










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.16 n.46 Murcia Apr. 2017 Epub Apr 01, 2017
https://dx.doi.org/10.6018/eglobal.16.2.249241
Originales
Quality of life and self-reported morbidity of productively active women
1Master in Nursing. University of Guarulhos. Brazil.
2Obstetrician. Doctor of Nursing. Professor of the Master's Program in Nursing. University of Guarulhos. Brazil.
Introduction
Self-reported morbidity, lifestyle and quality of life is a triad that seems to be aligned and has been little explored in the context of women’s life. The study aimed to: check the quality of life index of productively active women’s and associate the quality of life index with self- reported morbidity and lifestyle.
Methods
This was a cross-sectional analytical field study of a quantitative approach, with 121 women participating. WHOQOL- BREF was utilized to measure the quality of life.
Results
The quality of life General Index was 63.7.The domain with the worst average was the environmental (54.6). There was a statistically significant difference (p=0.035) when comparing women who reported health problems and those who did not and among women who feel pain or not (p=0.001) in the physical domain and quality of life General Index (p=0,003). In the comparative analysis of the quality of life index and lifestyle there is no statistically significant difference in this sample.
Conclusion
It was concluded that health problems and feel pain had negative influence in the quality of life index of these women.
Keywords Quality of Life; Women; Morbidity
INTRODUCTION
In recent decades, Quality of Life (QoL) has been the subject of debate and research in different areas of knowledge, including health. Improvements in the conditions of health and life, in general, depend on many factors, among them preventive measures, health promotion and concern for the quality of life of people and the community (1). Conditions of life affect health, which strongly influences the perception of quality of life (2).
The perception of people regarding their health is important regardless of whether they have a disease or not. The feeling of well-being transcends the presence of problems, although it presents well established relationships with clinical conditions and morbidity and mortality indicators (3).
The self-reported morbidity of chronic diseases has been evaluated as a good measure of health, as it comes close to the information obtained through clinical tests(3). That is, self-reported disease information has shown good agreement with medical records or clinical examinations.
Self-perceived morbidity is one of the health condition indicators used to identify the demands for services, as well as to evaluate health policies and assist in new proposals in public health (4). Health conditions are influenced by lifestyle and living habits that, in turn, influence the well-being of people and consequently their QoL. Food consumption, physical activity, smoking, work and the socioeconomic conditions of individuals determine their health profile (4). Therefore, a network of social interaction and support, healthy eating and physical activity should be systematized and encouraged to promote health (3).
Morbidity, health habits and QoL is a triad that seems to be well aligned. However, studies that relate these elements have mostly been developed with older adults. Research carried out exclusively with females and the productively active population is scarce, hence the motivation for this study, which aimed to verify the quality of life index of women of a private health institution and associate the quality of life index with the morbidity and living habits reported.
METHOD
This was a cross-sectional, analytical, quantitative field study, conducted in a large hospital in São Paulo. The institution was chosen due to ease of access to the women for the researcher. It should be noted that the focus of the study was not QoL at work, but the general QoL of healthy productive women. The institution had 5,259 employees, 3,179 of whom were female.
To calculate the sample size, a total of 3,035 employees present in the institution at the time of the study were considered. The formula used was: n= [1/(d2/z2*s2)+(1/N)], in which d=margin error, z=z score of the normal curve for the desired alpha error, s=standard deviation and n=population size (for finite populations). A confidence level of 95%, margin of error ± 3 and standard deviation of 17 were considered. The estimated size for the sample was 121 women (N=121).
Sampling was carried out in a simple random way and the site randomized.com was used to draw the participants. In the sample the following inclusion criteria were considered: to be drawn for the sample; to be available to answer the QoL instrument; to be aged ≥18 years; to be literate; and to be present in the institution at the time of data collection. Data were collected between July and September 2014 and the participants were individually interviewed in the sector in which they worked.
