










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.14 n.37 Murcia Jan. 2015
REVISIONES
Text messaging interventions to glycemic control in type 2 diabetes adults: systematic review
Mensajes de texto para el control glucémico en adultos con diabetes tipo 2: revisión sistemática
Valles Ortiz, Patricia M.*; Miranda Felix, Patricia** and García Sosa, Elia S.***
*PhD in Nursing Sciences, Faculty of Nursing at the Universidad Autónoma de Nuevo León. E-mail:
pvalles@uacj.mx
**Full time professor, Nursing Program at the Institute of Biomedical Sciences of the Universidad Autónoma de Ciudad Juárez.
***Professor at the Nursing School of the Universidad Autónoma de Sinaloa. México.
ABSTRACT
Objective: The aim of this systematic review was to evaluate the effectiveness interventions that have used text messaging in the reduction of glycosylated hemoglobin levels in type 2 diabetes patients.
Methods: a systematic review of articles published in the MEDLINE database, Elsevier, Springer, DARE, CINAHL, Scopus, and Open Access, eight interventions studies that met the inclusion criteria, were identified.
Results: Intervention using short message services of cellular phones improved HbA1c levels and improved the metabolic control in T2D adults.
Conclusions: The use of text messaging in the management of T2D, is presented as a suitable, practical, and well accepted technology, it has strong potential for providing effective, ongoing support in the future. However the research studies, showed that the evidence is not yet conclusive to the improvement in glycemic control.
Key words: type 2 diabetes; glycosylated hemoglobin; text messaging; mobile phone.
RESUMEN
Objetivo: Evaluar la evidencia disponible sobre la efectividad de las intervenciones que han utilizado mensajes de texto para la disminución de los niveles de hemoglobina glucosilada en el control glucémico en personas con DT2
Métodos: Se realizó una revisión sistemática en las bases de datos MEDLINE, Elsevier, Springer, DARE, CINAHL, Scopus, y Open Access, se identificaron ocho artículos que cumplieron con los criterios de elegibilidad para evaluar el uso de los mensajes de texto y los niveles de HbA1c.
Resultados: El envío de mensajes de texto a través de teléfono móvil mostró una disminución de los niveles de hemoglobina glucosilada en pacientes adultos con DT2.
Conclusiones: La utilización de mensajes de texto en la atención de los pacientes con DT2, se presenta como una tecnología factible y bien aceptada sin embargo los estudios señalaron que la evidencia aún no es concluyente en la mejoría del control glucémico.
Palabras clave: diabetes tipo 2; hemoglobina glucosilada; mensajes de texto; teléfono móvil.
Introduction
Diabetes has been identified as a health problem that affects high, middle and low income populations. The cost associated with its treatment and its complications represent the greatest burden not only to health services but also to patients and their families1. The World Health Organization (WHO) estimates that the number of people with diabetes in the world is 347 million and foresees that this figure will double by the year 2030. It also points out that 90% of cases belong to the category of type 2 diabetes (T2D). This data makes diabetes one of the greatest threats to public health in the 21st century2. In Mexico, T2D is considered the greatest health problem among the population. In the 2012 Survey of National Health3, 6.4 million people affirmed to have been diagnosed with diabetes. T2D is considered to be the primary cause of death and is the most frequent cause of premature impairment, blindness, terminal renal failure and non-traumatic amputations. Finally, it is a disease that is often not diagnosed until after its complications have appeared4,5.
Foremost, T2D is an illness that entails self-management, and its treatment is highly associated with behavior modification. Once diagnosed, people with T2D are responsible for managing their disease and, therefore, for carrying out both the pharmaceutical and the non-pharmaceutical actions prescribed in the therapeutic plan6. Performing these actions requires permanent support such as counseling and orientation from health professionals concerning diet, physical activity, medication oral intake, insulin injection and self-monitoring of capillary blood glucose in order to achieve optimum control of the disease and avoid or delay complications. Due to the long lasting nature of T2D, it is necessary to implement alternate strategies to ensure long term improvement7-9. Wireless phone service is one of the most widespread technologies throughout the world; thus, it is no surprise that it is considered for medical applications and those specific programs be developed to foster self-control of chronic diseases such as diabetes10-12.
