










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAcción Psicológica
On-line version ISSN 2255-1271Print version ISSN 1578-908X
Acción psicol. vol.12 n.2 Madrid Dec. 2015
https://dx.doi.org/10.5944/ap.12.2.15783
The Relationship between Autobiographical Self-Focus and Memory Specificity/Overgenerality: Differences between Individuals with and without a Diagnosis of Depression
Relación entre Auto-Focus Autobiográfico y Especificidad/Sobregeneralización de la Memoria: Diferencias entre Personas con y sin un Diagnóstico de Depresión
Michael Bender1,2, María Carrera1,3 and Itxiar Alonso-Arbiol3
1 Tilburg University, the Netherlands
2 Gratia Christian College, Hong Kong
3 Universidad del País Vasco (UPV-EHU), España.
With funding from the Gipuzkoa Regional Council (DG10/02) and the University of the Basque Country UPV/EHU (General Grants for Groups, GIU11/29)
ABSTRACT
Research has revealed that clinical depression is related to reduced specificity and/or overgenerality in autobiographical memory. We set out to investigate this relationship by comparing depressed (n = 40) and non-depressed (n = 40) individuals not only in terms of autobiographical memory specificity/generality, but also in terms of narrative structure. Specificity was assessed with the Autobiographical Memory Test (AMT; Williams & Broadbent, 1986) and participants also provided open-ended memories, which were analyzed for autobiographical cognitive complexity (Woike, 1994). Narrative differentiation, as an indicator of self-focus, was negatively related to specificity and positively to overgenerality of particularly negative autobiographical memories - but only in the depressed sample. Relationships were significantly different among non-depressed individuals. Results are discussed in the context of the relation between specificity/overgenerality and self-focus.
Key words: autobiographical memory; specificity; depression; cognitive complexity.
RESUMEN
La investigación ha revelado que la depresión clínica está relacionada con una menor especificidad y/o sobregeneralización en la memoria autobiográfica. Nuestro objetivo consistió en estudiar dicha relación comparando personas deprimidas (n = 40) y no deprimidas (n = 40) no solo en términos de especificidad/generalidad de la memoria autobiográfica, sino también con respecto a la estructura narrativa. Se evaluó la especificidad con el Test de Memoria Autobiográfica (AMT; Williams & Broadbent, 1986). Los participantes también proporcionaron recuerdos en formato abierto, los cuales se analizaron en términos de complejidad cognitiva autobiográfica (Woike, 1994). La diferenciación narrativa, como un indicador de auto-focus, se relacionó negativamente con la especificidad y positivamente con la sobregeneralización de recuerdos autobiográficos negativos, pero solamente en la muestra de deprimidos; las asociaciones fueron significativamente diferentes entre personas no deprimidas. Se discuten los resultados en el contexto de la relación entre especificidad/sobregeneralización y auto-focus.
Palabras clave: memoria autobiográfica; especificidad; depresión; complexidad cognitiva.
Introduction
Depression is associated with individuals recalling overly categoric memories. This phenomenon has been described as an overgeneral memory retrieval style (OGM, Williams & Broadbent, 1986) or a reduced autobiographical memory specificity (rAMS). Differences in OGM and rAMS between depressed and non-depressed individuals have been widely documented, with depressed groups recalling less specific/more general memories than their non-depressed counterparts (for a review, see King et al., 2010; van Vreeswijk & de Wilde, 2004). The OGM/rAMS phenomenon has emerged as a stable cognitive marker for depression (Williams et al., 2007) and predicts its course (see Sumner, Griffith, & Mineka, 2010). OGM/rAMS is modifiable and can be reduced in non-clinical (e.g., Raes, Watkins, Williams, & Hermans, 2008), and dysphoric as well as depressed individuals (e.g., Watkins & Teasdale, 2004).
Such research and intervention efforts particularly focus on the management of rumination (reduction and/or induction), a maladaptive analytical self-focused style of thinking, which has been described as "repetitively focusing on the fact that one is depressed; on one's symptoms of depression; and on the causes, meaning, and consequences of depressive symptoms" (Nolen-Hoeksema, 1991, p. 569). Williams (1996) coined the term 'mnemonic interlock' to describe the process that prevents individuals from gaining access to event-specific autobiographical knowledge, thus remaining on the general level of memory retrieval - which in turn becomes a habitual cognitive style among depressed individuals. Rumination has been shown to be a mediator of the relationship between autobiographical memory (AM) specificity and depression levels (e.g., Debeer, Hermans, & Raes, 2009). Rumination also features prominently in the CaRFAX model proposed by Williams (2006). In this model, Williams concludes that OGM, or rAMS, can have adaptive value in avoiding negative memories as an affect regulation that can be functionally protective in the short-term - but not when it is becoming habitual. There is empirical evidence for OGM to be such a cognitive avoidance strategy, which is enacted differently among depressed and healthy individuals. Healthy individuals reduce a negative memory's specificity to avoid re-experiencing the emotions associated with it, but they do so in a context-dependent way, while depressed individuals do not (Debeer et al., 2012; Debeer, Raes, Williams, & Hermans, 2011). There is evidence that depressed and non-depressed individuals differ in the general extent to which they engage in OGM/rAMS, whether they engage in OGM/rAMS habitually or context-dependently, and ruminative self-focus has been associated with OGM-rAMS among depressed individuals.
