










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.15 n.43 Murcia Jul. 2016
CLÍNICA
Quality of life of patients with chronic kidneydisease undergoing hemodialysis
Calidad de vida en pacientes con insuficiencia renal crónica en hemodiálisis
Qualidade de vida de pacientes com insuficiência renal crônica em tratamento hemodialítico
Costa, Gabrielle Morais Arruda*; Pinheiro, Maria Berenice Gomes Nascimento**; Medeiros, Soraya Maria de***; Costa, Raphael Raniere de Oliveira**** and Cossi, Marcelly Santos*****
*Nurse. Member of the Research Group Kaleidoscope Nursing Education of the Federal University of Rio Grande do Norte - UFRN. Natal, Rio Grande do Norte.
**Nurse. Master' s Degree in Public Health. Professor of the Federal University of Campina Grande - UFCG. Campina Grande, Paraíba
***Ph.D. in Nursing. Professor of the Federal University of Rio Grande do Norte, leader of the Research Group Kaleidoscope Nursing Education UFRN.
**** Master' s Degree in Nursing. Ph.D.of the PostGraduate Nursing Program of the Federal University of Rio Grande do Norte - UFRN. Member of the Research Group Kaleidoscope Nursing Education - UFRN. E-mail: raphaelraniere@hotmail.com
*****Nurse. Master's Degree of the Post-Graduate Nursing Program of the Federal University of Rio Grande do Norte - UFRN. Member of the Research Group Kaleidoscope Nursing Education- UFRN. Brazil.
ABSTRACT
This research aimed to evaluate the quality of life of patients with chronic kidney disease undergoing hemodialysis treatment, as well as to characterize them, identify the factors that affect and influence them. This is a field study, descriptive, cross-sectional and quantitative approach performed in a hemodialysis center in Alto Sertão da Paraíba, Cajazeiras municipality. A socio-demographic questionnaire and the WHOQOL-BREF were used to evaluate the average domains and quality of life of participants, as well as the Pearson correlation test between variables obtained. The sample consisted of 39 subjects. The research included patients of both genders: 54% male and 46% female and has, concerning age group, high prevalence for older than 51 years old. In general, the most affected domain among the participants was the physical domain (FD), averaging 59.44, and the best preserved was the social domain (SD), averaging 72.87, reflecting on Quality of Life (QOL) of patients with RI, which showed an average of 64.96. Through the Pearson correlation test, there was a significant relationship between the various domains, where all domains showed a high correlation with QOL. It was concluded that patients with CKDundergoing hemodialysis treatment have a regular quality of life, and the knowledge of the professionals about this issue is paramount to reach an optimization in the care of patients with CKD undergoing hemodialysis treatment.
Key words: Quality of life; Hemodialysis; kidney failure.
RESUMEN
Esta investigación tuvo como objetivo evaluar la calidad de vida de los pacientes con enfermedad renal crónica en hemodiálisis, así como caracterizarlos, identificar los factores que afectan e influyen en la misma. Se trata de un estudio de campo, descriptivo, transversal y cuantitativo realizado en un centro de hemodiálisis en el Alto Sertão da Paraíba, municipio Cajazeiras. Se utilizó un cuestionario sociodemográfico y el WHOQOL-BREF para evaluar los puntajes promedio y la calidad de vida de los participantes, así como la prueba de correlación de Pearson entre las variables obtenidas. La muestra estuvo conformada por 39 sujetos. La investigación incluyó a pacientes de ambos sexos: 54% hombres y 46% mujeres y tiene, con respecto a la edad, alta prevalencia de más de 51 años. En general, el dominio más afectado entre los participantes fue el dominio físico (DF), con un promedio de 59.44, y el mejor conservado fue el dominio social (DS), con un promedio de 72.87, reflejado en la Calidad de Vida (QOL) de los pacientes con IR, que mostró un promedio de 64.96. A través del test de correlación de Pearson, hubo una relación significativa entre los diversos ámbitos en los que todos los dominios mostraron una alta correlación con la calidad de vida. Llegamos a la conclusión de que los pacientes con enfermedad renal crónica en hemodiálisis tienen una calidad de vida regular, y el conocimiento de los profesionales sobre este tema es de suma importancia para alcanzar una optimización en el cuidado de los pacientes con IRC sometidos a hemodiálisis.