Two instruments were used for the data collection. A questionnaire was used to collect the sociodemographic (age, marital status, education, ethnicity, number of children and religion), reported morbidity, life habits (regular consultations with the gynecologist, smoking, alcohol consumption and physical exercise) and pain evaluation data. Quality of life was measured by applying the shortened version of the World Health Organization Quality of Life Index (WHOQOL-BREF).
The WHOQOL-BREF has been used in many countries and applied with different groups of people and has demonstrated its applicability from an international and cross-cultural perspective. This instrument is self-administered and consists of 26 items. It assesses five domains of quality of life: physical, psychological, social relationships, environment and general (5). Responses to the WHOQOL-BREF items are given on a Likert type scale ranging from 1 to 5. Items 3 and 4 of the physical domain and item 26 of the psychological domain should have the response scale inverted. The domain scores are calculated through the mean score of the items that comprise each domain. The result is multiplied by 4, with a range of 4 to 20. The domain scores are converted to a scale of 0 to 100 (6), with higher scores representing better QoL.
To compare the scores with the qualitative variables, Student’s t-test was used to compare two means and Analysis of Variance (ANOVA) to compare more than two means. In the case of ANOVA, for the variables that represented significant test values (p <0.05), an analysis of multiple comparisons was made, using the Bonferroni method. Results in which p<0.05 were considered statistically significant. Internal consistency analysis was also performed for the index of total quality, through Cronbach’s alpha, which was satisfactory (0.8001).
This study was approved by the Research Ethics Committee of Guarulhos University (Authorization No. 696.003) and fulfilled the ethical requirements of Resolution 466/12 of the National Health Council.
RESULTS
In this study, 3,035 women of the institution were eligible for inclusion in the sample of 121 participants, with none of those draw refusing to participate. The profile of the participants can be described as follows: mean age 34.2 years (SD±8.2) with a minimum of 19 and maximum of 57 years. The majority (n=63; 52.1%) were married, of the white ethnic group (n=89; 73.6%) and from the state of São Paulo (n=96; 79.3%), 60 (49.6%) had no children and the predominant religion was Catholic (n=53; 43.8%). The majority (n=61; 50.5%) had complete higher education.
Of all the women (n= 121) that participated in the study, 59 (48.8%) reported a current or previous health problem, in (Table 1) the total was 74 because one woman may have reported more than one morbidity. The morbidities most mentioned were those of the musculoskeletal system (n=13; 17.3%), neoplasms (n=13; 17.3%), digestive system (n=10; 13.3%) and respiratory system (n=8; 10.7%).
Table 1 Morbidities reported by the women (n=74), São Paulo, 2014
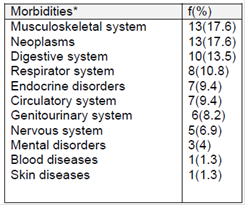
*More than one morbidity could be reported by each woman.
The health problems of the musculoskeletal system most frequently cited were: tendinitis in the hip (n=2; 15.3%), bursitis (n=1; 7.7%), Sjögren’s syndrome (n=1; 7.7%) tendonitis (n=4; 30.6%), rheumatoid arthritis (n=1, 7.7%), ankylosing spondylitis (n=1; 7.7%) and herniated disc (n=3; 23.3 %). The neoplasms most cited by the women were breast cancer (n=6; 46.6%), ovarian cancer (n=2; 15.3%) and thyroid cancer (n=3; 23.3%). The majority of the women (n=65; 53.7%) received medication and, of those taking some kind of medication, the majority (n=60; 92.3%) had a medical prescription. In relation to pain, 60 women mentioned this, i.e. 49.6% of the sample suffered from some type of pain. In the assessment of pain intensity (scale from 0 to 10) the mean was 5.6, the median score was 5, with this being 4 in the 25th percentile and 7in the 75th, indicating pain of moderate intensity (7).
The morbidities of the digestive system most reported were: gastritis (n=3; 30%), cholelithiasis (n=3; 30%) and related to the respiratory system: bronchitis (n=2; 25%) and asthma (n=2, 25%).
With regard to the life habits and health, the majority, 103 (85.1%), had undergone monitoring with a gynecologist in the previous year, 93 (76.9%) performed an annual cervical cancer detection examination and 86 (71, 1%) a breast cancer examination.
