










 Custom services
Custom services
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Diabetic macular oedema (DME) is the leading cause of vision loss in diabetic retinopathy and, consequently, of blindness in patients with diabetes mellitus1. As such, it has a strong negative impact on patients.
This inflammatory disorder is a consequence of metabolic changes secondary to hyperglycaemia caused by diabetic retinopathy in the macula. Vasogenic changes that induce rupture of the blood-retinal barrier together with inflammatory activation lead to severe retinal damage and chronic macular changes2.
The clinical objectives of the treatment of DME are to reduce the severity of oedema and prevent loss of vision3. Treatment is based on effective metabolic control (glycaemia, hypertension, lipid profile, renal function), but requires further measures to prevent vision loss, such as laser photocoagulation and drug treatments4. Approved treatments for DME include two groups of medications which are delivered by intravitreal injection: vascular endothelial growth factor inhibitors (anti-VEGF), such as ranibizumab and aflibercept, and corticosteroids, such as dexamethasone in a sterile sustained-release implant. Posology is variable because the response to treatment over time determines the frequency of injections. Several clinical trials have found that these therapies are effective5 6-7. They are indicated for patients with DME, regardless of the recommendations or protocols that establish specific treatment algorithms.
Blindness, diabetic retinopathy, and DME are very frequent in diabetic patients. Blindness, diabetic retinopathy, and DME have prevalences of between 4% and 11%, of 40%, and between 1.4% and 7.9%, respectively8. DME and loss of visual acuity negatively affect patients’ health-related quality of life and affects their ability to perform everyday tasks, including the self-management of diabetes9,10.
DME and diabetic retinopathy have a high economic impact because of their direct costs as well as their indirect costs, such as reduced income or an increased need for social support as vision worsens11. It has been estimated that the annual resource utilisation and direct health cost per patient with DME are approximately double those of patients without DME12. Bilateral DME is associated with higher direct health costs and with higher indirect costs caused by its impact on working life13.
The aim of this study was to determine the budget impact on the Spanish National Health System of the inclusion of dexamethasone intravitreal implant (IVI) in the treatment of DME in a specific healthcare region in Spain.
Methods
The budget impact analysis was developed based on national and international recommendations14,15. The analysis was conducted using Microsoft Excel. An expert panel comprising three vitreoretinal specialists was consulted to validate the values of the parameters obtained from the literature and to reach a consensus on resource utilisation in standard clinical practice. This study assessed the incremental budget impact of the inclusion of dexamethasone IVI as a new therapeutic alternative for DME.
Therapeutic alternatives and scenarios
The analysis considered the therapeutic options currently funded by the Spanish National Health System with approved indication and currently in use for the treatment of DME: aflibercept 40 mg/mL injectable solution; ranibizumab 10 mg/mL injectable solution; and 700 μg dexamethasone IVI in applicator. Two different scenarios were compared: in scenario 1 dexamethasone IVI is not available; in scenario 2 dexamethasone IVI is included in the therapeutic armamentarium for DME. For each scenario, the costs associated with the management of DME were calculated for each of the treatment options. The costs of each of the selected drugs were weighted according to the percentage of usage to obtain the total costs of each scenario. The budget impact of introducing the new treatment was calculated by comparing the total costs generated in each scenario (without dexamethasone IVI vs with dexamethasone IVI).Table 1shows the percentage of usage of each drug in each scenario (internal estimate (base case) and the expert panel estimate (alternative analysis)).