For literary revision, the study used Cooper's seven step methodology13. All available evidence shows that information and communication technologies (ICTs) have enabled remote monitoring of results for different physiological variables, thus fostering better disease management in T2D patients and rendering additional benefits such as a decrease in the number of visits to the hospital while offering patients realtime support for their health condition. This technology makes it possible to send self-management-promoting reminders regarding their capillary glycaemia and levels of glycosylated hemoglobin (HbA1c), as well as motivation and educational messages conducive to self-care14,15. Although some studies show minor results concerning the utilization of information technologies to regulate T2D, message-based interventions oriented to promote patients' self-control reported an improvement in HbA1c and highlighted the establishment or the improvement of communication between health professionals and patients as one additional benefit17, 18
The relative ease with which a text message or a short message service (SMS) can be sent turns the utilization of mobile phones into an ideal means to exchange information between T2D patients and health professionals18,19 However, very few studies have been published so far which have examined whether mobile phone service is an effective tool to improve glycemic control or whether this kind of support offers enough advantages in self-management follow-up to enact its utilization. The use of remote monitoring systems, along with the intervention of health professionals, offers new opportunities for therapy adjustment in order to support T2D patients20.
Consequently, the aim of the revision was to identify the evidence provided by the interventions which evaluated the effectiveness of mobile phone text messages in the actual improvement of HbA1C levels.
Methods
The revision took place during the months of October and November of 2012. The work plan that the procedure would methodologically follow was outlined initially. The systematic revision was carried out with the utilization of Cooper's seven step model13: 1) Formulation of the problem, which stemmed from the research question: Are the messages sent through wireless mobile phone service useful in the glycemic control of T2D patients? 2) Search for literature, conducted according to selection criteria previously established. 3) Gathering of information in studies which were selected according to their pertinence to the stated purpose 4) Evaluation of the quality of the studies. 5) Analysis and interpretation of the studies' results. 6) Interpretation of evidence. 7) Reporting of results.
The selection criteria established to conduct the search included the following: articles in English and Spanish published between 2002 and 2012 which described the use of text messages sent through mobile phone service to adults involved in self-management of T2D to maintain their glycemic control and report on their HbA1 c.
In order to select information, an Internet search was conducted through the following data bases: Cochrane, CINAHL, Database of Abstracts of Reviews of Effectiveness (DARE), Academic Search Complete, MedicLatina, Open Access, MEDLINE, CENTRAL, ScienceDirect and Academic Google. The key terms used were those obtained in the Medical Subject Headings (MeSH). The search strategy applied was the cross reference of terms and key words with the use of Boolean operators AND, OR and NOT and the end truncation symbols; * and " ".
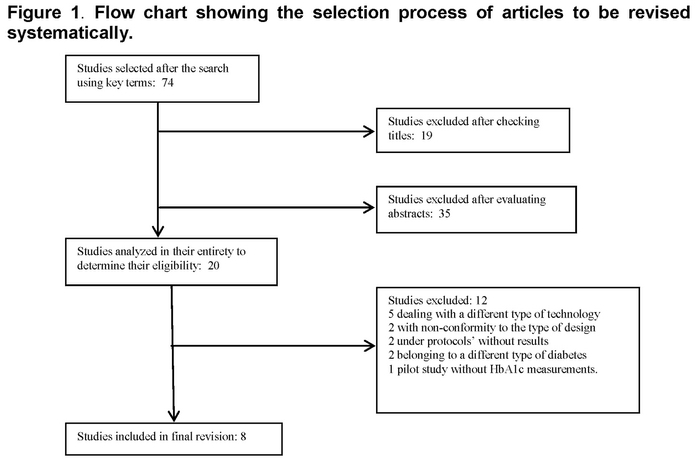
The articles selected from among the data bases were those mentioning the established key terms in their titles and abstracts. In order to obtain a final selection of articles, the authors performed a critical reading of all abstracts, obtaining a total of 74 publications. After examining their titles, 19 articles were excluded, and after evaluating the abstracts, 35 more were disregarded. Of the 20 remaining studies, 12 articles were excluded: 5 of them because they dealt with another type of technology, 2 of them because of inconformity with the type of design, 2 because they observed protocols without results, 2 because their samples included school-age patients with Type 1 diabetes (T1D), and a pilot study which did not include HbA1c measurements. Finally, only eight studies were considered suitable for revision (Figure 1). To ensure the quality of such studies, the Critical Appraisal Skills Program guide for clinical trials in Spanish (CASPe) was used. Furthermore, to analyze information, a format in Microsoft Excel was developed, which recorded the following data: Author, journal, year of publication, title of the article, aim or purpose of the study, study location, participants, description of the intervention, duration of the intervention, findings, main results and conclusions.