Performing physical activity was mentioned by 42 women (34.7%). Of those that were not sedentary, 19 (45.2%) practiced activities 3 times a week and 33.3% (n=14) 4 times or more.
The majority, 76 (62.8%), reported not consuming alcohol, and of those who mentioned this habit 75.6% (n=34) consumed it only once a week. Regarding smoking, 95.5% (n=116) did not have this habit. Of the smokers (n=5, 4.1%), 60% (n=3) consumed more than 5 cigarettes per day.
It can be observed in (Table 2) that the highest mean of the quality of life scores was in the Social domain (68.3) and the lowest in the Environment domain (54.6). The General QoL mean was 63.7 (SD ± 64.4).

(Table 3) shows that in the physical domain the women who reported health problems presented lower mean QoL scores. There was a statistically significant difference in this domain (p=0.035) in the comparison between those with and those without health problem and a statistical trend (p=0.056) in the psychological domain.
Table 3 Comparison of the quality of life indices according to reported health problem (n=121). São Paulo, 2014
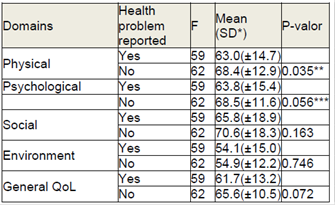
*SD = standard deviation **statistically significant (p<0.05) ***statistical tendency (p≈0.05)
Comparing the quality of life indices and the presence of pain in the women, both the physical domain and the general QoL of the women who reported feeling pain (n=60; 49.6%) presented lower mean scores (59.6; SD ± 14.4) (60.5; SD ± 11.8). There was a statistically significant difference in these domains between the women who felt pain and those that did not (p=0.001), i.e., pain interfered in the QoL of the women.
The association of the QoL index with living habits showed a statistically significant difference only in relation to smoking in the social domain (p=0.04). Smokers (n=5; 4.1%) presented higher quality of life scores in the social domain compared to the non-smokers (85.5; SD±10.9) (67.6; SD±18.6).
DISCUSSION
The knowledge produced by this study is important due to it being a gender study. Studies of QoL directed only toward women are scarce. Knowing the perception of women about their morbidities and lifestyle habits can contribute to the establishment of health policies aimed at improving the living conditions of this portion of the population.
The works cited in this discussion from the literature on QoL were not performed exclusively with women, as in this study; however, in many of the studies the participants were predominantly female and productively active, allowing the data to be used for comparisons (8)(28).
In this study, the mean age of the participants was found to be between the third and fourth decade of life (34.2 years), featuring a young group, similar to other studies (8)(11) in which the majority of participants were women aged between the third and fourth decade of life. This may explain the lack of references to the morbidities of hypertension and diabetes mellitus.
The majority of the women (73.6%) were white, data similar to those disclosed by public agencies that highlight the white ethnicity as 61.9% of the population of São Paulo (12). Another finding relates to the religion declared by the women, most of whom (77.7%) reported being christian, with 53 (43.8%) reporting catholic and 41 (33.9%) evangelical religions. these data are consistent with those presented by the brazilian population, according to the ibge (13) that indicates the majority of brazilians (86.8%) as catholics and evangelicals.
The study identified that 85.1% of the women reported annual monitoring by a gynecologist. the findings related to the gynecologic cancer screening tests are consistent with those presented by the ministry of health in 2013 (14) that showed 82.9% of women performed a pap smear and 78% a mammography.
AN IMPORTANT ASPECT EVALUATED IN THIS STUDY WAS THE MORBIDITY REPORTED BY THE WOMEN. THE STUDY OF SELF-REPORTED MORBIDITY IS CONSIDERED IMPORTANT BECAUSE THE INFORMATION GIVEN BY THE INDIVIDUAL COMES CLOSE TO THAT OBTAINED BY CLINICAL EXAMINATIONS (3).
In the current study almost half the sample (48.8%) reported some type of health problem, among them, diseases of the musculoskeletal system and cancer stood out, each reported by 17.3% of the participants. Diseases of the digestive system were cited by 13.5% and those of the respiratory and circulatory system were cited by 10.8% and 9.4% of participants, respectively.