To our knowledge, there has been no study so far that investigated whether narrative structure differs between depressed and non-depressed individuals. Narrative structure has been commonly used to provide insight into the uses of autobiographical remembering (Woike, 1994), differentiating between a self- and socially focused structure. We therefore set out to investigate whether there are differences in how depressed and non-depressed individuals, memory structure relates to OGM/rAMS.
Narrative Structure as an Indicator of Autobiographical Memory Use
The structure of an autobiographical memory can be taken as an indicator of its purpose by defining the parameters of potential uses (Robinson & Swanson, 1990). In more general terms, the features of a structure limit its potential applications, such that a hammer is good for hammering, but not for digging. Two main functions have been traditionally differentiated: an intrapersonal (self) and interpersonal (social) function (Robinson & Swanson, 1990; see also Bluck, 2003). Recent approaches have further differentiated self and social functions of autobiographical remembering (for an overview, see Pillemer, 2009). Functions of AM can be assessed with self-reports, like the Thinking about Life Experiences Questionnaire (TALE; Bluck & Alea, 2011), but individuals may have only limited introspective insight into their own memory activities (Pillemer, 2009). Research therefore focuses also on the narrative structure of autobiographical memories, which do not require an individual to arrive at introspective judgments about memory usage. Woike (1994) has documented two important ways in which individuals organize autobiographical information in narrative structure: differentiation indicates narrative elements indicating differences among objects, and integration includes elements indicating connections among objects. Differentiation has been linked to self-focused functions of AM (setting oneself apart from others), and integration has been linked to social functions of AM (Bender & Chasiotis, 2011; Woike, 1994). In other words, a memory that features predominantly self-focused structural elements (e.g., perceiving differences, comparing, and restricting narrative elements) is unlikely to be functionally appropriate when a person wants to rekindle a relationship or maintain a social bond - much like diverting the aforementioned hammer from its intended use by employing it for digging.
The Present Study
There has been much support for the importance of (ruminative) self-focus for depression (e.g., Raes, Schoofs, Griffith, & Hermans, 2012; Sumner, Griffith, & Mineka, 2011), but we are not aware of studies investigating narrative structure as an indicator of self-focus. We suggest that an investigation of the relationship between autobiographical narrative structure and memory specificity/overgenerality among depressed and non-depressed represents a novel and complementary methodological approach, which also comes with the added benefit of being unobtrusive (participants cannot easily form expectations about the investigation). We suggest that the heightened ruminative self-focus associated with depression is likely to also manifest itself in the narrative structure of autobiographical memories. Similar to the context-dependency of cognitive avoidance (Debeer et al., 2011, 2012), we expect differences between depressed and non-depressed in terms of the relationships between variables.
Three main hypotheses can be derived. First, we expect to replicate the relationship between depression and memory specificity/overgenerality such that depressed patients retrieve fewer specific -rAMS- (H1a) and more general (OGM) memories (H1b) than non-depressed individuals. Second, against the background of a more pronounced style of self-focused rumination, we predict that depressed individuals exhibit a more self-focused narrative structure in their autobiographical memories than non-depressed individuals (H2). Third, we expect to find both a negative association between narrative self-focus and autobiographical specificity (rAMS) (H3a) and a positive association between narrative self-focus and overgeneral autobiographical memories (OGM) among depressed (H3b) as opposed to non-depressed, where such associations are not expected. We refrained from specific predictions regarding a socially focused narrative structure (integration) among depressed and non-depressed individuals.
Method
Participants
A total of 80 individuals participated in the study1. The depressed group (n = 40) was admitted to an institution for treatment (psychological and/or psychopharmacological treatment). All were diagnosed as having a depressive episode2, and had no psychotic or obsessive symptoms according to the ICD-10 criteria (World Health Organization, 1992). Only individuals without confounding comorbidities3 were recruited to keep this subsample comparable with previous samples (see William & Broadbent, 1986; Williams & Dritschel, 1988). The non-depressed group (n = 40) consisted of individuals admitted to a general hospital for general treatment (to account for effects of being hospitalized). They did not suffer from depression. Both groups were recruited from institutions in Osnabrück, Germany.