Results
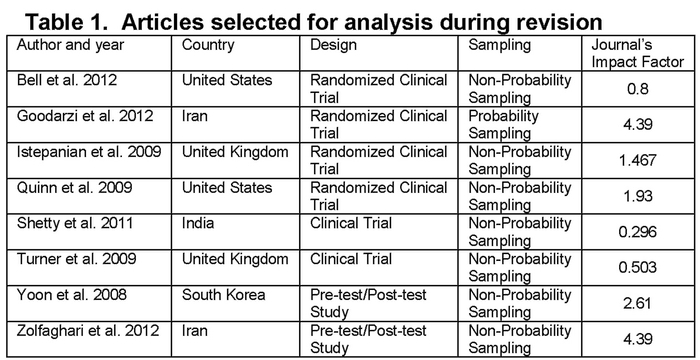
In the final revision, eight studies were analyzed, which complied with previously established selection criteria. Such studies took place in the following locations: 1 in South Korea, 2 in the United States (USA), 1 in India, 2 in Iran and 2 in the United Kingdom (UK). Five of them were randomized clinical trials, two were clinical trials and two were pre-test/post-test studies. The articles were published in different medical journals specializing in the treatment of diabetes, remote medicine and remote care (Table 1).
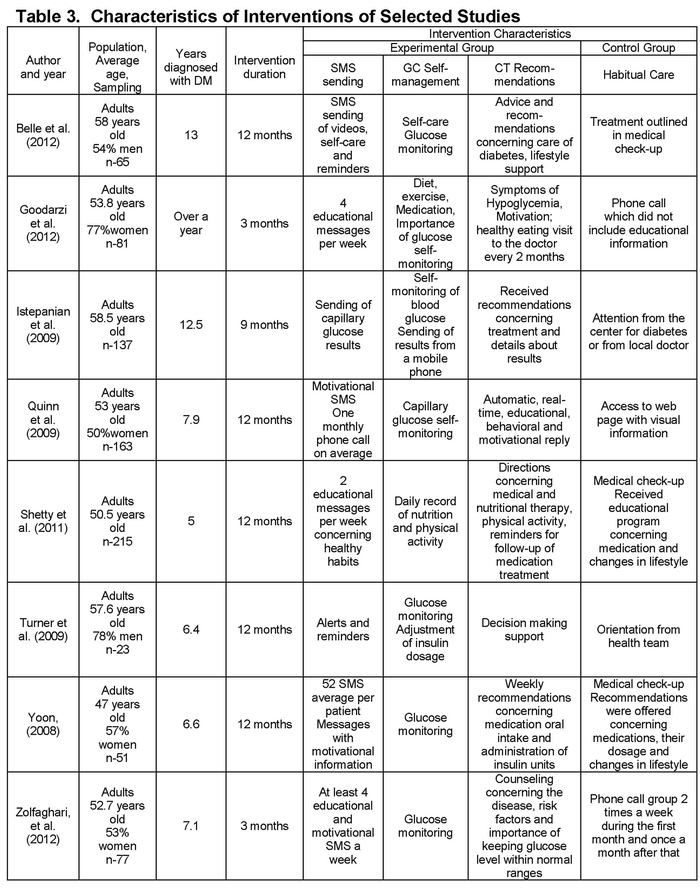
Intervention duration lasted between three and twelve months, and sample size varied between 23 and 215 participants. The revision excluded intervention studies which used the sending of text messages with information concerning self-care, management of prescribed therapeutics, clarification of doubts and surveillance of blood glucose levels, among other messages, to patients with T2D. Control groups received habitual attention given by the doctor, a specialized nurse of diabetes, or both, whether in the doctor's office, in the Health Care Center or in the Clinic for Diabetes according to the medical system of each country.