These findings are in agreement with other studies, one of which involved the employees of the hygiene service of a hospital in são josé dos campos (15), in which the majority (87.88%) of the participants were female and 54.54% of the women indicated some health problem. as in the present study, musculoskeletal diseases (63.33%), those related to the circulatory system (20%) and digestive system (6.67%) were highlighted. in another study performed with dentists in Goiania (11) musculoskeletal problems (17.8%) and hypertension (8.9%) were the diseases most mentioned.
In a study involving workers at a state hospital in Minas Gerais (16) 70% of the participants reported morbidities, predominantly related to the musculoskeletal (11.83%) respiratory (10.83%) and circulatory (8.62%) systems.
Modernity causes people to behave in ways that affect qol, such as unhealthy eating habits, physical inactivity, stress and habits that act as a source of pleasure, such as drinking and smoking, which can affect the body and cause diseases (17). In this study the majority of women (65.3%) reported not practicing physical activity, an aspect that can compromise the qol.
A study performed with teachers of Bagé in Rio Grande do Sul (18) highlighted the importance of the lifestyle on the perception of health conditions among this population, evidencing better health perception indices among those who had healthier lifestyles, including physical exercise, balanced diet, control of body weight and control of the use of substances such as alcohol and tobacco.
A healthy lifestyle has been associated with the systematic realization of bodily activities and a positive relationship has been established between physical activity and better qol, therefore, the habit of practicing physical activity is a determining factor for the improvement of health patterns and quality of life (5).
The most important finding of this study, which also responds to one of its aims, was measuring the QoL index of the participants. The mean general QoL of the women was 63.7, median 64.4, standard deviation (SD) ± 12, indicating a generally good quality of life, if considering the classification Castro and Fracolli (2), which classifies very good QoL when the mean score is above 81, good 61 to 80, neither good nor bad between 41 and 60, poor between 21 and 40 and very poor for scores lower than 20. The results are similar to another study with anesthesiologists from Recife (19), which showed a mean score of 65.02, indicating that these professionals had a good QoL.
The measurement of QoL allows individuals to reflect on their behavior and habits and stimulates them to seek a balance of activities (20). The analysis of the QoL of the participants, by domains, highlighted the environment domain as having the lowest score. The mean was 54.6, median 56.3 (SD ± 13.6), classifying this QoL domain as neither bad nor good. These results may be related to the city where the participants lived. São Paulo is today one of the largest urban centers and its inhabitants live with issues such as violence, displacement and problems of transport, pollution and sanitation, among others. Added to this, the economic and population growth have generated an ecological imbalance and the degradation of the physical and social environments, factors that may affect the QoL and may have affected the results in this domain (21).
The perception of Qol of the women in the physical domain indicated a mean of 65.8, median 67.9 (sd ± 14), indicative of a good quality of life in this domain. This finding is similar to data of some studies found in the literature (9), (11), (19), (22), (23), in which the mean scores for this domain ranged between 63.7 and 77.2. However, intensive care unit nursing professionals (24), teaching hospital nurses (10) and pregnant women (2) presented lower means in this domain, 53.1, 42.6 and 57.6, respectively, compatible with a Qol neither good nor bad.
In the psychological domain, the mean qol index found was 66.2, median 66.7 (sd ± 13.8). in this domain other studies, despite the results being within the same Qol assessment limit, i.e. good, found a slightly higher mean, such as with teachers of Florianopolis (25) and pregnant women (2), which showed means of 68.6 and 68.7, respectively. Some other studies found even higher means in this domain, such as those developed with community health workers (23), operating room professionals (9) and dentists of Goiânia (11), with scores of 74.3, 72.0 and 69.7, respectively. However, a study with nurses of a teaching hospital showed a mean of 44.0 (10), indicating this quality of life domain as neither good nor bad.
The highest Qol index observed was in the social domain (68.3). This finding is similar to that of studies carried out in several states (9), (11), (20), (22), (24), (25), which showed means of 71.4, 69.4, 63.7, 67.8 and 73.1, respectively.
