), yaw and roll in the group with preoperative planning. Zimmerer et al.(11 showed that with intraoperative navigation, the precision of orbital volume reconstruction increased significantly. We achieved an improvement in plate positioning in the navigation group, and this improvement was more evident at the the residual posterior intact bony ledge of the floor of the orbit, where an average error of 1.69 mm was found in contrast to the 3.65 mm observed in the control group (p = 0.001). In our study, stereolitographic models and patient specific implants bended presurgically were used in the navigation group. An overlap in the use of individualized implants and navigation may make it difficult to attribute the improved precision to a single factor, although some studies found no significative differences between the use of patient-specific implants molded from the preinjury STL model, titanium mesh sheets bent freehand, and preformed titanium meshes12.
Reconstruction of the orbital floor posterior to the eyeball equator is the most important aspect for correcting enophthalmos13,14,15. As mentioned above, we have demonstrated a better control of plate positioning in the posterior orbital floor with navigation-aided surgery, and this could explain our better results in terms of orbital globe projection in the navigation group compared to the control group (p = 0.039). We assessed orbital globe projection clinically, by estimating the projection of the eyes by viewing from above and below, as performed in other studies8, and we considered an abnormal globe projection to the enophthalmos perceived clinically (> 2 mm).
According to the literature, there are different methods for the measurement of orbital volumes16,17. The major difficulty in comparing data is the definition of the anterior border of the bony orbit and the delimitation of the herniated periorbital tissue into the maxillary or ethmoidal sinuses18,19,20. We observed that the brainlab software by itself could not only calculate properly the contour of the herniated soft tissue, but also it was hard to delineate the anterior bony orbit manually without having a reference. To avoid this potential bias, we performed the measurement of the contour of the bony orbit manually (by using the smart brush tool). Doing the measurements this way we could delineate the limits of the herniated soft tissue avoiding the error produced if we did it automatically. Some studies have reported that navigation aided surgery significantly improves the restoration of the orbital volume, and that specifically the use of a navigation system leads to a greater volume reduction than in the conventional surgery. In our study, we observed that both groups were similar in terms of mean orbital volume of the unaffected and affected sides, and that with both methods a similar volume of the reconstructed side was achieved (Table 4). By comparing the difference in volume between unaffected and reconstructed side we can observe that both groups achieved an adequate orbital volume in the reconstructed side (control group -0.23 cm3; navigation group -0.14 cm3) (Table 4). We observed a greater volume reduction in the navigation group (4.71 cm3) compared with the control group (3.90 cm3), but nevertheless these differences were not statistically significative (p = 0.34) (Table 4). Maybe, one of the reasons for obtaining this result was the different protocol for performing the postoperative CT scan in both groups, as in the control group the postoperative CT scan was made one month postoperatively, and in the navigation group it was made the day after the surgery.
There is a paucity of literature comparing the computer-aided techniques with conventional techniques with which to analyse outcomes. Zavattero et al.2 reported a lower rate of severe postoperative diplopia in the navigation group. Their orbital volume analysis showed that reconstructed orbital volume in the navigation group was closer to unaffected orbital volume compared with the control group. Markiewicz et al.3 reported a retrospective cohort study of 23 subjects that assessed the reliability and effectiveness of intraoperative navigation in restoring normal orbital volume in traumatic and postablative defects. Their sample was composed by patients with complex orbital fractures affecting several walls and associated to other facial fractures, and by some patients with orbital tumours. The results of their study validate that intraoperative navigation is not only effective in restoring orbital and globe dimensions in post-traumatic defects, but also in post-ablative defects. Randall et al.6) also observed a reduced postoperative diplopia in the navigation group. and the effectiveness was maximal for fractures that involved 3 or 4 walls or the posterior one-third of the orbital floor. The need for revision surgery was also reduced in this cohort. Essig et al.7 found that the orbital volume of the affected side was significantly bigger in orbital fractures with involvement of the posterior third of the orbital floor and in comminute fractures. They observed a significant reduction of orbital volume in the navigation group and non-significant reduction in conventional group.
Our study has some limitations, as we did not construct a multivariate model for analysis. Therefore, potential confounders that could modify treatment outcomes were not identified. Also, enophthalmos was addressed only clinically. Some differences existed between both groups, as all the surgeries were not performed by the same surgeon, and due to the different times when the surgery was performed: first, stereolitographic models and patient specific implants bended presurgically were used in the navigation group, and not in the control group; and second, the postoperative CT scan was not made at the same moment in both groups, which was probably the reason for not obtaining differences between the navigation group and the control group in terms of orbital volume reduction.
CONCLUSIONS
The results of this study suggest that using intraoperative navigation in orbital fractures is effective in improving plate positioning in the residual posterior intact bony ledge of the floor of the orbit, reducing complications such as enophthalmos compared to conventional surgery. Furthermore, the use of intraoperative navigation seems to decrease the rate of reintervention compared to conventional surgery. In our study, the restoration of orbital volume seems to be well addressed by both methods, as by comparing the difference in volume between unaffected and reconstructed side, both groups achieved an adequate orbital volume in the reconstructed side.