Table 1. Number of injections per year, percentage of usage, and unitary price of the therapies
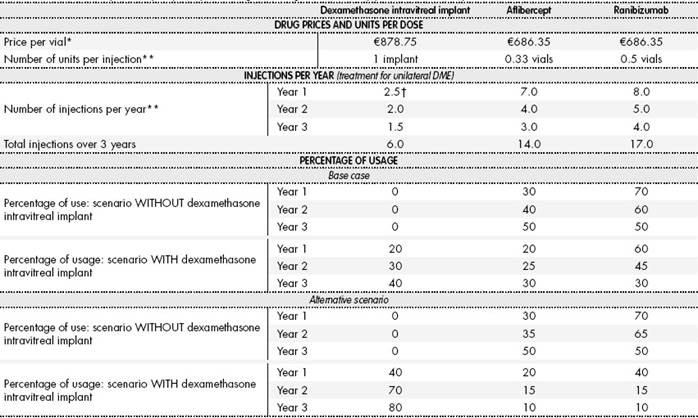
DME: diabetic macular oedema. *Exfactory prices with deduction established by Royal Decree-Law 8/2010. **Determined by an expert panel according to standard clinical practice. † Standard clinical practice establishes a 5-month interval for treatment-naive patients (2-3 injections/year).
Target population
The target population considered for treatment comprised diabetic patients with macular oedema undergoing treatment with intravitreal ophthalmologic therapies. Epidemiological data were used to calculate the target population in an area with a population of 25,000 adults. We considered the prevalence of diagnosed diabetes mellitus (7.8%)16and of DME (5.73% in type 1 diabetes and 6.44% in type 2 diabetes)17, as well as the incidence of DME (6.36% during 8-year follow-up in diabetic patients)18over the total study period. The percentages of patients diagnosed with DME receiving treatment (80%) and patients with bilateral DME (60%) were determined by the expert panel according to standard clinical practice.
Perspective, time horizon, and discount rate
Direct health costs alone were considered because the analysis was conducted from the perspective of the Spanish National Health System. No discount rate was applied because interannual costs were not compared. The time horizon used was 3 years.
Resources and costs
Given the chosen perspective, the following costs were considered: drug costs, administration costs, monitoring/follow-up costs (including tests and follow-up visits), and the costs of managing adverse events. Resource costs were based on the estimated utilisation of each resource and their unitary costs
Drug costs were estimated using the exfactory price (EFP), which corresponds to the official price19. The deductions established by Royal Decree-Law 8/2010 were applied to the EFP. The estimated drug costs of each therapy were based on the number of injections required per year and the number of vials of each drug used per injection. In line with standard clinical practice, it was assumed that the contents of the vials would be divided (aflibercept divided into 3 intravitreal injections, and ranibizumab divided into 2 intravitreal injections). We excluded the additional cost of the division process to the pharmacy services. The estimated drug administration costs of each drug were based on the number of annual intravitreal injections needed for each therapeutic alternative and on whether DME was unilateral or bilateral as determined by the expert panel (Table 1).
Follow-up costs were estimated according to the total number of follow-up visits required (with or without delivery of an intravitreal injection) and the diagnostic tests performed during these visits. Tests performed during the follow-up visits included optical coherence tomography, ophthalmoscopy, tonometry, visual acuity testing and, in some cases, fluorescein angiography. It was assumed that 100% of patients receiving treatment with dexamethasone for bilateral DME would require two visits to treat both eyes, whereas only 80% of patients receiving treatment with aflibercept or ranibizumab would require two visits for the treatment of bilateral DME.
The model considered the adverse ocular events (cataracts, elevated intraocular pressure, retinal detachment, endophthalmitis, and intravitreal haemorrhage) and adverse cardiovascular events (acute myocardial infarction, ischemic stroke, and other types of cardiovascular events) that may occur during treatment for DME. Endophthalmitis and increased intraocular pressure can be treated using combined medication and surgery or medication alone. Overall, 70% of patients with endophthalmitis receive pharmacologic treatment alone regardless of the treatment option for DME, whereas 100% of patients with increased intraocular pressure receive pharmacologic treatment. The model did not include surgery as a treatment for intraocular hypertension.Table 2.