Acute or chronic health problems seem to affect the QoL of people. In the comparison of the QoL indices of the participants a statistically significant difference was seen between those with and those without a health problem in the physical domain (p=0.035) and a statistical trend (p=0.056) in the psychological domain.
Studies aiming to determine the relationship between QoL and morbidity have identified that disease interferes with QoL. In one study developed with dentists (11) the QoL index was lower among those who reported health problems, with the same occurring with medical students (22), in which lower QoL rates were identified among those that reported health problems, with special attention to the fact that these students were young, with a mean age of 23 years.
The presence of pain reported by the women had a negative impact on the general QoL and on the physical and social domains. A study performed with community health workers (23) showed a statistically significant difference (p<0.001) in the physical domain for those who reported musculoskeletal pain.
Many health professionals suffer from lowered QoL because of chronic pain from musculoskeletal problems. This is usually due to repetitive actions and improper posture in the execution of work activities, with an overload of the spine. A study with patients suffering with chronic low back pain (26) highlighted a low mean QoL (44.1), demonstrating the disability caused by pain and its negative impact and important influence on the QoL of these individuals.
Regarding alcohol, there was a statistical trend (p=0.70) in the physical domain, showing that those who consume this have the potential for worse QoL. A study that examined the QoL of adolescents demonstrated a worse QoL with alcohol dependence, more pronounced in females (27).
Smoking only showed a statistically significant difference in the social domain (p=0.040), demonstrating, in this study, that in women smokers the QoL was better. This result may be linked to the fact that cigarettes help people cope with social situations they consider difficult.
The results found in the study differed from studies that relate QoL and smoking that, according to Castro et al. (28), show worse QoL for smokers. A study of community health workers (23) also showed a statistically significant difference (p=0.008) in the physical domain for those who reported smoking, indicating greater impairment of QoL, that is a negative influence from their perception.
CONCLUSIONS
The General QoL of the women that composed the sample can be considered good. The mean QoL scores, by domain, can also be evaluated as good, with the exception of the environment domain that showed a mean compatible with a QoL neither bad nor good.
Morbidity and pain impacted negatively on the QoL of the women. Diseases impaired the QoL in the physical domain and tended to influence the psychological domain, while pain impacted negatively on the general QoL and physical and social domains.
The performance of further studies is recommended to measure the QoL of healthy women to make comparisons and confirm these results.
REFERENCIAS
1. Buss PM. Promoção da Saúde e qualidade de vida. Ciênc Saúde Coletiva [online]. 2000; [acesso em 2014 maio 11];5(1):163-77. Disponível em: http://www.scielo.br/pdf/csc/v5n1/7075.pdf [ Links ]
2. Castro DFA, Fracolli LA. Qualidade de vida e promoção da saúde: em foco as gestantes. Mundo da Saúde [online]. 2013; [acesso em 2014 maio 10];37(2):159-65. Disponível em: http://www.saocamilo-sp.br/pdf/mundo_saude/102/4.pdf [ Links ]
