










 Custom services
Custom services
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Capecitabine is an oral fluoropyrimidine carbamate destined to an adjuvant therapy for nonmetastatic colorectal cancer (NCCN), either in monotherapy or in combination with oxaliplatin (XELOX scheme)1. Their most frequent adverse reactions include gastrointestinal disturbances, mucositis, palmar-plantar erythrodysesthesia (PPE), fatigue, asthenia, anorexia, neurotoxicity and hepatotoxicity1. There are other factors that can enhance such toxicity depending on the patient (ECOG scale (Eastern Cooperative Oncology Group), age, concomitant pathologies) and the drug (number of cycles, administered chemotherapy scheme)2.
In Spain, capecitabine was first marketed in 2001, and in 2012 generic presentations were comercialized. Regarding intravenous anti-neoplastic drugs, there are studies where the toxicity of generic and innovative formulations are compared. However, there are no studies on oral cytotoxic treatment3 4-5. This is important information, as the number of orally adapted cytotoxic molecules is increasing, allowing the patient to be more autonomous and preventing punctures and risks associated with catheters6.
Generic drugs have the same active ingredients, dose, pharmaceutical form and bioavailability as the innovative drug. For its commercialization, bioequivalence trials with the innovative drug are required: if both medicines are bioequivalent, they show the same security and effectiveness7.
For most therapies, acceptance limits of bioequivalence trials do not show clinically relevant differences in the activity of the active ingredient administered in the innovative or generic drug. However, in some fields such as Oncology, where drugs show high toxicity, this allowed interval between generic and innovative could become too large, especially bearing in mind that, frequently, the antineoplastic drugs therapeutic dose is dictated by the toxicity limit. This issue is particularly relevant when the oral route is used, as there may be variations in the release and absorption of the active ingredient. Those variations do not exist in the intravenous, where plasma concentrations depend on the infusion rate.
Therefore, the objective of this study is to analyze the frequency and severity of adverse reactions in NCCN-diagnosed patients, due to adjuvant treatment with two capecitabine formulations -innovative or generic- and/ or the chemotherapeutic regimen employed, either in monotherapy capecitabine or XELOX scheme.
Methods
Descriptive retrospective study of NCCN-diagnosed patients under adjuvant treatment with capecitabine, an innovative drug (Xeloda®) or a generic (Capecitabine Pharmaceutical Equivalent®). The two drugs are excipient, both at the tablet core and at the coating are identical.
The study was carried out in a second level hospital during two periods: November 2013-April 2014, where both formulations coexisted; and August 2016-May 2017, where only the generic formulation was available. Both periods arose from the small number of patients treated with the first generic formulation. The study was approved by the Ethics Committee for Clinical Research Center including all patients who received adjuvant treatment for NCCN. Those patients who received only one cycle of chemotherapy were not included.
The relevance of the chemotherapeutic scheme used in the appearance and severity of adverse events was assessed, as well as capecitabine as a monotherapy or XELOX scheme, and the relevance of drug administered capecitabine. For this final assessment, patients were divided into three groups (1: innovative drug-treated patients, 2: generic drug-treated patients, 3: patients treated with innovative and generic drugs combined).
Computerized medical records (Mambrino XXI®) and pharmacotherapeutic monitoring (Farmatools-Dominion® and Farhos-Oncology® v.5.0) were reviewed. Different variables, such as exposure (chemotherapy scheme and medication administration), control (age, sex, stage of disease, ECOG, starting dose, dose reduction, discontinuation of treatment and number of cycles received) and response (safety profile and severity, established as Common Terminology Criteria for Adverse Events, CTCAE v.4.03)8 were collected.
The statistical analysis of data was performed using SPSSR 15.0 program. (version for Windows®). A descriptive analysis of continuous or numeric variables was performed by applying central tendency and dispersion measures. Regarding the bivariate analysis, the relationship between different nominal categorical independent variables and the dependent variable was studied by chi-square. To analyze the means, T test was used for independent samples. p < 0.05 was considered statistically significant.