Palabras clave: Calidad de Vida; Hemodiálisis; Insuficiencia renal.
RESUMO
Esta pesquisa objetivou avaliar a qualidade de vida dos pacientes portadores de doença renal crônica em tratamento hemodialítico, bem como caracterizá-los, identificar os fatores que interferem e influenciam na mesma. Trata-se de um estudo de campo, descritivo, transversal, com abordagem quantitativa realizada em um centro de hemodiálise do Alto Sertão da Paraíba, município de Cajazeiras. Foi utilizado um questionário sócio-demográfico e o Whoqol-bref para avaliar a média dos domínios e da qualidade de vida dos participantes, bem como o teste de Correlação de Pearson entre as variáveis obtidas. A amostra foi composta por 39 sujeitos. A pesquisa contou com pacientes de ambos os sexos: 54% do sexo masculino e 46% do sexo feminino e possui, com relação a faixa etária, alta prevalência para maiores de 51 anos. De modo geral, o domínio mais prejudicado entre os participantes foi o físico (DF), com média de 59,44, e o mais preservado foi o domínio social (DS), com média de 72,87, refletindo na Qualidade de Vida (QV) dos portadores de IR, que apresentaram uma média de 64,96. Através do teste de Correlação Pearson observou-se relação de significância entre os diversos domínios, onde todos os domínios apresentaram uma correlação alta com a QV. Conclui-se que os pacientes com IRC em tratamento hemodialítico possuem uma qualidade de vida regular, e que o conhecimento dos profissionais acerca deste assunto é primordial para que alcance uma otimização na assistência aos portadores de IRC em tratamento hemodialítico.
Palavras chave: Qualidade de Vida; Hemodiálise; Insuficiência renal.
Introduction
Chronic diseases have received increased attention from health professionals by presenting high rate of morbidity and mortality rates. Thus, it becomes a major concern for the public health field. Among the many chronic diseases that affect the population, Chronic Kidney Disease (CKD) is considered a pathology without expectation of the cure, with rapidly and progressive evolution, triggering diverse reactions for patients and compromise the quality of life (QOL)(1-2).
This disease is present in a large number of people and has a gradual and irreversible evolution, generating complications and disorders for patients. Dialysis is the main treatment for this disease.
The CKD and dialysis treatment trigger different situations for the patient, affecting different aspects related to health. The treatment conditions and chronic disease progression limits the CKD carrier's and, therefore, they are aggressive factors that trigger stress, social isolation as well as limitations to the possibility of locomotion and tours, decreased physical activity, dependency and feelings of fear and uncertainty regarding health and welfare. Therefore, the QOL is an extremely important factor because it directly affects the effectiveness of treatments and interventions in health(3-1).
Even with technological and therapeutic advances achieved until today, to improve the clinical condition and increase CKD carrier survival, their level of quality of life continues to decline (4).
Knowing that nursing care constantly needs changes to meet the individual needs, it is necessary, and extremely important, to advance in the search field to improve the quality of nursing care and consequently, the individual QOL(5).
Therefore, it was decided to conduct this study to evaluate the QOL of CKD patients undergoing dialysis treatment, of Alto do Sertão, Paraíba, Brazil and to characterize them as the socio-demographic variables, to investigate the factors that interfere with daily activities of patients and identify the correlation between the overall quality of life and the diverse domains of WHOQOL-BREF.
Materials and Methods
This is a descriptive and transversal study, with a quantitative approach. This study was conducted in the Dialysis Center of Cajazeiras (CHC), Paraíba state, Brazil. The Dialysis Center of Cajazeiras is added to the physical structure of the Regional Hospital in Cajazeiras (HRC) and it is small. The CHC serves 15 surrounding municipalities and has a team of doctors, nurses and nursing technicians who are responsible for the dialysis process and for maintaining the health status of the patient during the session.
The initial sample consisted of 50 patients with CKD undergoing dialysis treatment in CHC. The research included patients with CKD, over 18 years old, both genders, who were undergoing dialysis treatment for more than six months. Patients who did not accept voluntarily to sign the Informed Consent form (IC) were excluded, as well as people with mental disorders, or those who, at the time of data collection showed a decreased level of consciousness. Also, patients who did not attend the dialysis unit during the stipulated period for data collection were excluded. Once applied the inclusion criteria, the final sample consisted of 39 subjects.