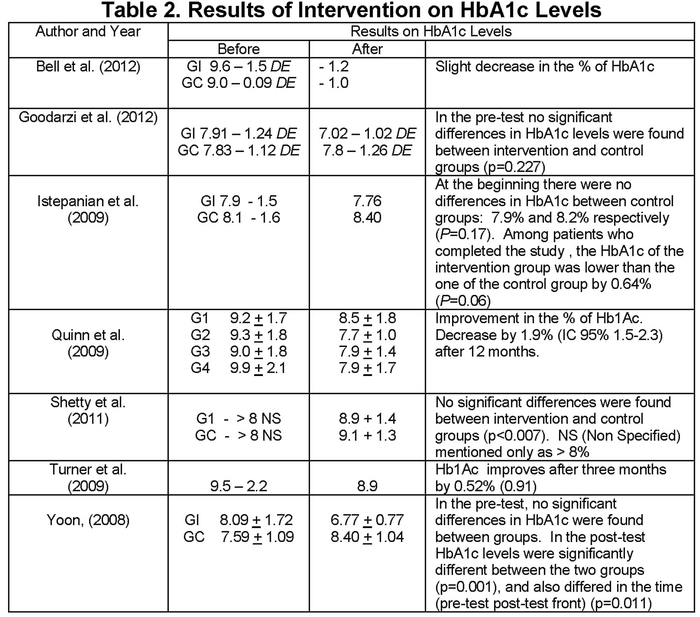
Turner and collaborators15 consider that the greatest achievement in self-management was that patients received educational messages in real time in response to the values of blood glucose reported. Quinn and collaborators17, in turn, highlighted that patients benefitted from the information concerning diabetes, medication, habits and lifestyle that was sent via messages to their mobile phones. In addition, both Yoon and Kim19 and Bell and collaborators mentioned that intervention using this technology is easy to implement and maintain, considering this a successful preventive factor in self-care in order to achieve glycemic control. Goodarzi and collaborators' findings22 demonstrated the effectiveness of intervention using mobile phone SMS in T2D management, drawing attention to the use of mobile phone service to provide remote education to these patients. Istepanian and collaborators16 did not find differences in the levels of HbA1c between intervention and control groups, explaining that sending SMS does not provide an advantage in habitual care; however, intervention did show a favorable 0.64% (P=0.06) difference in HbAlc. Shetty and collaborators' study14 showed that communication through SMS is well accepted by T2D patients and contributed to improving health results. Zolfaghari and collaborators23 underlined that using SMS through cell phones improved HbA1c levels as well as the adherence to prescribed treatment in patients with T2D (Table 2).
Six of the eight studies analyzed maintained contact exclusively through text messages. In one study, one weekly phone call was made by the patient's health provider if he had not received information about the patient three days after the date appointed to communicate results while another study compared the use of SMS with phone calls made to land lines23. (Table 3)
Discussion
The revision of intervention studies based on the use of SMS through cell phone showed a significant reduction in HbA1c levels; however, it cannot be affirmed that these data are a result of the exclusive use of text messages for self-management. It must be taken into consideration that while a significant reduction in HbA1c levels was observed in six of the eight studies, the period of duration of interventions was not the same for all studies. Glycemic control was determined by the HbA1c levels, and comparisons were drawn at the beginning and end of the intervention in both experimental and control groups. It was noted that participants in the intervention group in all eight studies obtained lower figures for their HbA1c levels at the end of the studies when compared to the control group. Istepanian and collaborators16 pointed out that no significant differences in HbA1c levels were found between the experimental and the control groups. Such data coincided with the results of other studies with a different type of intervention conducted in the United Kingdom such as the one by Farmer and collaborators in which they show that there is no convincing evidence to incorporate their findings into the self-care of T2D patients nor of the fact that providing greater intensive support or mere habitual care may have an effect on the improvement of glycemic control in well controlled T2D patients. Two of the studies provided support through phone calls17,23; another study utilized a video of care methods18 and the remaining five mention sending messages with educational and motivational content. From all this information it can be inferred that there was no uniformity among interventions to demonstrate that sending SMS exclusively is an effective strategy for maintaining T2D patients' glycemic control, since glycosylated hemoglobin levels were maintained or reduced to figures lower than 7%.