Measures
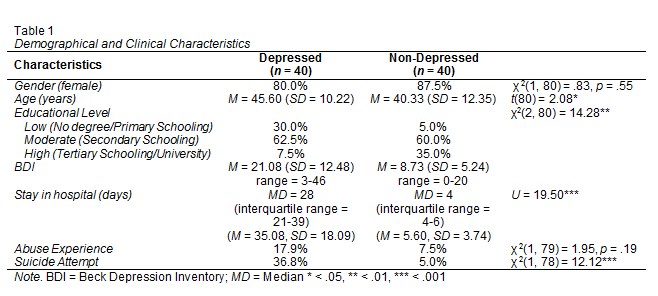
Demographics and Clinical Background. Participants reported gender, age, and educational level (for an overview, see Table 1). Information was gathered about their length of stay in hospital for the treatment, reported suicide attempts, and prior experiences of abuse, which have been shown to be related to OGM (King et al., 2010).
Beck Depression Inventory (BDI). The German version (Hautzinger, Bailer, Worall, & Keller, 1994) was used to assess depressive symptoms. It includes 21 items prompting participants to choose a description of how they have felt in the previous week. The response format is associated with the severity of the depression, ranging from 0 (absence of depressive symptoms) to 3. These points are summed, indicating the absence or severity of depression (< 11 = non-clinical; 12-17 = mild to moderate; > 18 = clinically relevant).
Autobiographical Memory Test (AMT). To assess OGM/rAMS we adapted the AMT (Williams & Broadbent, 1986). The AMT was presented individually, respondents were prompted after certain time intervals. Participants were given 60 seconds to recall a specific personal memory in response to five positive (happy, safe, interested, successfull and surprised) and five negative cue words (sorry, angry, clumsy, hurt -emotionally-, and lonely). Two examples were presented prior to recollection (one specific, one general). Participants were asked to write down their memories. These were coded in accordance with the coding system by Williams and Dritschel (1992), which differentiates four categories and is based on the traditional two category system by Williams and Broadbent (1986)4. The four categories are omissions (memory-unrelated content, e.g., "I am currently filling out a questionnaire."), categoric-general (description of a category of events, e.g., ". when a lot of people are around me."), extended (periods longer than a day, e.g., "Our honeymoon to Cornwall."), and specific (events lasting less than a day at a particular, identifiable point in time, e.g., "On January 13th, when my wife told me that she was pregnant."). Two trained researchers coded the memories (inter-rater agreement of r = .86). Categoric and extended memories were summed (omissions excluded) as an indicator of OGM, and specific memories indicated rAMS (lower scores = rAMS). Answers were also broken down according to type of cue word (positive vs. negative).
Autobiographical Cognitive Complexity. Participants were asked to write down their first childhood memory; as such types of memories reflect important concerns and current themes in people's lives (Singer & Salovey, 1993). Participants were instructed to write in complete sentences without the use of catchwords. Narratives were then subjected to a content analysis of cognitive complexity (Woike, 1994). The manual distinguishes between the categories of differentiation and integration that can occur at both simple and elaborated levels, but only elaborated levels were used here to follow guidelines from previous research (e.g., Bender & Chasiotis, 2011). Narrative elements of differentiation are structural aspects expressing the perception of differences. Such elements are contrasts ("We went to Cornwall, but not to Wales"), comparisons ("We liked Cornwall more than other regions of England"), and qualifying statements ("Before we arrived, we did not know whether we would like Cornwall"). Elements of integration are concerned with the perception of connections, which include similarities ("We both liked Cornwall"), dynamic, causal relationships ("Her way of thinking influenced me"), and concluding statements ("We will keep thinking about Cornwall for a long time"). The same researchers who analyzed the AMT also coded 20% of the memories, with an excellent inter-rater agreement of .90. One of the researchers (the first author) then coded the remainder of the memories. Frequencies of categories of differentiation and integration in the participants' narratives were summed to form the scores of differentiation and integration, respectively. These frequency scores were then weighted by memory length (i.e., wordcount, see Bender & Chasiotis, 2011, Woike, 1994).
Procedure
Data for the clinically depressed group was gathered in close coordination with the management and therapists/psychiatrists of the institutions. Depressed individuals were approached by their therapist/psychiatrist to inquire whether they were willing to participate in the study. After acquiring consent, an individual appointment with a research assistant was made to collect data in a quiet room of the clinic.
For the non-depressed sample, participants admitted to a general hospital were recruited. Patients came from the internal medicine and trauma surgery wards. No patients were considered who had a life-threatening disease or were (or had been during their hospital stay) in a life-threatening situation. In close coordination with the doctors and nurses, a research assistant approached each patient in their rooms individually to inquire about their willingness to participate in the study. Upon consent and scheduling the data collection, information was gathered.