The study was approved by the Ethics Research Committee of the Federal University of Campina Grande, Paraíba, Brazil, under protocol number 338.082, and developed obeying and respecting all the conditions required by Resolution 196/96 of the National Health Council (NHC).
As data collection instruments, two instruments were used: a questionnaire focused on socio-demographic profile of the participants and other for the analysis of quality of life, WHOQOL-BREF(7).
Data were obtained in a spreadsheet of Excel program for Windows, 2010version, checked, corrected and imported into the Statistical Package for Social Sciences (SPSS Program), 17.0 version, for statistical analysis.
Results
Table 1 shows the socio-demographic data of CKD patient's undergoing dialysis treatment in Cajazeirascity.
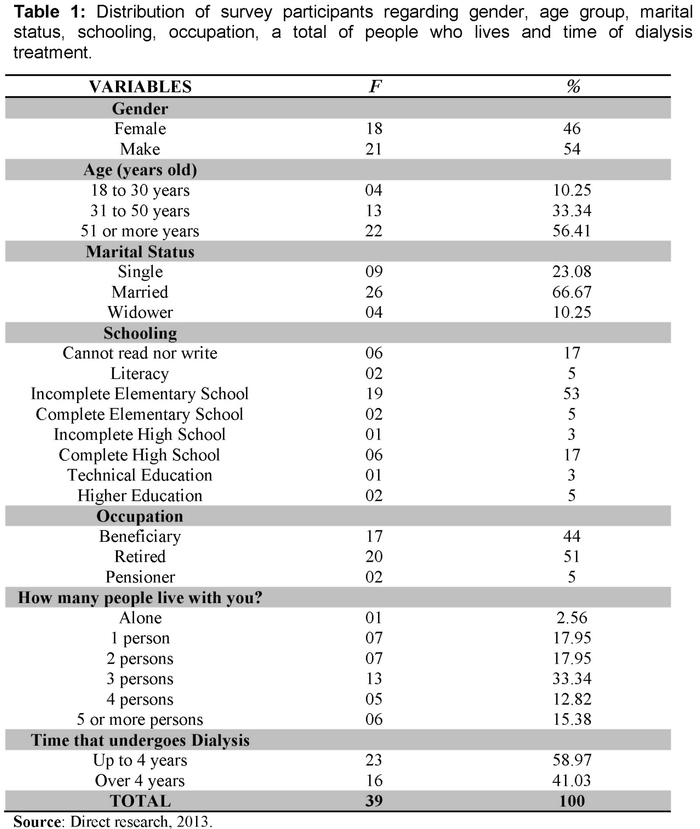
It is observed that, according to gender and age group, it is possible to analyze the rate of men who perform the treatment reaches a percentage of 54%; higher than women, representing 46% of the participants. One can also observe that, with increasing age group, there is an elevation in the prevalence rate of CKD in patients, getting the following results: between 18 and 30 years old, a percentage of 10.25% was obtained; from 31 to 50 years old 33.34% and from 51 years old onward, there is a prevalence of 56.41%.
It is possible to observe that such data have no contradiction when compared to dialysis sense conducted by SBN, in which it was found that the number of men who perform the treatment is higher than women; and the most prevalent age group in the treatment goes from 19 to 64 years old, increasing the incidence with advancing age(8).
It was observed that, regarding marital status, most of the interviewed are officially married (66.67%) and lives with their companions.
Thus, it was concluded that the study participants who were married, did not feel alone in facing the disease, overcoming obstacles and challenges posed by physical limitations caused by the illness.
According to the research data, it is possible to evaluate that the majority of the population have some instruction degree, with only 17% who can not read nor write and 5% have only literacy.
It should be noted that in the occupational/professional context of each participant, none is in labor activity. The study shows that 44% receive disease assistance, i.e., receive a specific benefit for CKD carrier's dependent undergoing hemodialysis treatment; 51% are retired, and 5% are pensioners.
The CKD is a disabling disease in the professional dimension, i.e., imposes difficulties and physical limitations that cancel out, most of the time, the ability to work. In this study, specifically, 100% of the participants are unemployed.