3. Theme Filha MM, Szwarcwald CL, Junior PRBS. Measurements of reported morbidity and interelationships with health dimensions. Rev Saúde Pública [online]. 2008 feb; [acesso em 2014 maio 1];42(1):73-81.Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=s0034-89102008000100010 [ Links ]
4. Iozzi R, Caetano S, Carneiro AC, Theme MM, Reis V, Santos LH. Morbidade referida - 1ª pesquisa sobre condições de saúde e vida de idosos da cidade do Rio de Janeiro. Trabalho apresentado no XVI Encontro Nacional de Estudos Populacionais; 29 de setembro a 03 de outubro de 2008; Caxambú - MG - Brasil. [ Links ]
5. Fleck MPA, Leal OF, Louzada S, Xavier M, Cachamovich E, Vieira G, et al. Desenvolvimento da versão em português do instrumento de avaliação de qualidade de vida da OMS (WHOQOL-100). Rev Bras Psiquiatr [online]. 1999; [acesso em Set 15];21(1):21-8. Disponível em: http://www.scielo.br/pdf/rbp/v21n1/v21n1a06.pdf [ Links ]
6. Pedroso B, Pilatti LA, Gutierrez GL, Picinin CT. Cálculo dos escores e estatística descritiva do WHOQOL-bref através do Microsoft Excel. R Bras Qual Vida [online]. 2010; [acesso 2015 set 10];2(1):31-6. Disponível em: https://periodicos.utfpr.edu.br/rbqv/article/view/687 [ Links ]
7. Kimberly MJ, Lewthwaite BJ, Mandzuk LL, Schnell-Hoehn KN, Wheeler BJ. The pain experience of inpatients in a teaching hospital: Revisiting a strategic priority. Pain Management Nursing. 2015;16(1):69-76. [ Links ]
8. Conceição MR, Costa MS, Almeida MI, Souza AMA, Cavalcante MBPT, Alves MDS. Qualidade de vida do enfermeiro no trabalho docente: estudo com o WHOQOL-Bref. Esc Anna Nery [online]. 2012 abr/jun; [acesso em 2014 ago 3];16(2):320-5. Disponível em: http://www.scielo.br/pdf/ean/v16n2/16.pdf [ Links ]
9. Stumm F, Miladi E, Nogueira GM, Kirchner RM, Guido LA, Ubessi LD. Qualidade de vida de profissionais em um centro cirúrgico. Enferm Glob [internet]. 2013 abr; [acesso em 2014 set 13];12(30):220-231. Disponível em: http://scielo.isciii.es/pdf/eg/v12n30/pt_administracion2.pdf [ Links ]
10. Lima EFA, Borges JV, Oliveira ERA, Velten APC, Primo CC, Leite FMC. Qualidade de vida no trabalho de enfermeiros de um hospital universitário. Rev Eletr Enf [internet]. 2013 out/dez; [acesso 2014 set 13];15(4):1000-6. Disponível em: https://www.fen.ufg.br/fen_revista/v15/n4/pdf/v15n4a18.pdf [ Links ]
11. Nunes MF, Freire MCM. Qualidade de vida de cirurgiões-dentistas que atuam em um serviço público. Rev de Saúde Pública [internet]. 2006 dez; [acesso em 2014 ago 15];40(6):1019-26. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-89102006000700009 [ Links ]
12. Secretaria Municipal de Saúde. Coordenação de epidemiologia e informação (CEInfo) [internet]. Boletim ISA - Capital 2008: Inquérito de Saúde - primeiros resultados. nº 1. São Paulo - Capital. 2010. Consultado em 01.02.2015. [ Links ]
13. Instituto Brasileiro de Geografia e Estatística (IBGE) [internet]. São Paulo. 2010. Consultado em 01.02.2015. Disponível em: http://www.sidra.ibge.gov.br/bda/popul/default.asp?t=3&z=t&o=25&u1=1&u2=1&u3=1&u4=1&u5=1&u6=1 [ Links ]
14. Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico (VIGITEL 2013). Consultado 01.03.2015. Disponível em: http://portalsaude.saude.gov.br/images/pdf/2014/abril/30/Lancamento-Vigitel-28-04-ok.pdf [ Links ]
15. Silva A, Ferreira GAL, Pereira RSF, Santos CA, Gusmão JL. Morbidade referida pelos trabalhadores do Serviço de Higiene de um hospital público de São José dos Campos - SP. Revista Atual in derme [online]. 2013; [acesso em 2014 ago 15];67:19-22. Disponível em: http://inderme.com.br/05-03.html [ Links ]
