










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.16 n.47 Murcia Jul. 2017 Epub July 01, 2017
https://dx.doi.org/10.6018/eglobal.16.3.266571
Originales
Validation of the Subjective Happiness Scale in people with Chronic Kidney Disease
1 Nurse Specialist in Rehabilitation Nursing at Curry Cabral Hospital, Centro Hospitalar Lisboa Central. Professor of the Universidad Atlántica. Portugal
2 Nurse Specialist in Rehabilitation Nursing at Curry Cabral Hospital, Centro Hospitalar Lisboa Central. Portugal.
3 Specialist in Rehabilitation Nursing at Fernando da Fonseca Hospital. Portugal.
4 ESpecialist in Medical-Surgical, CIIS Researcher and Scholar of the European Academy of Nursing Science. Director of the Multipefil Health School, Luanda, Angola.
Objective
To explore the psychometric properties of the Subjective Happiness Scale (SHS) in patients with Chronic Kidney Disease (CKD) under hemodialysis.
Methods
This is a methodological study. The random sample included 171 patients with CKD under hemodialysis program in two clinics in the region of Lisbon, Portugal. Data was collected between May and June 2015. The following psychometric properties were evaluated: validity (construct, convergent and discriminant), reliability through internal consistency (Cronbach α) and stability (intraclass correlation coefficient and Spearman-Brown correlation coefficient).
Results
The results support the unifactorial structure, with reliability (α = 0.90). In addition, this scale is positively correlated with the Satisfaction Life Scale (r = 0.60; p <0.001), supporting the validity criteria.
Keywords: Renal Insufficiency; Chronic; Validation studies; Psychometrics; Happiness; Nursing
INTRODUCTION
Chronic Kidney Disease (CKD) is a degenerative disease characterized by the progressive, gradual and irreversible destruction of a large number of nephrons and consequently, decreased capacity of the kidneys to excrete metabolites, corresponding to a loss of renal function1)(2)(3)(4. Hemodialysis is one of the options for treating people with CKD. This technique consists of extracorporeal blood filtration by means of a machine. Hemodialysis has an impact on the physical, psychological and social level, with repercussions on personal and family life1.
Subjective well-being or happiness5 can be described as stable extroversion, which seems to be related to easy sociability, which favors a natural and enjoyable interaction with other people. The person with the higher level of well-being seems to have better social relations than the one with a reduced level of well-being5.
The Subjective Happiness Scale (SHS), developed by Lyubomirski and Lepper6) consists of four items, The SHS is composed of four items: within two items (two and three) respondents are asked to characterize and compare themselves with others, both in absolute and relative terms; the two other items correspond to descriptions of happiness and unhappiness. The score is reversed in the last item.
This scale requests one to indicate the extent to which the statements presented characterize them. The answer is given on a visual analogical scale with seven positions, based on two antagonistic statements, which express the level of happiness or its lack. Its authors conceived the one-dimensional measure of the scale, with only four items, so as not to overload the participants.
The SHS was developed for both the North American and Russian population6, however, it has been validated in other populations, namely the Japanese7, the Chinese and Malay8, Australian, German and Filipino9 Chinese students10, Arabic11, Spanish12, Italian13, European Portuguese14)(15, Brazilian Portuguese16 and Mexican population17.
In the construct validity only one dimension was demonstrated, this study was done by exploratory factorial analysis6)(9)(10)(12)(13)(14)(15)(16, with Principal Component Analysis12 or Principal Axis Factoring9)(16 with rotation Quartimax9 and by confirmatory factor analysis10)(11)(12)(13)(14)(15)(16)(17.
Concurrent validity was achieved with other measures related to happiness6)(9, satisfaction with life9)(13)(14)(15)(16, affectivity6)(9, self esteem(6,16), hope16, quality of life10, depression6)(13, and anxiety13)(14.
Regarding the reliability of the original scale, it has a Cronbach's alpha ranging from 0.79 to 0.94 (M = 0.86) which has shown a good internal consistency. It exhibits stability over time, with test retest reliability ranging from 0.55 to 0.90 (M = 072)6. In all populations, the scale has proved to be a valid and reliable instrument for assessing subjective happiness7)(8)(9)(10)(11)(12)(13)(14)(15)(16. The Portuguese version of the scale revealed psychometric properties identical to those of the original version6 and can be used to make comparisons in cross-cultural investigations15).