Results
A number of 50 patients were analyzed with a median age of 68 years (range: 47-88) and mostly male (34 patients; 68%). All patients had less than or equal to 2 ECOG at the onset of treatment, and the most common chemotherapy regimen was monotherapy (27 patients, 54%). Regarding drug administration, 22 (44%) patients received innovative medication, 15 (30%) was generic and 13 (26%) received a combination of generic and innovative.
Starting doses were all according to summary of product characteristics, except for 5 (10%) patients whose starting dose was reduced due to their bad general condition. During treatment, 32 (64%) patients had to reduce doses due to the drug’s safety profile, namely: PPE (17 patients, 34%), (7 patients; 14%) haematological toxicity, neurotoxicity (6 patients; 12%) and diarrhea (5 patients; 10%). In addition, 12 (24%) patients discontinued treatment, 3 of them (25%) due to progression, 4 of them (33%) due to adverse effects (hypertensive hypertrophic cardiomyopathy, thrombocytopenia, enteritis and malnutrition, PPE and neurotoxicity), 2 of them (17%) due to family and patient decision, and 3 of them (25%) for other reasons (surgery, recent cerebral stroke and endometrial biopsy).
The median of cycles administered was 7 (range: 2-8), and all patients had some adverse reaction except one (98%).
Regarding the administered chemotherapeutic scheme, the characteristics of the patients are listed in Table 1, with no statistically significant differences shown. The safety profile is also reflected inTable 1, where statistically significant differences were found in the frequency of PPE and total bilirubin alteration (more frequently with monotherapy) as well as in the frequency of neurotoxicity, thrombocytopenia, neutropenia, and gamma-glutamyl transpeptidase (GGT) alteration (more frequently with XELOX). The most common side effects for both groups of patients were diarrhea and/ or constipation, PPE, anemia and lymphopenia, while the less frequent side effects shown were nausea and/or vomiting, mucositis and increased total bilirubin, transaminases and GGT.
Table 1. Patient characteristics depending on the received chemotherapy scheme and adverse reactions presented

*p < 0.05.
**p ≤ 0.005.
GOT: glutamate oxaloacetate transaminase; GPT: glutamic pyruvic transaminase; GGT: gamma-glutamyl transpeptidase.
Regarding the capecitabine administered, the patient characteristics and safety profile are reflected in Table 2, where no statistically significant differences were found in any of the items. The most frequent adverse reactions for both groups of patients were diarrhea and/or constipation, PPE, thrombocytopenia and lymphopenia, while less frequent adverse reactions were nausea and/or vomiting, mucositis and GGT alteration.
Table 2. Patient characteristics depending on the type of drug administered and adverse reactions presented
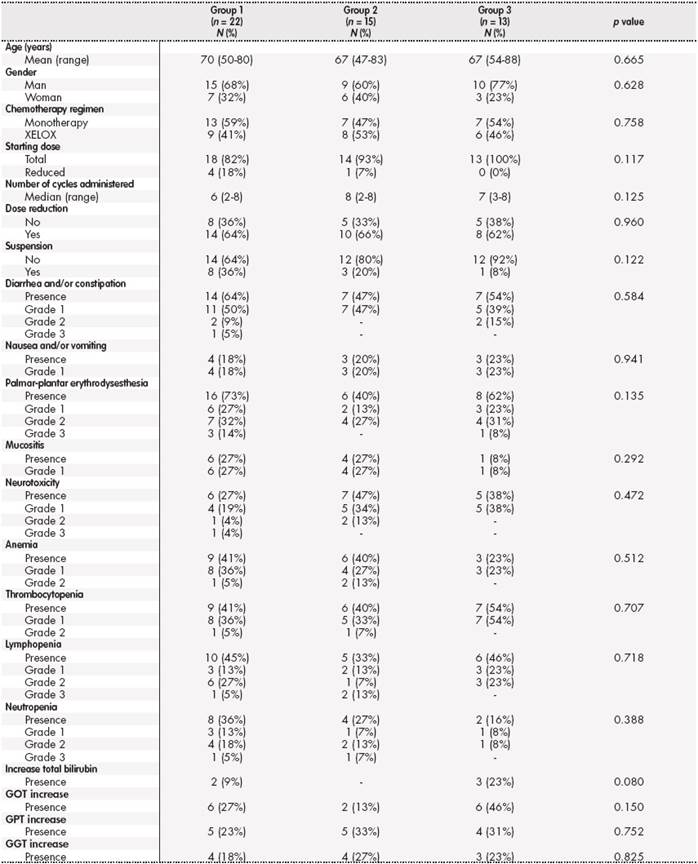
Group 1: patients treated with innovative drug; Group 2: patients treated with generic; Group 3: patients treated with a combination of innovative and generic medication. GOT: glutamate oxaloacetate transaminase; GPT: glutamic pyruvic transaminase; GGT: gamma-glutamyl transpeptidase.