Table 2. Follow-up visits, diagnostic tests per year, and percentage of patients with adverse events
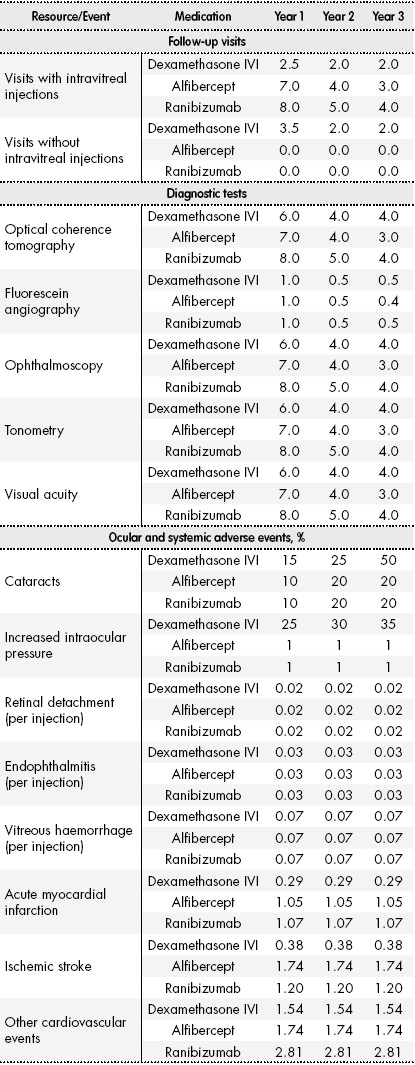
IVI, intravitreal implant.
The incidence of adverse ocular events and resource utilisation in their management were determined by the expert panel according to standard clinical practice, whereas the incidence of cardiovascular events was established using data from the pivotal clinical trials of the therapeutic options5 6-7.
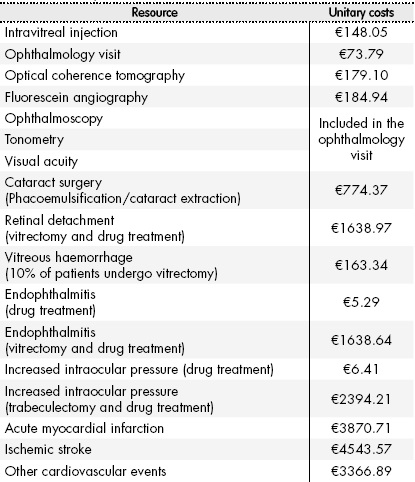
All costs are expressed in 2016 euros.Table 3shows the unitary costs of the healthcare resources included in the analysis, which were obtained from the literature and from national cost databases19 20 21-22.
Sensitivity analysis and alternative scenarios
We performed several univariate and multivariate sensitivity analyses, modifying the values of different parameters in order to incorporate the uncertainty into the analysis and observe the effect of these modifications on the results. We included the following parameters in the sensitivity analysis: the percentage of patients diagnosed with DME receiving treatment, unitary costs, the cost of intravitreal injections, the number of dexamethasone IVI injections per year, the cost of managing adverse cardiovascular events, the incidence of cataracts associated with antiangiogenic drugs, and the price of therapeutic alternatives (EFP with or without the deduction stipulated in RDL 8/2010). We also modified the percentage of usage of dexamethasone IVI and the other therapeutic alternatives (Table 1). We also considered three alternative scenarios to assess different healthcare regions with bigger populations (100,000, 250,000, and 500,000 adults) than that of the initial scenario.
Results
After applying epidemiological data for DME in Spain to a healthcare region with 25,000 adult inhabitants, we estimated that 100, 112, and 124 patients would be eligible for treatment per year over the 3-year study period.
In the scenario without dexamethasone IVI, the total annual cost of treating DME in these patients would be €835,197 (year 1), €606,004 (year 2), and €555,227 (year 3). In the scenario with dexamethasone IVI, the total annual costs would be €800,167 (year 1), €595,262 (year 2), and €550,176 (year 3). Thus, the inclusion of this treatment modality in the therapeutic arsenal for DME would produce budget savings of 4.2% (year 1), 1.8% (year 2), and 0.9% (year 3) involving reductions of €35,030, €10,743, and €5,051, respectively (Table 4). The annual cost of treatment per patient would be reduced by €350.31 (year 1), €95.97 (year 2), and €40.80 (year 3).