16. Murose NT, Marziale MHP. Doenças do sistema osteomuscular em trabalhadores de enfermagem. Rev Latino Am Enfermagem [online]. 2005 maio/jun; [acesso em 2014 set 13];13(3):364-73. Disponível em: http://www.scielo.br/pdf/rlae/v13n3/v13n3a11.pdf [ Links ]
17. Köhler APPC, Versari AF, Roriz CC, Paula SN. Hipertensão e tabagismo: um estudo com usuários de uma unidade básica de saúde no município de JI-Paraná - roraima. netsaber [internet]. 2007. disponível em: http://artigos.netsaber.com.br/resumo_artigo_5425/artigo_sobre_hipertensao-e-tabagismo [ Links ]
18. Santos MN, Marques AC. Condições de saúde, estilo de vida e características de trabalho de professores de uma cidade do sul do Brasil. Ciênc Saúde Colet [online]. 2013 mar; [acesso em 2014 ago 19];18(3):837-46. Disponível em: http://www.scielo.br/pdf/csc/v18n3/29.pdf [ Links ]
19. Calumbi RA, Amorin JÁ, Maciel CMC, Filho OD, Teles AJF. Evaluation of the Quality of Life of Anesthesiologists in the City of Recife. Rev Bras Anestesiol [online]. 2010 jan/feb; [acesso em 2014 set 11];60(1):42-51. Disponível em: http://www.scielo.br/pdf/rba/v60n1/en_v60n1a05.pdf [ Links ]
20. Constantino MAC. Avaliação da qualidade de vida: desenvolvimento e validação de um instrumento, por meio de indicadores biopsicossociais, junto à comunidade da Universidade de São Paulo-USP [Tese]. São Paulo: Universidade de São Paulo; 2007. [ Links ]
21. Mazetto FAP. Qualidade de vida, qualidade ambiental e meio ambiente urbano: breve comparação de conceitos. Sociedade e Natureza [online]. 2000 jul-dez; [acesso em 2014 ago 10];12(24):21-31. Disponível em: http://www.seer.ufu.br/index.php/sociedadenatureza/article/view/28533/pdf_125 [ Links ]
22. Chazan ACS, Campos MR. Qualidade de Vida de Estudantes de Medicina medida pelo WHOQOL-bref - UERJ, 2010. Rev Bras de Educ Méd [online]. 2013 jul/set; [acesso em 2014 set 10];37(3):376-84. Disponível em: http://www.scielo.br/pdf/rbem/v37n3/10.pdf [ Links ]
23. Mascarenhas CHM, Prado FO, Fernandes MH. Fatores associados à qualidade de vida de agentes comunitários de saúde. Ciência Saúde Colet [online]. 2013 maio; [acesso em 2014 set 20];18(5):1375-86. Disponível em: http://www.scielo.br/pdf/csc/v18n5/23.pdf [ Links ]
24. Paschoa S, Zanei SSV, Whitaker IY. Qualidade de vida dos trabalhadores de enfermagem de unidades de terapia intensiva. Acta Paul Enf [online]. 2007 jul/set; [acesso em 2014 Jul 15];20(3). Disponível em: http://www.scielo.br/pdf/ape/v20n3/a10v20n3.pdf [ Links ]
25. Pereira EF, Teixiera CS, Lopes AS. Qualidade de vida de professores de educação básica do município de Florianópolis, SC, Brasil. Ciênc Saúde Colet [internet]. 2013 jul; [acesso em: 2014 ago 12];18(7):1963-70. Disponível em: http://www.scielo.br/pdf/csc/v18n7/11.pdf [ Links ]
26. Stephane T, Santos AM, Marinovic A, Hortense P. Chronic low back pain: pain intensity, disability and quality of life. Acta Paul Enf [online]. 2013; [acesso em 2014 jul 11];26(1):14-20. Available from: http://www.scielo.br/pdf/ape/v26n1/en_04.pdf [ Links ]
27. Gordia AP. Associação da atividade física, consumo de álcool e índice da massa corporal com a qualidade de vida de adolescentes [dissertação]. Curitiba (RS): Universidade Federal do Paraná, 2008. [ Links ]
28. Castro MR, Matsuo T, Nunes SOB. Clinical characteristics and quality of life of smokers at a referral Center for smoking cessation. J Bras Pneumol [online]. 2010 jan/feb; [acess em 2014 ago 12];36(1):67-74. Available from: http://www.scielo.br/pdf/jbpneu/v36n1/en_v36n1a12.pdf [ Links ]
Received: January 28, 2016; Accepted: March 26, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