As for the salary, the lack of jobs for this group generates conflicts. In the reports we identified a reduction in the standard of living because they enjoy only benefits/retirement/pension, being such situation an important factor in the change of QOL.
Another social aspect analyzed in this study was the observation of the number of people living alone or with others, being part of the family social life. It was observed that only 2.56% of them are living alone, statistics corresponding to one (01) person; as for the rest, 17.95% live with 01 or 02 persons; 33.34% live with 03 persons, constituting the majority of the population; 12.82% live with 04 persons, and 15.38% live with 05 or more persons.
To analyze the dialysis treatment time, those treated for more than six months were included, considering that during this period changes and variation in quality of life would be more evident. The patients then were divided, between those undergoing treatments for six months to four years, comprising a statistical value of 58.97%; and those undergoing dialysis for more than four (04) years, 41.03%.
At this stage, the data were analyzed according to the WHOQOL-BREF collection instrument, specific for the quality of life, applied to the CKD patients undergoing dialysis treatment in the city of Cajazeiras, Paraíba state.
The instrument has four domains, namely: physical, psychological, social and environmental; shown in the table below:
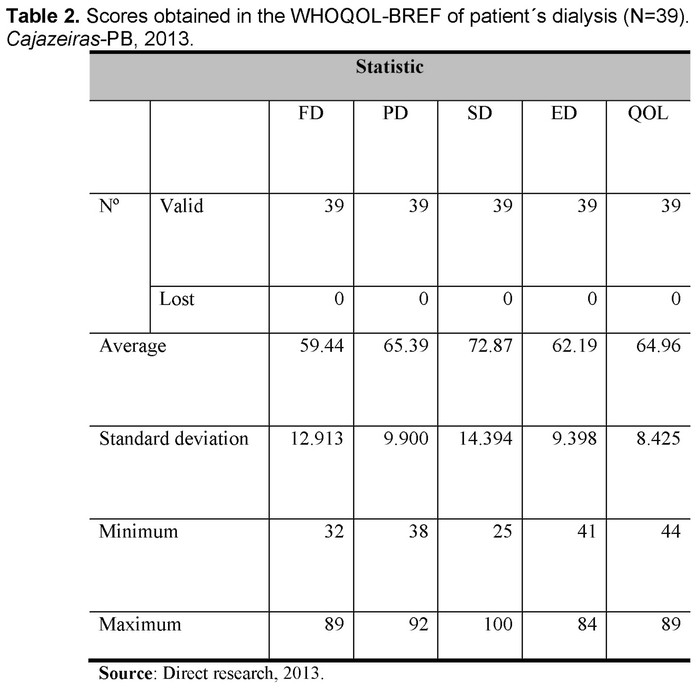
It is possible to analyze in the table above, the results that are obtained through the domains and QOL addressed in general, in the WHOQOL-BREF collection instrument of this study. In a comprehensive way, the most affected domain among participants was the physical (FD) with an average of 59.44 and the most preserved the social domain (SD) with an average of 72.87. However, the other domains, both psychological (PD) and environmental (ED) also presented low averages, reflecting on the QOL of patients with CKD, who had an average of 64.96.
The commitment in the FD reflects the overview of a chronic disease, where treatment creates pain and discomfort, as well as dependence on medication and renal replacement therapy; creates fatigue, decreased the patient's mobility, since they need to connect to a machine during several days a week, it affects the sleep and rest, in the activity of everyday life and work capacity.
Environmental conditions was also a domain with a low average, showing that patients with CKD undergoing dialysis, have difficulties in acquiring new skills, job opportunities, recreation, and leisure, maybe, to be transported from one place to another.
Thus, it is concluded that the physical limitations caused by the disease, as well as the environmental conditions in which they live, are the most aggravating factors for the quality of life of patients with CKD, detected by this study. Leading us to believe that, over time, patients undergoing dialysis can overcome imposed psychological challenges, as well as seeks and relies on greater social support for coping the disease and its treatment.
A good feature of the studied group was the best average in social relations, showing that despite the disease and treatment, the CKD carriers maintain a good personal relationship and sexual activity and social support. Regarding QOL, the study obtained an average of 64.96, a value that does not characterize a bad quality of life, but at the same time, does not match a good QOL, but regular.