Table 4. Results of the budget impact analysis (base case and sensitivity analysis)
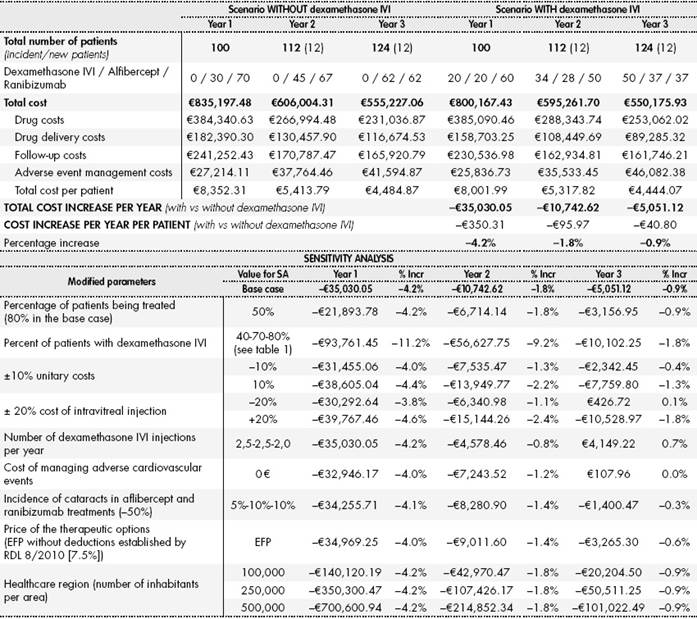
% Incr, % increase of costs in the scenario with dexamethasone IVI vs the scenario without dexamethasone IVI; EFP, ex-factory price; IVI, intravitreal implant; RDL, Royal Decree-Law; SA, sensitivity analysis.
Relative to the scenario without dexamethasone IVI, the scenario with dexamethasone IVI would have led to an overall saving of 5% in drug costs over the 3-year study period (0.2%, 8%, and 9.5% per year, respectively). Drug delivery and monitoring costs would provide the greatest savings in total costs. Drug administration costs and monitoring costs would have been between 13% and 23.5% lower and between 2.5% and 4.6% lower, respectively. In the scenario with dexamethasone IVI, for the whole analysis period, drug delivery costs and monitoring costs would have been 17.01% and 3.93% lower, respectively.
Sensitivity analyses showed that an increase in the use of dexamethasone IVI would further reduce the annual costs relative to the scenario without the implant. The sensitivity analysis also showed that an increase in unitary costs of healthcare resources (excluding drug costs) would increase the total cost in the scenario without dexamethasone (drug delivery and follow-up) which is already the scenario with greater costs. Thus, this would increase the savings between scenarios due to the introduction of dexamethasone IVI. However, several factors could reduce the potential savings derived from the introduction of dexamethasone IVI. These factors include: reductions in the unitary costs of healthcare resources, not considering the cost of managing adverse systemic events, a decrease in the incidence of cataracts in antiangiogenic therapies, and increasing the number of dexamethasone IVI injections per year (Table 4).
For each of the 3-year analysis period, the total cost in a population of 100,000 adults (400 prevalent patients) would be €3.3 million, €2.4 million, and €2.2 million in the scenario without dexamethasone IVI and €3.2 million, €2.4 million, and €2.2 million in the scenario with dexamethasone IVI, respectively. In a medium-sized health area with a population of 250,000 adults (1,000 prevalent patients), for each of the 3 years the total cost of treatment for DME would be €8.4 million, €6.1 million, and €5.6 million in the scenario without dexamethasone IVI. The scenario with dexamethasone IVI would led to savings of €350,300, €107,426, and €50,511 in each year, respectively. In an area with a population of 500,000 adults, the total cost of treating DME without dexamethasone IVI would be €16.7 million, €12.1 million, and €11.1 million euros for each of the 3 years in study, respectively. The introduction of dexamethasone IVI would led to savings of €700,601, €214,852, and €101,022, respectively.