Given the above, this study aims to determine whether the Portuguese version of SHS15 is considered valid and reliable in patients with CKD under hemodialysis.
METHOD
This is a methodological study18, carried out in June 2015, in two dialysis units of Diaverum in the Lisbon region.
The sample is comprised of patients with CKD under hemodialysis.
Inclusion criteria were as follows: CKD, undergoing hemodialysis for at least six months, aged 18 years or over. People with cognitive impairment and active psychiatric illness were excluded. The information on the exclusion criteria was obtained through the clinical history, recorded in the clinical process.
The population was composed of a group of 248 people with CKD, who met the inclusion criteria (139 of clinic 1 1 114 of clinic 2). The sample consisted of individuals who accepted the eligibility criteria and their evaluation was 19% (19), in order to obtain a minimum sample of 192 people (103 at clinic 1 and 89 at clinic 2). A random selection without replacement was made. Concerning Clinic 1, six people refused to participate, two were hospitalized and two dropped out. In clinic 2, four people refused to participate, two were hospitalized and five gave up. Data were obtained from 171 people, 93 from clinic 1 (89%) and 78 (88%) from clinic 2.
For data collection, the Portuguese version of SHS15 was used to evaluate happiness and to evaluate satisfaction with life in general, the Personal Welfare Index (PWI)20 was used to collect data whose original version is the PWI, developed from the Comprehensive Quality of Life Scale21. An instrument was also used to characterize the profile of the sample at the sociodemographic and clinical level, specifically, age, gender, nationality, schooling, professional activity, marital status, dialysis time, presence of Arterial Hypertension and Diabetes.
The SHS is asked to indicate the extent to which the four affirmations characterize them, with a visual analog scale graded from 0 to 7. The Portuguese version presents a single factor and has an internal reliability with the value of Cronbach's α of 0.7615.
The PWI consists of seven items / domains (satisfaction with standard of living, health, personal fulfillment, personal relationships, sense of security, community attachment, and security with the future) that aim to evaluate "satisfaction with life in general ". For each question respondents are asked to say how satisfied they are with each item / domain on a scale from "0" (extremely dissatisfied) to "10" (extremely satisfied) with a neutral intermediate position. The PWI is calculated on a score of 0-100 (maximum percentage of the scale). The confirmatory factor analysis of the Portuguese version demonstrates the existence of a single factor, with the Cronbach's Alpha value of 0.8120.
Statistical analyzes were performed with the Statistical Package for Social Sciences (SPSS) version 20.0. Reproducibility was studied by internal consistency and stability. The reliability study was performed using the Cronbach's α and to evaluate stability the Intraclass Correlation Coefficient (ICC) and Spearman-Brown Correlation Coefficient22 in the Retest Test (after 48 to 96 hours in 40 people randomly selected, 26 per questionnaire and 14 per interview) were used. A minimum value of 0.70 was adopted as a satisfactory internal consistency22.
In this study the validity of the construct, concurrent and discriminant was analyzed. The construct validity was performed using exploratory factorial analysis (EFA) and confirmatory factorial analysis (CFA). The CFA was performed using the maximum likelihood method, with Varimax rotation. Adequacy was estimated by Kaiser-Meyer-Olkin (KMO) and Bartlett's sphericity test.
The CFA was developed using AMOS 21.0 software. The robust estimation method was used in maximum likelihood23. The adjustment indexes used to verify the adjustment of the model were: ratio between chi-square and degrees of freedom ratio (Χ2 / g.l); Goodness-of-fit index (GFI), root mean square error of approximation (RMSEA); Comparative fit index (CFI), Tucker-Lewis index (TLI)((22)(23.