Table 3 it is a correlation between domains and QOL. The Person Correlation test was used between the variables, which results showed a significant relationship between the various domains, in which all showed a high correlation with QOL.
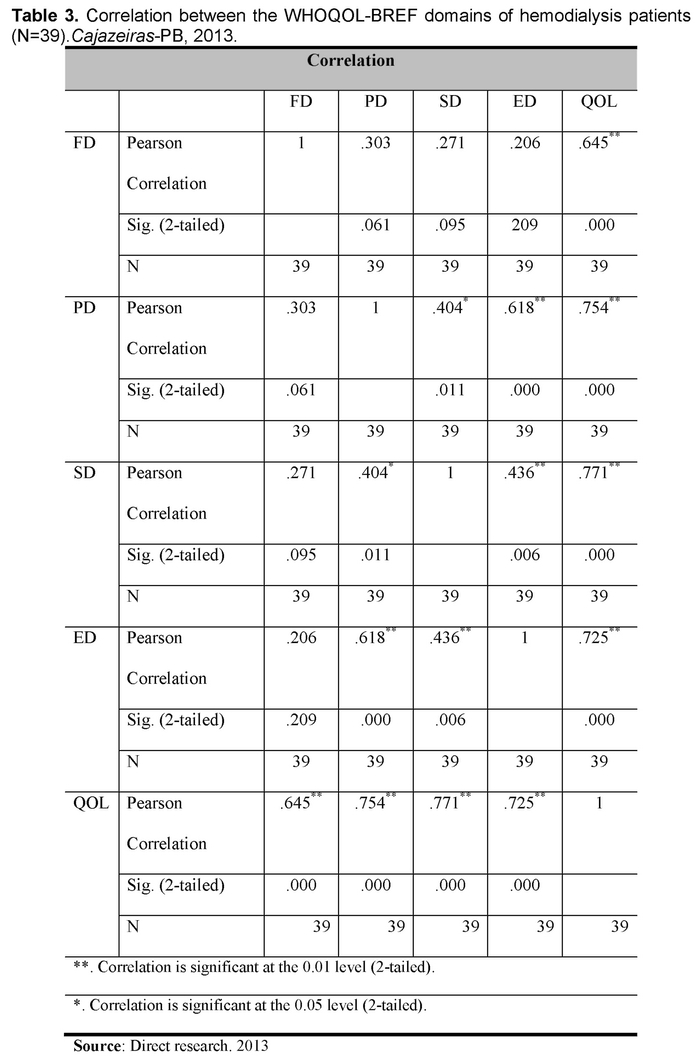
Referring only to the domains, it was possible to analyze that FD, in contradiction to the literature, in this case, did not possess correlation with other particular domains, only significantly and interfered in QOL.
Chronic condition and dialysis treatment are sources of stress, which leads to cause many problems such as social isolation, loss of employment, social security dependency, partial failure of locomotion and tours, decreased physical activity, need to adapt to the loss of autonomy, body image changes, and also an ambiguous feeling of fear live and die (3).
Regarding other domains, it was observed that the PD and SD have a small correlation between each other, but when it comes to the ED, both have strong influence, which suggests that social relations, support of family and friends, financial issues and the environment where these patients live, cause a change in the individual psychological, that because the living conditions are unique and different for each person.
Discussion
It is known that, with advancing age, the regulatory functions of the body gradually decrease, which shows the onset of chronic diseases in this stage of life. It is possible to analyze that the CKD index affects more men than women, suggesting a decrease about health care by this gender, damaging the process of prevention and early diagnosis of diseases.
The increase in cases of kidney disease is mainly due to aggravating pathologies and the increase in population life expectancy since over the years the body tends to lose gradually its regulatory functions(9).
In a study conducted in 2009, there are finding that the interviewee that had a steady partner had a better average about the physical dimension, compared to those who did not have a steady partner, indicating that the ability to perform daily activities become easier with help and support from the partner(10).
It is important to note that, in general, the higher the level of study more information that patients have about their medical condition and ways to maintain a healthy life.
Self-care can be considered a practice of regulatory functions that individuals develop to maintain a healthy lifestyle, which does not involve risks to vital functions. Thus, they collaborate intensively with the quality of life, since the proper health care prevents or reduces medical procedures. Therefore, it is believed that knowledge is a tool of great importance and influences self-help skills of the individual(11).