It is also noteworthy that the doctors and nursing staff using this technology for the first time shared the opinion that it does have the potential to improve patient care23. This opposes Turner and collaborators' reports showing concern from the medical staff of patients becoming dependent on orientation and guidance outside of the health care facilities15.
The rapid advance in information and communication technologies opens new possibilities for T2D self-management. The main findings demonstrated that intervention through counseling and/or orientation based on the use of mobile phone service through SMS actually improves HbA1c levels. It is also worth mentioning that it is necessary to conduct more studies on this option before generalizing its utilization by most people with T2D. However, it is undeniable that SMS through cell phones are associated with improvement in glycemic control, which is of particular interest due to the fact that the index of access to mobile phone service is quite high12,17.
Reliable information and efficient communication are both crucial elements in health care, and the use of proper technology may indeed increase the quality and outreach of both elements. On one hand, information is the basis for the knowledge that allows people to maintain their own health, and, on the other, social organizations help people reach a healthy state through health care systems25.
Conclusion
It was concluded that SMS represent a new communication technology which enables a person with a mobile phone to send a text message to another mobile phone. SMS are sent almost instantaneously to the destined cellular phone and can be read virtually anywhere, which is highly convenient for the receiver.
This service is also inexpensive, efficient, comfortable and less intrusive in comparison to a phone call. Currently, it is widely available, and more and more widely used throughout the world. Finally, the relative ease with which an SMS can be sent fosters both information exchange and ongoing communication between T2D patients and their medical staff.
During recent years, several applications of information technology based mainly on mobile phone service have been developed in order to help patients manage chronic conditions, such as T2D, outside clinics. However, the scarce number of existing articles was considered a limitation to this revision as no greater contribution of evidence was found to point out more conclusive results concerning glycemic control through this information technology.
Received: December 12, 2013
Accepted: 26 January 2014
References
1. International Diabetes Federation. (2011). IDF Diabetes Atlas, 5th edn. Brussels, Belgium: International Diabetes Federation. Disponible en: http://www.idf.org/diabetesatlas. Consultado Febrero, 2013. [ Links ]
2. World Health Organization. The diabetes program 2012. Disponible en: http://www.who.int/diabetes/en/. Consultado Abril, 2013. [ Links ]
3. Secretaria de Salud. Encuesta nacional de salud y nutrición 2012. Instituto Nacional de Salud Pública. Subsecretaria de Prevención y Promoción de la Salud. 2012. recuperado de: http://ensanut.insp.mx/. [ Links ]
4. Aguilar C, Gómez R, Gómez FJ. La diabetes tipo 2 en México: principales retos y posibles soluciones. Revista de la ALAD. 2011; 19(4):148-161. [ Links ]
5. Villalpando S, Rojas R, Shamah-Levy T, Ávila M, Gaona B, De la Cruz V, Rebollar R, Hernández L. Prevalence and distribution of type 2 diabetes mellitus in Mexican adult population: a probabilistic survey. Revista de Salud Pública de México. 2010; 52(lS): 19-26. [ Links ]
6. Hoyos T, Arteaga M, & Muñoz M. (2011). Factores de no adherencia al tratamiento en personas con Diabetes Mellitus tipo 2 en el domicilio. La visión del cuidador familiar. Revista de Investigación y Educación en Enfermería; 29(2):194-203. [ Links ]
7. American Diabetes Association. Standards of medical care in diabetes-2013. Diabetes Care. 2013; 36(1S): 11-66. [ Links ]