Discussion
Diabetes mellitus is a highly prevalent disease and its prevalence is expected to increase over the coming years. Poor glycaemic control and subsequent complications, such as diabetic retinopathy and DME, are a great economic burden for the Spanish National Health System due to the challenge of managing this increasing number of patients.
According to recent economic data on DME in Spain, the estimated direct annual cost per patient with DME was €6,271 (excluding drug costs)13, whereas the estimated annual cost of treatment with antiangiogenic drugs was €7,154 with follow-up costs of €47423. DME can cause partial vision loss or blindness, which would entail an additional increase in indirect costs due to disability. The mean annual cost per patient due to permanent disability is €7,051, which is especially relevant in patients with bilateral DME (€11,712 in bilateral DME vs €4,284 in unilateral DME)13. A report on blindness in Spain24has suggested that the cost is around €5,100 per blind patient per year, entailing a total cost of around €360 million. There are additional costs that are paid by blind patients (€25,914) or those with impaired vision (€11,032)25. Besides good glycaemic control, opting for more effective treatments would reduce the economic burden on the Spanish National Health System service of treating patients with DME.
According to the model, the inclusion of dexamethasone IVI in the therapeutic arsenal for DME would save €35,030, €10,743, and €5,051 over each of the 3 years of analysis, respectively. These savings would mainly be due to the lower rate of treatments with dexamethasone IVI, which would in turn reduce drug delivery and follow-up costs. Annual savings per patient would be between €41 and €350. These estimations are corroborated by the alternative scenario in which there is increased use of dexamethasone IVI, suggesting that there would be even greater savings over the study period.
To the best of our knowledge, this study is the first to assess the impact on the healthcare budget of currently available treatments for DME in Spain, including dexamethasone IVI. A review of the literature found three recent economic assessment studies conducted in different countries that analysed the efficiency of several anti-VEGF therapies26 27-28. However, we found only two studies that included dexamethasone IVI25,29. One of these was a cost-effectiveness analysis conducted in Spain, which suggested that dexamethasone IVI was an efficient option with a cost of €2,050 per line of visual acuity gained25.
The present study has some limitations. The main limitation is related to the estimation of the target population. The robustness of the data is affected by the reliability of the epidemiological data available for DME, because the studies from which the data were obtained were conducted with relatively small reference populations17,18. The percentages of usage of the different therapeutic alternatives represent possible future trends in the usage of these drugs. The results obtained could vary if the estimated values of medication use do not closely reflect changes in the market.
The lack of robust information on the real-world management of patients with DME meant that some parameters had to be provided by the expert panel. Therefore, the following estimates may not accurately represent daily clinical practice in all Spanish healthcare centres: the number of intravitreal injections, the number of annual visits needed to treat patients with the therapeutic alternatives, resource utilisation caused by adverse events and patient follow-up.
Complete economic assessments, such as cost-effectiveness or cost-utility analyses, allow us to determine the comparative efficiency of the available alternatives for the treatment of a given disease. Budget impact analyses, such as that conducted in this study, involve partial economic assessments which analyse the economic impact of different therapies without assessing their effectiveness or efficacy, thus making them complementary to other assessments. This type of assessment should be seen as a useful tool for decision-making in healthcare, particularly in settings in which healthcare budget control is a priority. However, future studies should help to complement the information presented in this study and therefore assist in this decision-making process.
In conclusion, the use of dexamethasone IVI for the treatment of DME would entail savings to healthcare budgets. These savings would mainly be due to the reduced costs of drug delivery and patient follow-up.