The adaption to the CKD features, knowing that it has no cure and treatment is highly complex, also means the adaption to the numerous changes in quality of life, due to various symptoms in the course of the disease. Some of them cause different levels of physical limitation and working conditions, constituting a problem of social and economic health(12).
The social life and family relations are of great importance in the hemodialysis treatment, as the disease influences and generates physical, social, psychological and emotional changes that often lead to the isolation of the patient and clinical depression.
There are differences in the dimensions of physical functioning, effects of the disease and also sexual function, being the variables lower for people living alone, which indicate a worse thereof. Therefore, it is worth mentioning the importance of family support in QOL and its collaborator role with health care in CKD carrier undergoing dialysis treatment(10).
The impact caused by dialysis time is little known, however, in its studies, it was found that patients with increased treatment time showed better score as the functional capacity domains, physical, vitality, emotional aspects and social aspects(13).
The CKD leads to patients, various physical characters, and environmental conditions changes where they live, trigger psychological and social changes, being directly linked to their quality of life evaluation. Concerning that perception of quality of life is unique for each participant, it can be a positive character, in which the patient seeks understanding about the disease and better-coping measures; as well as negative, which a denial feeling about the disease(14).
The restrictions caused by dialysis can significantly change the QOL of CKD patients since the physical signs and symptoms of the disease cause changes in lifestyle, and the ability to work awakening depressive conditions related to the disease(15).
Changes in physical patterns may be related mainly to the fatigue factor and signs of musculoskeletal deterioration and physical weakness due to dialysis action, which triggers other symptoms such as negative, depressive or irritating feelings(15).
The need to continuously perform dialysis contributes to dependence on medical treatment, including the FD, and work and studies interfere, resulting in lack.
In the analyzed PD, a study performed in Minas Gerais/Brazil shows that the results are similar. The situation of the QOL of interviewed patients was neither bad nor good, as it goes against the result of the average obtained in this study, considering that in the evaluation, the closer to 100%, the better the result. They took into consideration that in the social relations, patients had a score between good and very good, meeting the average obtained in this study compared to the SD(16).
On the other hand, another study shows that the social fact is one of the most affected; by often take the patient to the removal of social relationships(17).
Concerning QOL, various aspects such as physical, psychological, social, including the level of satisfaction of each one and the importance to live, as well as the ability to perform activities, contribute to good or excellent QOL(2).
It is noteworthy and necessary to observe that the dialysis treatment time interferes with dimensions of physical functioning, energy, and fatigue because they modify the ability to perform daily activities. However, the time spent in the dialysis induces the patient to seek ways to deal with the domain changes over the time, which is a favorable factor to a better quality of life(10).
Therefore, since the domains are correlated, the quality of life depends directly on at least a minimum of good conditions in each one, so the individual can lead to the life without major losses in the living habits after the discovery of disease and early dialysis treatment.
Nursing is mainly focused on patient's assistance and care, beyond the technical procedures and requires the establishment of customer-professional relationship to understand the greater needs of the patient to ensure a humanized work, worried with the cared being(18).
Concerning specifically the clinical dialysis sector, this requires a specialized nursing care, mainly for maintenance of customer's quality of life. Thus, we can highlight the importance of nursing professionals in this sector about the provided care, as well as and the quality of care and education of chronic kidney patients, to achieve a qualified attendance in the service, considering the high level of complexity and undergoing dialysis treatment addiction(18).
Conclusion
This study enables to know the QOL of CKD patients undergoing dialysis treatment in the city of Cajazeiras, Paraíba state; aiming to characterize their socio-demographic variables and through the WHOQOL-BREF instrument, to investigate the factors that interfere with daily activities and influence their QOL.
The CKD is an incurable and continued progression disease that has dialysis as a treatment, which is a modality that requires discipline and also brings on several changes in the physical, psychological, social and environmental context, which influence the quality of life of patients.
It is important to note that even with these changes, dialysis is seen as a synonym of maintenance of life, as it carries one of the vital functions that are the blood filtration system, that without it, the toxic waste would not be removed and improper for the body.