These indices can be classified into absolute indexes and relative indices. The Absolute Indices evaluate the quality of the model, without comparing with other models. The most used indices in this family are: Χ2 / g.l. that when Χ2 / g.l. = 1, the fit is perfect, when Χ2 / g.l. is less than 2, the fit is good, it is acceptable when Χ2 / g.l. <a 5 and unacceptable when Χ2 / g.l.> 5. Root Mean Square Residual (RMSR) is determined by dividing the square root of the error matrix by the degrees of freedom. Thus, the lower the RMSR the better the adjustment. When RMSR = 0 indicates that the adjustment is perfect. The Goodness of Fit Index (GFI) explains the proportion of the observed covariance among the manifested variables, explained by the fitted models. In general, GFI <a 0.8 indicates models with poor fit to the data; GFI between [0.9; 0.95 [indicates a good fit; GFI> at 0.95 indicate very good fit and GFI = 1 perfect fit. The Relative Indices evaluate the quality of the model under test, relative to the model with the worst possible adjustment and / or the model with the best possible adjustment. The Comparative Fit Index (CFI) compares the adjustment of the model under study (Χ2) with the degrees of freedom (gl), with the adjustment of the basal model with degrees of freedom. It is generally accepted that CFI <a 0.9 indicates models with poor fit; CFI between [0.9; 0.95 [indicates a good fit; CFI> at 0.95 very good adjustment and CFI = 1 perfect fit. The TILI-Lewis Index (TLI), also known as Bentler-Bonett-non-normed fit index (NNFI), where TLI values range from 0 to 1. Values close to 1 indicate very good fit23.
The convergent validity was verified through the Pearson Correlation Coefficient between SHS and PWI. To verify the discriminant validity, the student t test for independent samples or ANOVA was used for more than two independent samples (verified normal distribution by Kolmogorov-Smirnov KS test).
Categorical variables were expressed as percentage or absolute value and continuous variables as mean ± standard deviation or median. The cutoff point was the median age and the time of hemodialysis to create category variables. The level of significance was set at p <0.05.
Permission of author of the Portuguese versions of SHS15 and PWI19 was requested and granted.
This study was approved by Diaverum's Ethics Committee (nº1 / 2015). All participants signed the informed consent form after being informed about the guarantee of confidentiality of their data and the right of withdrawal.
RESULTS
The socio-demographic and health profile is shown in Table 1. In this study the mean age of the sample is 60.20 ± 14.34 years. The majority are men (61%), Portuguese (80.1%), 4 years of schooling (42.9%), retired (76.7%) and married (56.5%). Regarding health data, the subjects of the sample underwent hemodialysis for 72,17 ± 54,23 months, 62,1% referred Hypertension and 27,1% has Diabetes.

Reliability and stability
In the analysis of the psychometric properties, the reproducibility of SHS, verified by the coefficient of Cronbach α, varied from 0.85 to 0.90 after the exclusion of each of the items. In the stability evaluation (Test-Retest), the data obtained by questionnaire (n = 26) presented a global Cronbach's α in the first evaluation of 0.80 and in the second evaluation of 0.61. The Spearman-Brown Correlation Coefficient was 0.82 and the ICC was 0.82 [95% CI; 0.71 to 0.91, p <0.001]. By interview (n = 14) the global Cronbach's α in the first evaluation was 0.83 and in the second evaluation was 0.85. The Spearman-Brown Correlation Coefficient was 0.77 and the ICC was 0.87 [95% CI; 0.74 to 0.95, p <0.001]. In this way the consistency and the stability between the SHS evaluations were demonstrated through a self-reported questionnaire and interview.
Validity
The exploratory factorial analysis (KMO = 0.83; Bartlett χ2 sphericity test [6] 486,679, p <0.001) presented a single factorial solution, which was responsible for 72.10% of the explained variance of the construct. All items were loaded into the factor, with adequate factor loads (ie> 0.6, see Table 2). The value of Cronbach's α coefficient was 0.90.
Table 2 Exploratory factorial analysis of the Portuguese version of SHS in patients with CKD. Lisbon, Portugal, 2015.

*Subjective Happiness
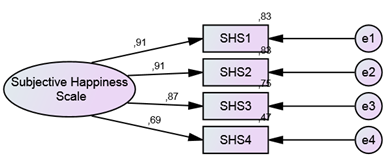
The confirmatory factorial analysis obtained, Χ2 / g.l = 0.971, RMSEA = 0.00; GFI = 0.994, CFI = 1.00 and TLI = 1.00. These values show a very good fit for the hypothesis of one solving factor (Figure 1).
In the study of convergent validity, there was a moderate positive correlation (r = 0.60; p <0.001) between the SHS score and the PWI. Table 3 shows the results regarding discriminant validity in order to identify whether SHS is able to differentiate subjective happiness in the variables gender, age, nationality, schooling, occupational activity, marital status, presence of Hypertension, Diabetes and dialysis time.