The order of the instruments was the same for all participants (demographics, BDI, AMT). All participants took part in the study voluntarily, were informed that their data would be kept confidential, and that they could discontinue at any time.
Results
Before testing the hypotheses, we investigated whether sociodemographic control variables (see Table 1) affected the target variables. Women, across samples, reported significantly fewer categoric AMT memories (M = 2.33; SD = 2.20) than men (M = 3.85, SD = 2.67), t(78) = 2.20, p < .05. They also provided more specific AMT responses, t (38) = 4.58, p < .001, and fewer general answers than men, t (38) = 3.52, p < .001, within the non-depressed sample. Furthermore, age was negatively correlated with integration (r = -.34, p < .05). No further effects were observed. Consequently, the effects of gender and age were controlled in subsequent analyses.
Group Differences in OGM and rAMS
In order to replicate that depressed patients retrieve fewer specific (rAMS, H1a) and more general (OGM, H1b) memories, we analyzed the frequency of categories (i.e. specific, general) with a group (depressed, no depressed) × valence (positive, negative) using a mixed-design ANOVA model. As expected (H1a), depressed participants retrieved fewer specific memories than non-depressed individuals (see Table 2). No main effect of valence was detected, F(1,78) = .30, p = .59. There was, however, a significant group by valence interaction, F(1,78) = 8.41, p < .01, η2partial = .10. Depressed patients were significantly less specific than controls in providing answers to negative but not to positive cues. Further, as expected (H1b), depressed individuals recalled marginally more general memories. There was no significant effect of valence, F (1,78) = .008, p = .93, but the group by valence interaction was statistically significant, F (1,78) = 4.87, p < .05, η2partial = .06, with depressed individuals retrieving more general memories in response to negative, but not positive, cue words than the non-depressed control group.
Group Differences in Autobiographical Cognitive Complexity
Before we compared groups concerning their scores of differentiation and integration as indicators of cognitive complexity, we weighted categories by number of words to account for differences in length of narratives. Depressed (M = 62.58; SD = 47.15) and non-depressed (M = 73.03, SD = 48.66) individuals did not differ significantly in word count t(75) = 1.00, p = .34, Cohen's d = .25. To test whether depressed individuals include more structural markers of differentiation in their memories, and thereby exhibit a stronger self-focus (H2) than non-depressed, we compared mean differences in this score. Depressed individuals showed more differentiation (M = 0.03, SD = 0.02) than non-depressed individuals (M = 0.01, SD = 0.02); the difference was not statistically significant, t(75) = 1.52, p = .13, but the effect size was considerable: Cohen's d = .36. The medium effect size suggests that the absence of statistically significance in mean differences might be due to low power to detect them (resulting from a moderate sample size). We therefore inspected differences in the categories constituting differentiation, and found that depressed patients used significantly more comparisons in their memories than non-depressed individuals, t(75) = 2.27, p < .05, Cohen's d =.53. No differences in integration, t(75) = .10, p = .92, Cohen's d = .02, or its subcategories (all ps > .05, effect sizes close to zero) were found.
Relationship of Autobiographical Cognitive Complexity and OGM/rAMS
Given that OGM/rAMS is "encouraged by and itself is encouraging ruminative self-focus" (Williams, 1996, p. 261), we expected it to be associated with the narrative structure with which individuals organize their autobiographical memories. We predicted that differentiation, comprising narrative elements of separatedness as an indicator of self-focus (Woike, 1994), would be related negatively to specificity (H3a) and positively to overgenerality (H3b) among depressed individuals, but not among non-depressed.
We computed Pearson correlation coefficients to test these hypotheses. All correlations can be seen in Table 2.5 As expected, in the subsample of depressed individuals, differentiation was associated negatively with specificity, which seemed mainly driven by an effect of negative words among the depressed. This association did not appear for the non-depressed counterparts. The difference between these correlations was statistically significant. In other words, a differentiated narrative structure is associated with reduced autobiographical memory specificity (H3a). There was no relationship between differentiation and overgeneral recall, but an inspection of the relationship between differentiation and overgenerality in response to negative cue words revealed differentiation to be positively correlated with negative general memories in the depressed sample, which partially supports our hypothesis (H3b).
We expected no relationship between differentiation and overgenerality in the non-depressed sample. As mentioned earlier, a short-term style of selectively avoiding the retrieval of some specific memories can even be adaptive (see the CaRFAX model, Williams, 2006, see also Debeer et al., 2011, 2012). Interestingly, we found that differentiation was negatively related to negative general memories (with the coefficient being significantly different from the one in the depressed group). In other words, overgeneral memories are associated with an increased differentiation in the depressed sample, reflecting self-focus, but in the non-depressed sample, less overgenerality can be expected the higher the narrative differentiation is.