It was observed that concerning to FD, this was the most affected in terms of evaluation, concluding that the limitations imposed by treatment led patients to restrictions regarding work, and to perform routine physical activities as well as the displacement need to ensure treatment, since there is a dependency as a guarantee of life, thus becoming a stressful factor for the patient.
Between PD and SD, it was noted that they were not such affected during the assessment, leading to the belief that patients have a high degree of acceptance regarding the treatment, also emphasizing that they strongly believe in this with hope, because they are plenty aware that it is the only way to continue to live. Still in question, it was clear that the CKD carriers have satisfactory social relations, thus obtaining the necessary support for coping the disease as well as contributing to the reduction of negative feelings and impotence within the social environment.
The ED also has a low average, and it was concluded that there is security, comfort, leisure opportunity, financial resources, transportation and deficit among others, affecting the quality of life of patients undergoing dialysis treatment. It is appropriate to analyze that the satisfaction with transport is fundamental to the locomotion to the dialysis center.
It was possible to analyze that exists, between most of the population, a dissatisfaction with the working capacity, a decrease in income that limits them to maintain the same standard of life before the disease; the restrictions and the sharp decrease in leisure and tour activities. It was also observed satisfaction with social and family relationships, did not feel harmed with the health service of the dialysis center, and some even with treatment modality, maintaining a hope that life can continue, even if effort and the restrictions would be necessary. The search for QOL involves goodwill and means a constant struggle between the limits imposed by the disease and its treatment modality, and seeks control of feelings. Hence the importance of social and family support.
In general, CKD patients undergoing dialysis treatment have a regular quality of life. It is important to note that even with all changes in the course of the disease, the target population of this study showed that, despite the restrictions and changes in living habits, it is important to continue and overcome difficulties, aiming at a better QOL, i.e., live well, although the elimination of signs and symptoms would be unlikely.
As a suggestion, it is necessary that health professionals increasingly seek to inform patients about the disease, the individual conditions, the limits imposed by treatment modality and know the needs, desires and fears; aiming at clarifying, encouraging learning, so that the target audience in question, can know the importance of treatment continuity, and develop better self-care and better QOL.
Finally, this study was, therefore, of great importance because it offers subsidies for the team responsible for dialysis to realize the need and importance of evaluating the quality of life for dialysis patients and provide them optimization means on this treatment modality.
It is expected to contribute to future studies, considering that work quality of life is complex but of great importance in promoting the welfare of the CKD patients undergoing edialysis treatment.
Received: December 4, 2014
Aceppted: March 5, 2015
Referênces
1. Martins MRI, Cesarino CB. Qualidade de Vida de Pessoas com Doença Renal Crônica em Tratamento Hemodialítico. Rev Latino-am Enfermagem, 2005 (citado 2014 Nov 12); 13(5): (06 telas). Disponível em: http://bvsms.saude.gov.br/bvs/isdigital/is 0106/pdfs/IS26%281%29017.pdf. [ Links ]
2. Bezerra KV. Estudo do Cotidiano e Qualidade de Vida de Pessoas com Insuficiência Renal Crônica (IRC), em Hemodiálise (dissertação). Ribeirão Preto: Universidade de São Paulo, Faculdade de Medicina de Ribeirão Preto; 2006. [ Links ]