The SHS can discriminate by age, nationality, occupational activity and presence of diabetes. In this sense, people under the age of 63, with an occupational activity, have higher levels of happiness. People of Portuguese nationality have lower levels of happiness than people with the nationality of an African country. In addition, people with diabetes have lower levels of happiness than those without diabetes.

DISCUSSION
The reliability values were similar to the original version6 and higher than the Austrian (α = 0.80)9, Filipino (α = 0.82)9, Chinese (α = 0.82)10, Brazilian (α = 0.74)12, Brazilian (α = 0.81)13, Italian (α = 0.79)14) and European Portuguese (α = 0.84)16. The Cronbach's α values obtained in this study are considered good22. On what concerns stability, in both questionnaire and interview, correlation values were interview, was higher than the original study (r = 0.55 to 0.86)6, Chinese version (r = 0.70)10, Spanish version (r = 0.72)13. In this study the values are higher than 0.7 which indicates that there is good stability of the measurement22. We obtained support for the stability of this measure in the questionnaire and interview modality.
All items were loaded on a single factor, similar to other studies that performed exploratory factor analysis6)(7)(9)(10)(16. The factorial weight was identical to the Chinese and Portuguese versions of Brazil (> 0.60) and higher than the Lebanese version (> 0.46). The KMO value was higher than the Austrian (KMO = 0.80)9) and Philippine (KMO = 0.65)9, Chinese (KMO = 0.7910, Lebanese (KMO = 75)12 and Brazilian Portuguese (KMO = 0.79)16 versions. In this study the KMO value is good and reveals the adequacy of the model to the data22. The variance explained for one factor was higher than the Austrian (65.7%)9 and Filipino (53.2%)9, Chinese (65.3%)10, Lebanese (45.2%)12) and Brazilian Portuguese (64.2%)16 versions. It was thus demonstrated that the SHS score is valid for measuring subjective happiness. In this study the CFA also supported the one factor solution11)(12)(13)(14)(15)(16)(17.
The convergent validity also presented results in the expected directions, that is, high SHS scores are associated with high PWI scores (satisfaction with life in general). Support was obtained for the external validity of the measure, similar to the samples9)(13)(14)(15)(16.
The SHS is able to distinguish patients with CKD under hemodialysis program by age, professional status, nationality and presence of Diabetes. In the Lebanese version it was verified that this measure can also distinguish patients by age and parents rejection in childhood12. In the Italian version it was observed that elderly men have a lower percentage of high scores (ceiling effect) and have higher percentage of low scores (floor effect) comparing to women and young people14.
Our main limitations were the sample size and lack of financial support.
The results of this study are in agreement with the original scale and all other adapted versions of SHS7)(8)(9)(10)(11)(12)(13)(14)(15)(16 and suggest that the European Portuguese version of SHS is a valid and reliable measure to evaluate subjective happiness in patients with CKD , in a self-filled questionnaire and interview format.
This study used a representative sample of patients with CKD under dialysis program. However, in future research it is important to perform a confirmatory factor analysis in this specific population with a sample greater than 300 people.
CONCLUSIONS
The SHS in patients with CKD is a reliable, reproducible and valid instrument when applied as a questionnaire and interview. This tool presents good psychometric properties suggesting that it can be considered a good measure, with similar properties to the original and Portuguese version, as well as, to the versions in other languages and cultures.