With regard to integration as an indicator of the social aspects of autobiographical structure, we also found differences between groups. Although there was no relationship between integration and specificity (it was marginally significant among the non-depressed respondents, p = .09), groups differed significantly in both direction and magnitude, as indicated by the statistically significant Fisher's Z for the comparison of the pairs of correlation coefficients: depressed individuals exhibited a positive correlation, but non-depressed a negative correlation. For non-depressed individuals, integration was negatively related to fewer specific negative memories - which was not true for depressed participants (Fisher's Z for the comparison of this pair of correlation coefficients was statistically significant at a marginal level). Other significant correlations or group differences did not emerge.
Discussion
By investigating the narrative structure of autobiographical memories, we introduced a novel and complementary methodological angle to the investigation of the link between self-focus and specificity among depressed and non-depressed individuals. There were three specific aims: (1) to replicate the link between AM specificity/overgenerality and depression, (2) to assess differences in narrative structure between depressed and non-depressed individuals, and (3) to investigate whether narrative self-focus and AM specificity/overgenerality are differentially related among depressed and non-depressed individuals.
We replicated the previously documented link between rAMS/OGM and depression, such that depressed individuals were less specific and more general in their autobiographical retrieval than non-depressed individuals, and we provided new evidence. Specifically, we found support for differences in narrative structure, as assessed by cognitive complexity, between depressed and non-depressed individuals. We observed that depressed individuals focused more on comparative, separating elements in their narrative structure. Finally, we could demonstrate the predicted pattern of narrative self-focus and specificity among depressed - but not non-depressed - individuals: A differentiated narrative structure, exemplifying a narrative self-focus, is associated with rAMS, particularly for negative cue words. This pattern extended partially to OGM, with narrative self-focus being associated with negative general memories in the depressed sample (but not other memory types).
In the non-depressed group, we found a decidedly different pattern: higher levels of differentiation in one's narrative structure are related to less OGM. This further highlights that relationships between self-focus and OGM are different for depressed and non-depressed individuals. While in the depressed group a self-focused narrative is associated with OGM (Watkins & Teasdale, 2001, 2004), self-serving, differentiated memories among non-depressed are likely useful, experiential part of an everyday use of autobiographical memories (see Bender & Chasiotis, 2011). No overall relationships with a socially oriented narrative (i.e., integration) emerged, but a close inspection revealed that the correlations were significantly different from one another. These differences suggest that there is a more positive association between social narrative focus among non-depressed than depressed individuals. Although it is too early to conclusively interpret such a finding, it adds to the above pattern of differences in the use of autobiographical memories, with depressed individuals exhibiting a decidedly different pattern than non-depressed.
Limitations and Perspective
There are several limitations to be taken into account. First of all, sample sizes are moderate, which prompts us to evaluate the obtained effects with caution. However, the samples are carefully selected, and the effects we have obtained are sizable, which bodes well for replication. Second, the depressed sample was already in treatment at the time of the study, so may not (or may to a lesser degree) exhibit a prototypically depressed style of reminiscence. This, however, would in fact render our investigation more conservative. Nevertheless, future studies should assess the stage at which individuals are in their treatment trajectory. Third, we did not differentiate between different narrative modes of self-focus, which might have distinct functional properties (Watkins & Teasdale, 2001, 2004). Dysfunctionality, i.e., rAMS and OGM, is ascribed to (ruminative) analytical self-focus ('brooding'). In contrast, reflection, but also mindfulness, that is, the direct, intuitive, experiential awareness of experience in the moment, is not associated with a dysfunctional retrieval style (Teasdale, 1999). However, given that our study is the first to investigate narrative structure, it is not yet clear how such distinctions would translate to the method employed here. Even more, there is some disagreement whether particularly brooding and reflection are separate constructs. Even in the distinction between brooding and reflection, Ciesla and Roberts (2007) reported a strong correlation (r = .81) between the two types of rumination and finally used a single dimension rumination score in their study. This notwithstanding, it is highly desirable for future studies to work towards an identification of structural narrative elements which might be more reflective of brooding or reflection, respectively, and to thereby derive firmer interpretations of the autobiographic narrative dysfunctionality among depressed individuals. Fourth, we found differences between depressed and non-depressed groups in the responses to cue words irrespective of valence. We found, however, that the differential relations between rAMS, OGM, and cognitive complexity between groups were driven particularly by negative cue words, which is not surprising as rumination has been related more to negative than positive memories (e.g., Thomsen, Schnieber, & Olesen, 2011; see also Kuyken & Dalgleish, 2011). Formerly depressed individuals also recall less frequently positive memories, suggesting the importance of considering valence (Werner-Seidler & Moulds, 2011). Increasingly, however there are inconsistencies in the evidence regarding the importance of valence (King et al., 2010), and it is not clear enough whether such differences between studies might not result from different sample characteristics or application criteria of measures used (van Vreeswijk & de Wilde, 2004, for a meta-analysis), cue words eliciting particular autobiographical themes irrespective of valence, or passive avoidant learning styles that are generalized to cues, again irrespective of their valence (Williams et al., 2007). Evidence is accumulating that, in terms of valence, the AMT is unidimensional (Griffith et al., 2009; Griffith, Kleim, Sumner, & Ehlers, 2012; Heron et al., 2012).