3. Machado LRC, Car MR. A Dialética da Vida Cotidiana de Doentes com Insuficiência Renal Crônica: entre o inevitável e o casual. Rev Esc Enferm USP, 2003 (citado 2014 Nov 12); 37(3): (09 telas). Disponível em: http://www.scielo.br/pdf/reeusp/v37n3/04.pdf. [ Links ]
4. Guedes KD, Guedes HM. Qualidade de Vida do Paciente Portador de Insuficiência Renal Crônica. Revista Ciência & Saúde, Porto Alegre, 2012 (citado 2014 Nov 13); 5(1): (06 telas). Disponível em: http://revistaseletronicas.pucrs.br/ojs/index.php/faenfi/article/view/9734/7746. [ Links ]
5. Pennafort VPS, Furtado AM, Fialho AVM, et al. Produção do Conhecimento Científico de Enfermagem em Nefrologia. Rev. bras. enferm, 2010 (citado 2014 Nov 12); 63(5): (07 telas). Disponível em: http://www.scielo.br/pdf/reben/v63n5/22.pdf. [ Links ]
6. Pereira MG. Epidemiologia: teoria e prática. 12a edition. Rio de Janeiro: Guanabara Koogan, 2008. [ Links ]
7. Whoqol G. Whoqol-Bref. (Acesso em 12 Nov 2014). Disponível em: http://www.ufrgs.br/psiquiatria/psiq/WHOQOL-OLD Manual POrtugues.pdf. [ Links ]
8. Sociedade Brasileira de Nefrologia. Censo de Diálise. 2011 (acesso em 13 Nov 2014). Disponível em: http://www.sbn.org.br/. [ Links ]
9. Salgado Filho N, Brito DJA. Doença Renal Crônica: a grande epidemia deste milênio. J Bras Nefrol, 2006 (citado 2014 Nov 13); 28(3): (05 telas). Disponivel em: http://www.jbn.org.br/detalhesuplemento.asp?id=1553. [ Links ]
10. Cordeiro JABL, Brasil VV, Silva AMTC, et al. Qualidade de vida e tratamento hemodialítico: avaliação do portador de insuficiência renal crônica. Rev. Eletr. Enf, 2009 (citado 2014 Nov 12);11(4): (09 telas). Disponível em: http://www.fen.ufg.br/fenrevista/v11/n4/pdf/v11n4a03.pdf. [ Links ]
11. Baquedano IR, Santos MA, Teixeira CRS, et al. Fatores relacionados ao autocuidado de pessoas com diabetes mellitus atendidas em Serviço de Urgência no México. Rev. esc. enferm. USP, 2010 (citado 2014 Nov 10); 44(4): (07 telas). Disponível em: http://www.scielo.br/pdf/reeusp/v44n4/23.pdf. [ Links ]
12. Rudnicki T. Preditores de Qualidade de Vida em Pacientes Renais Crônicos. Estud. psicol. (Campinas), 2007 (citado 2014 Nov 12); 24(3): (10 telas). Disponível em: http://www.scielo.br/pdf/estpsi/v24n3/a06v24n3.pdf. [ Links ]
13. Silveira CB, Pantoja IKOR, Silva ARM, et al. Qualidade de Vida de Pacientes em Hemodiálise em um Hospital Público de Belém - Pará. J. Bras. Nefrol, 2010 (citado 2014 Nov 11); 32(1): (06 telas). Disponível em: http://www.scielo.br/pdf/jbn/v32n1/v32n1a08.pdf. [ Links ]
14. Higa K, et al. Qualidade de Vida de Pacientes Portadores de Insuficiencia Renal Crônica em Tratamento de Hemodilise. Acta Paul Enferm, 2008 (citado 2014 Nov 13); 21(Número especial): (04 telas). Disponível em: http://www.scielo.br/pdf/ape/v21nspe/a12v21ns. [ Links ]
15. Tretini M, Corradi EM, Araldi MAR, Tigrinho FC. Qualidade de Vida de Pessoas Dependentes de Hemodiálise Considerando Alguns Aspectos Físicos, Sociais e Emocionais. Texto & Contexto Enfermagem, 2004 (citado 2014 Nov 15); 13(1): (10 telas). Disponível em: http://www.redalyc.org/pdf/714/71413111.pdf. [ Links ]
16. Terra FS, Costa AMDD. Avaliação da Qualidade de Vida de Pacientes Renais Crônicos Submetidos à Hemodiálise. R Enferm. UERJ, Rio de Janeiro, 2007 (citado 2014 Nov 10); 15(3): (07 telas). Disponível em: http://www.facenf.uerj.br/v15n3/v15n3a18.pdf. [ Links ]
17. Meireles VC, Goes HLF, Dias TA. Vivências Do Paciente Renal Crônico Em Tratamento Hemodialítico: Subsídios Para O Profissional Enfermeiro. Ciência, Cuidado e Saúde, Maringá, 2004 (citado 2014 Nov 12); 3(2): (10 telas). Disponível em: http://www.periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/view/5423/3475. [ Links ]
18. Rodrigues TA, Botti NCL. Cuidar e o Ser Cuidado na Hemodiálise. Acta Paul Enferm. 2009 (citado 2014 Nov 12); 22 (Especial-Nefrologia): (03 telas). Disponível em: http://www.scielo.br/pdf/ape/v22nspe1/15.pdf. [ Links ]