8. Chen L, Magliano D, Zimmet P. The worldwide epidemiology of type 2 diabetes mellitus: present and future perspectives. Nature Reviews, Endocrinology. 2012; 8: 228-236. [ Links ]
9. Lawrenson R, Joshy G, Eerens Y, Johnstone W. How do newly diagnosed patients with type 2 diabetes in the Waikato get their diabetes education? Journal of Primary Health Care. 2010; 2(4):303-310. [ Links ]
10. Bravo-Toledo R. Nuevas tecnologías. Actualización en Medicina Familiar. 2011; 7(6):356-357. [ Links ]
11. Alfaro M, Bonisb J, Bravo R, Fluitersd E, Minuée S. Nuevas tecnologías en atención primaria: personas, máquinas, historias y redes. Gaceta Sanitaria. 2012; 26(S):107-112. [ Links ]
12. Fischer H, Moore S, Ginosar D, Davidson A, Rice-Peterson C, Durfee M, Mackenzie T, Estacio R, Steele A. Care by cell phone: text messaging for chronic disease management. American Journal of Managerial Care. 2012; 18(2): 42-47. [ Links ]
13. Cooper H. (2010). Research synthesis and meta-analysis: a step by step approach (4th ed). SAGE Publications, Inc. thousand Oaks, California. [ Links ]
14. Shetty AS., Chamukuttan S., Nanditha A., Champat RK., Ramachandran A. Reinforcement of adherence to prescription recommendations in Asian Indian diabetes patients using short message service (sms)-a pilot study. Journal of the Association of Physicians of India. 2011; 59. [ Links ]
15. Turner J., Larsen M., Tarassenko L., Neil A., Farmer A. Implementation of telehealth support for patients with type 2 diabetes using insulin treatment: an exploratory study. Informatics in Primary Care. 2009;17:47-53. [ Links ]
16. Istepanian K, Harry D, Moutosammy N, Sungoor A, Tang B, Earle KA. Evaluation of a mobile phone telemonitoring system for glycemic control in patients with diabetes Journal of Telemedecine and Telecare. 2009; 15:125-128. [ Links ]
17. Quinn CC., Gruber-Baldini AL., Shardell M., Weed K., Clough SS., Peeples M., Terrin M., Bronich-HallL., Barr E., Lender D. Mobile diabetes intervention study: testing a personalized treatment/behavioral communication intervention for blood glucose control. Contemporary Clinical Trials. 2009; 30(4): 334-46. [ Links ]
18. Yoon KH, Kim HS. A short message service by cellular phone in type 2 diabetic patients for 12 months. Diabetes Research and Clinical Practice. 2008; 79:256-261. [ Links ]
19. Bell AM., Fonda SJ., Walker MS., Schmidt V., Vigersky RA. Mobile phone-based video messages for diabetes self-care support. Journal of Diabetes Science and Technology. 2012; 6(2):310-319. [ Links ]
20. Chang, K., Davis, R., Birt, J., Castelluccio, P., Woodbridge, P., Marrero, D. Nurse practitioner-based diabetes care management impact of telehealth or telephone intervention on glycemic control. Manage Health Outcomes. 2007; 15(6): 377-385. [ Links ]
21. Institute of Health Sciences of Oxford University (2008). Critical Appraisal Skills Programme Español-CASPe. Boston, MA: Oxford University. Disponible en: http://www.redcaspe.org/herram ientas/index.htm. [ Links ]
22. Goodarzi M., Ebrahimzadeh I, Rabi A, Saedipoor B, Jafarabadi MA. Impact of distance education via mobile phone text messaging on knowledge, attitude, practice and self-efficacy of patients with type 2 diabetes mellitus in Iran. Journal of Diabetes & Metabolic Disorders. 2012; 11(10). [ Links ]
23. Zolfaghari M., Mousavifar SA., Haghani H. Mobile phone text messaging and telephone follow-up in type 2 diabetic patients for 3 months: a comparative study. Journal of Diabetes & Metabolic Disorders. 2012; 11(7). [ Links ]
24. Farmer A., Wade A., Goyder E., Yudkin P., French D., Craven A., Holman R., Kinmonth A-L., Neil A. Impact of self-monitoring of blood glucose in the management of patients with non-insulin treated diabetes: open parallel group randomized trial. British Medical Journal. 2007; July 21;335:132. [ Links ]
25. Chetley, A., Davies, J., Trude, B., McConnell, H., Ramirez, R. Improving health, connecting people: the role of ICTs in the health sector of developing countries. Washington, D.C., World Bank, Information for Development Program. 2006 May 31. (25). [ Links ]