As a perspective, it seems worthwhile to capitalize on narrative structure to understand how (depressed) individuals actually use their memories in relation to the memory's specificity. Such insights could also be relevant for therapeutic interventions geared towards mindfulness or specificity training (e.g., Raes, Williams, & Hermans, 2009). We argue that focusing on the constituting narrative elements of self-focus may reveal when self-referential use of autobiographical memories is adaptative and when it is not, as well as which elements are particularly related to one or the other. This may - with a focus on interventions - enable us also to better understand not only at which level of specificity depressed individuals should learn to encode memories, but also on specifically how depressed individuals should structure their autobiographical narratives.
To conclude, we have set out to introduce narrative cognitive complexity (i.e., differentiation and integration) as a conceptually and methodologically innovative and useful indicator for the assessment of autobiographical self-focus to the study of autobiographical memory and depression. We could show that narrative self-focus and specificity/overgenerality are differentially related among the two groups. Narrative self-focus (differentiation) is positively related to AM specificity, and negatively (partially) to AM overgenerality - but only among depressed, not non-depressed individuals. We take this as an indicator that the way depressed individuals structure their memory narratives reflects a self-focus that is associated with depression. We suggest that narrative self- or other-focus as an indicator of how individuals recall their lives could be a useful addition to intervention efforts in the treatments for depression.
1 The initial sample consisted of 83 participants. Three participants (one depressed, two non-depressed) were excluded from further analysis as their data included significant outliers (i.e., three or more standard deviations above or below the mean) suggesting that they have not followed the questionnaire instructions. The final sample consisted, therefore, of 40 participants in each group.
2 All diagnoses were obtained from the medical records of the collaborating institutions. Of the depressed patients, 52.8% were diagnosed as meeting the criteria for a recurrent depression, the rest as having a first episode of a major depression. There were no differences between those groups; therefore, we did not distinguish between them in further analyses.
3 Individuals with the following comorbidities were not recruited: Organic disorders, (F0), Mental and behavioral disorders due to psychoactive substance use (F1), Schizophrenia, schizotypal and delusional disorders (F2), manic episodes (F30), bipolar disorders (F31), obsessive-compulsive disorders (F42), post-traumatic stress disorder, acute stress disorder, personality and behavior disorders (F60, F61, F62) and mental retardation (F70; ICD-10 classification, WHO, 1991). Comorbidities of the depressed sample were anxiety disorders (n = 4), adjustment disorders (n = 2) avoidant personality disorders (n = 2), personality disorders not otherwise specified (n = 2), other depressive disorder (n = 1) and bulimia (n = 1). The control sample did not report any psychological disorder.
4 We chose the four category system to retain comparability with previous studies, and to differentiate memory-unrelated omissions from general memories (Sumner et al., 2010; van Vreeswijk & de Wilde, 2004).
5 Three participants (two depressed, one non-depressed) did not complete their first childhood memory. Accordingly, correlations between AMT Categories and Categories of Cognitive Complexity are only reported for 38 depressed and 39 non-depressed participants.