Discussion
Comparing between capecitabine with monotherapy and capecitabine in combination with oxaliplatin, there is more PPE and an increased total bilirubin with capecitabine monotherapy, as well as an increased neurotoxicity, thrombocytopenia, neutropenia, and increased GGT with XELOX. These data are consistent with the literature, where most neurotoxicity and hematologic toxicity with XELOX versus capecitabine in monotherapy9 are observed. In our study, the most common side effect is PPE of any grade (74%), being similar to previous studies (62%). As for hyperbilirubinemia, in our study the rate stands at 19%; and 20% in previous studies10. Regarding the severity of adverse reactions, our study shows less adverse 3-4 grade effects, probably due to doses being reduced in clinical practice when mild adverse reactions occur, in order to prevent severe adverse events. Specifically, in previous studies, grade 3-4 EPP appears to be 3-4% (which it is not shown in our study), while grade 3-4 neurotoxicity represents 17% (in our study, 4%)11,12.
These data are not remarkable, as PPE is a common adverse reaction to capecitabine, and neurotoxicity is a very frequent and adverse event inherent in oxaliplatin1. The greatest EPP effect from capecitabine in monotherapy is likely due to the doses used, as the scheme uses about a 20% more capecitabine dose12,13.
The reason for a higher level of thrombocytopenia and neutropenia in the combined medication is caused by a cumulative toxicity as a result of a two antineoplastic drugs coadministration. Neutropenia is shown to be 48% in our study, while thrombocytopenia represents a 70% versus 20-30% rates reported in other studies12 13 14-15. However, when analyzing the severity of these adverse effects, the data are similar for grade 3-4 neutropenia (9% in our study versus 9.7% in literature) and favorable grade 3-4 thrombocytopenia (0% in our study versus 2.6% in literature)12 13 14-15. These differences, mainly in grade 1-2 adverse effects may be due to standard-marked values by different laboratories where biological samples are analyzed, as the CTCAE v. 4.03 does not define an interval to adverse grade 1 hematologic reactions.
Regarding adverse effects where no statistically significant differences are found, it should be highlighted that there is a trend of increased diarrhea and/or constipation, nausea and/or vomiting, anemia and lymphopenia with XELOX, most likely due to the joint administration of two cytotoxic drugs.
In the comparative analysis of innovative capecitabine and capecitabine as a generic drug, it is found that both medications are presented in the same form and qualitative composition of excipients, which did not show statistically significant differences in adverse events. Only a trend of greater PPE with the innovative formulation and a higher level of neurotoxicity with the generic formulation is observed. These trends could be justified, as the innovative formulation is mostly used as capecitabine in monotherapy (a scheme associated with PPE) and the generic formulation as XELOX (a scheme associated with neurotoxicity). Therefore, the safety profile of two capecitabine formulations -innovative and generic- shows to be associated with the chemotherapy scheme employed, and not the drug itself.
Lastly, the study’s main limitation was the sample size, which draws limited conclusions. A further randomized study could be performed to confirm these results. In addition, the scarcity of studies comparing oral cytotoxic drugs’ safety profiles of innovative and generic formulations shows the need for more studies like this to be carried out.