References
1. Bender, M. & Chasiotis, A. (2011). Number of siblings explains cultural differences in autobiographical memory in PR China, Cameroon, and Germany. Journal of Cross-Cultural Psychology, 42, 998-1017. doi: http://dx.doi.org/10.1177/0022022110381127. [ Links ]
2. Bluck, S. (2003). Autobiographical memory: exploring its functions in everyday life. Memory, 11, 113-23. doi: http://dx.doi.org/10.1080/741938206. [ Links ]
3. Bluck, S. & Alea, N. (2011). Crafting the TALE: Construction of a measure to assess the functions of autobiographical remembering. Memory, 19, 470-486. doi: http://dx.doi.org/10.1080/09658211.2011.590500. [ Links ]
4. Ciesla, J. A. & Roberts, J. E. (2007). Rumination, negative cognition, and their interactive effects on depressed mood. Emotion, 7, 555-565. doi: http://dx.doi.org/10.1037/1528-3542.7.3.555. [ Links ]
5. Debeer, E., Hermans, D., & Raes, F. (2009). Associations between components of rumination and autobiographical memory specificity as measured by a Minimal Instructions Autobiographical Memory Test. Memory, 17, 892-903. doi: http://dx.doi.org/10.1080/09658210903376243. [ Links ]
6. Debeer, E., Raes, F., Claes, S., Vrieze, E., Williams, J. M. G., & Hermans, D. (2012). Relationship between cognitive avoidant coping and changes in overgeneral autobiographical memory retrieval following an acute stressor. Journal of Behavior Therapy and Experimental Psychiatry, 43 Suppl 1, S37-42. doi: http://dx.doi.org/10.1016/j.jbtep.2011.04.002. [ Links ]
7. Debeer, E., Raes, F., Williams, J. M. G., & Hermans, D. (2011). Context-dependent activation of reduced autobiographical memory specificity as an avoidant coping style. Emotion, 11, 1500-1506. doi: http://dx.doi.org/10.1037/a0024535. [ Links ]
8. Griffith, J. W., Sumner, J. A., Debeer, E., Raes, F., Hermans, D., Mineka, S., Craske, M. G. (2009). An item response theory/confirmatory factor analysis of the Autobiographical Memory Test. Memory, 17, 609-623. doi: http://dx.doi.org/10.1080/09658210902939348. [ Links ]
9. Griffith, J. W., Kleim, B., Sumner, J. A., & Ehlers, A. (2012). The factor structure of the Autobiographical Memory Test in recent trauma survivors. Psychological Assessment, 24, 640-646. doi: http://dx.doi.org/10.1037/a0026510. [ Links ]
10. Hautzinger, M., Bailer, M., Worall, H. & Keller, F. (1994). Beck-Depressions-Inventar (BDI) (Beck Depression Inventory). Bern, Switzerland: Verlag Hans Huber. [ Links ]
11. Heron, J., Crane, C., Gunnell, D., Lewis, G., Evans, J., & Williams, J. M. G. (2012). 40,000 memories in young teenagers: psychometric properties of the Autobiographical Memory Test in a UK cohort study. Memory, 20, 300-320. doi: http://dx.doi.org/10.1080/09658211.2012.656846. [ Links ]
12. King, M. J., MacDougall, A. G., Ferris, S. M., Levine, B., MacQueen, G. M., & McKinnon, M. C. (2010). A review of factors that moderate autobiographical memory performance in patients with major depressive disorder. Journal of Clinical & Experimental Neuropsychology, 32, 1122-1144. doi: http://dx.doi.org/10.1080/13803391003781874. [ Links ]
13. Kuyken, W. & Dalgleish, T. (2011). Overgeneral autobiographical memory in adolescents at risk for depression. Memory, 19, 241-250. doi: http://dx.doi.org/10.1080/09658211.2011.554421. [ Links ]
14. Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100, 569-582. doi: http://dx.doi.org/10.1037/0021-843X.100.4.569. [ Links ]
15. Pillemer, D. B. (2009). Twenty years after Baddeley (1988): Is the study of autobiographical memory fully functional? Applied Cognitive Psychology, 23, 1193-1208. doi: http://dx.doi.org/10.1002/acp.1619. [ Links ]
16. Raes, F., Schoofs, H., Griffith, J. W., & Hermans, D. (2012). Rumination relates to reduced autobiographical memory specificity in formerly depressed patients following a self-discrepancy challenge: The case of autobiographical memory specificity reactivity. Journal of Behavior Therapy and Experimental Psychiatry, 43, 1002-1007. doi: http://dx.doi.org/10.1016/j.jbtep.2012.03.003. [ Links ]
17. Raes, F., Watkins, E. R., Williams J. M. G., & Hermans, D. (2008). Non-ruminative processing reduces overgeneral autobiographical memory retrieval in students. Behaviour Research and Therapy, 46, 748-756. doi: http://dx.doi.org/10.1016/j.brat.2008.03.003. [ Links ]
18. Raes, F., Williams, J. M. G., & Hermans, D. (2009). Reducing cognitive vulnerability to depression: A preliminary investigation of Memory Specificity Training (MEST) in inpatients with depressive symptomatology. Journal of Behavior Therapy and Experimental Psychiatry, 40 24-38. doi: http://dx.doi.org/10.1016/j.jbtep.2008.03.001. [ Links ]
19. Robinson, J. A. & Swanson, K. L. (1990). Autobiographical memory: The next phase. Applied Cognitive Psychology, 4, 321-335. doi: http://dx.doi.org/10.1002/acp.2350040407. [ Links ]
20. Singer, J. A. & Salovey, P. (1993). The remembered self: Emotion and memory in personality. New York, NY: Free Press. [ Links ]
21. Sumner, J. A. (2012). The mechanisms underlying overgeneral autobiographical memory: An evaluative review of evidence for the CaR-FA-X model. Clinical Psychology Review, 32, 34-48. doi: http://dx.doi.org/10.1016/j.cpr.2011.10.003. [ Links ]
22. Sumner, J. A., Griffith, J. W., & Mineka, S. (2010). Overgeneral autobiographical memory as a predictor of the course of depression: A meta-analysis. Behaviour Research and Therapy, 48, 614-625. doi: http://dx.doi.org/10.1016/j.brat.2010.03.013. [ Links ]
23. Sumner, J. A., Griffith, J. W., & Mineka, S. (2011). Examining the mechanisms of overgeneral autobiographical memory: Capture and rumination, and impaired executive control. Memory, 19, 169-183 doi: http://dx.doi.org/10.1080/09658211.2010.541467. [ Links ]
24. Teasdale, J. D. (1999). Emotional processing, three modes of mind and the prevention of relapse in depression. Behaviour Research and Therapy, 37(Suppl 1), S53-77. doi: http://doi.org/10.1016/S0005-7967(99)00050-9. [ Links ]
25. Thomsen, D. K., Schnieber, A., & Olesen, M. H. (2011). Rumination is associated with the phenomenal characteristics of autobiographical memories and future scenarios. Memory, 19, 574-584. doi: http://dx.doi.org/10.1080/09658211.2011.591533. [ Links ]
26. Van Vreeswijk, M. F. & de Wilde, E. J. (2004). Autobiographical memory specificity, psychopathology, depressed mood and the use of the Autobiographical Memory Test: A meta-analysis. Behaviour Research and Therapy, 42, 731-743. doi: http://dx.doi.org/10.1016/S0005-7967(03)00194-3. [ Links ]
27. Waters, T. E. A. (2014). Relations between the functions of autobiographical memory and psychological wellbeing. Memory, 22, 265-275. doi: http://dx.doi.org/10.1080/09658211.2013.778293. [ Links ]
28. Watkins, E. & Teasdale, J. D. (2001). Rumination and overgeneral memory in depression: Effects of self-focus and analytic thinking. Journal of Abnormal Psychology, 110, 353-357. doi: http://dx.doi.org/10.1037//0021-843X.110.2.353. [ Links ]
29. Watkins, E. & Teasdale, J. D. (2004). Adaptive and maladaptive self-focus in depression. Journal of Affective Disorders, 82, 1-8. doi: http://dx.doi.org/10.1016/j.jad.2003.10.006. [ Links ]
30. Werner-Seidler, A., & Moulds, M. L. (2011). Autobiographical memory characteristics in depression vulnerability: formerly depressed individuals recall less vivid positive memories. Cognition & Emotion, 25, 1087-1103. doi: http://dx.doi.org/10.1080/02699931.2010.531007. [ Links ]
31. Williams, J. M. G. (1996). Depression and the specificity of autobiographical memory. In D. C. Rubin (Ed.), Remembering our past (pp. 244-267). New York, NY: Cambridge University Press. [ Links ]
32. Williams, J. M. G. (2006). Capture and rumination, functional avoidance, and executive control (CaRFAX): Three processes that underlie overgeneral memory. Cognition and Emotion, 20, 548-568. doi: http://dx.doi.org/10.1080/02699930500450465. [ Links ]
33. Williams, J. M. G. & Broadbent, K. (1986). Autobiographical memory in suicide attempters. Journal of Abnormal Psychology, 95, 144-149. doi: http://dx.doi.org/10.1037/0021-843X.95.2.144. [ Links ]
34. Williams, J. M. G. & Dritschel, B. (1992). Categoric and extended autobiographical memories. In M. A. Conway, D. C. Rubin, H. Spinnler, & W. Wagenaar (Eds.), Theoretical Perspectives on Autobiographical Memory (pp. 391-409). Dordrecht, The Netherlands: Kluwer Academic Publishers. [ Links ]
35. Williams, J. M. G., Barnhofer, T., Crane, C., Hermans, D., Raes, F., Watkins, E., & Dalgleish, T. (2007). Autobiographical memory specificity and emotional disorder. Psychological Bulletin, 133, 122-148. doi: http://dx.doi.org/10.1037/0033-2909.133.1.122. [ Links ]
36. Woike, B. (1994). The use of differentiation and integration processes: Empirical studies of "separate" and "connected" ways of thinking. Journal of Personality and Social Psychology, 67, 142-150. doi: http://dx.doi.org/10.1037/0022-3514.67.1.142. [ Links ]
37. World Health Organization. (1992). International statistical classification of diseases and related health problems,10th Revision (ICD-10). Geneva, Switzerland: Author. [ Links ]
![]() Correspondence:
Correspondence:
Michael Bender.
School of Social and Behavioural Sciences.
Tilburg University, the Netherlands;
Gratia Christian College, Hong Kong.
E-mail: m.bender@tilburguniversity.edu
Recibido: 13 de septiembre de 2015
Aceptado: 14 de noviembre de 2015