REFERENCIAS
1. Takemoto AY, Okubo P, Bedendo J, Carreira L. Avaliação da qualidade de vida em idosos submetidos ao tratamento hemodialítico. Rev Gaúcha Enferm, Porto Alegre (RS). 2011;32(2):256-62. [ Links ]
2. Oliveira CS, da-Silva EC, Ferreira LW, Skalinski LM. Perfil dos pacientes renais crônicos em tratamento hemodialítico. Rev Baiana Enferm. 2015; 29(1):42-49. [ Links ]
3. Ottaviani AC, Souza EN, Drago NC, de Mendiondo MSZ, Pavarini SCL, Orlandi FS. Esperança e espiritualidade de pacientes renais crônicos em hemodiálise: estudo correlacional. Rev Latino-AmEnferm. 2014;22(2):248-54. [ Links ]
4. Bosenbecker NRV, Menegon MBC, Zillmer JGV, Dall'agnol J. Perfil das pessoas em hemodiálise de um serviço de nefrologia. J Nurs Health. 2015;5(1):38-46. [ Links ]
5. Passareli PM, Silva JAD. Psicologia positiva e o estudo do bem-estar subjetivo. EstudPsicol (Campinas). 2007; 24(4): 513-517. [ Links ]
6. Lyubomirsky S, Lepper HS. A measure of subjective happiness: preliminary reliability and construct validation. Soc Indic Res.1999;46(2):137-55. [ Links ]
7. Shimai S, Otake K, Utsuki N, Ikemi A, Lyubomirsky S. Development of a Japanese version of the Subjective Happiness Scale (SHS), and examination of its validity and reliability. Nippon Koshu Eisei Zasshi. 2004; 51: 845-853. [ Links ]
8. Swami V. Translation and validation of the Malay Subjective Happiness Scale. Soc Indic Res. 2008; 88: 347-353. [ Links ]
9. Swami V, Stieger S, Voracek M, Dressler SG, Eisma L, Furnham A. Psychometric evaluation of the Tagalog and German Subjective Happiness Scale and a cross-cultural comparison. Soc Indic Res. 2009;93:393-406. [ Links ]
10. Nan H, Ni MY, Lee PH, Tam WW, Lam TH, Leung GM, McDowell I. Psychometric evaluation of the Chinese version of the subjective happiness scale: evidence from the Hong Kong FAMILY Cohort. Int J Behav Med. 2014; 21(4): 646-652. [ Links ]
11. Moghnie L, Kazarian SS. Subjective happiness of Lebanese college youth in Lebanon: Factorial structure and invariance of the Arabic Subjective Happiness Scale. Soc Indic Res. 2012; 109(2): 203-210. [ Links ]
12. Extremera N,Fernández-Berrocal P. The Subjective Happiness Scale: Translation and preliminary psychometric evaluation of a Spanish version. Soc Indic Res. 2014;119(1): 473-481. [ Links ]
13. Iani L, Lauriola M, Layous K, Sirigatti S. Happiness in Italy: translation, factorial structure and norming of the subjective happiness scale in a large community sample. Soc Indic Res. 2014; 118(3): 953-967. [ Links ]
14. Spagnoli P, Caetano A, Silva A. Psychometric properties of a Portuguese version of the Subjective Happiness Scale. Soc Indic Res. 2012;105(1): 137-143. [ Links ]
15. Pais-Ribeiro JL. Validação transcultural da Escala de Felicidade Subjectiva de Lyubomirsky e Lepper. Psicol Saúde Doenças. 2012; 13(2): 157-168. [ Links ]
16. Damásio BF, Zanon C, Roller SH. Validation and psychometric properties of the Brazilian version of the Subjective Happiness Scale. Univ Psychol. 2014; 13(1): 17-24. [ Links ]
17. Quezada L, Landero R, González MT. A validity and reliability study of the Subjective Happiness Scale in Mexico. J Happiness Well-Being. 2016; 4(1): 90-100. [ Links ]
18. De Lima DVM. Desenhos de pesquisa: uma contribuição para autores. Online Braz J Nurs (Online). 2011[Acceso 18 Agosto 2015]; 10(2). Disponible en: http://www.objnursing.uff.br/index.php/nursing/article/view/3648/html [ Links ]
19. Santos GEO. Cálculo amostral: calculadora on-line. [Acceso 1 maio 2015].Disponible en: http://www.calculoamostral.vai.la. [ Links ]
20. Sousa LM, Marques-Vieira CM, Severino SS, Pozo-Rosado JL, José HM. Validación del Índice de Bien-estar Personal en personas con enfermedad renal crónica. Enfermería Nefrológica. 2016;19(2):135-41. [ Links ]
21. Cummins RA, McCabe MP, Romeo Y, Gullone E. The Comprehensive Quality of Life Scale: Instrument development and psychometric evaluation on tertiary staff and students. Educ Psychol Measur. 1994; 54: 372-382. [ Links ]
22. Sousa LMM, Marques-Vieira CMA, Carvalho ML, Veludo F, José HMG. Fidelidade e validade na construção e adequação de instrumentos de medida. Enformação. 2015 [Acceso 17 agosto 2015]; 5:25-32. Disponible en: http://www.acenfermeiros.pt/index.php?id1=15&id2=9. [ Links ]
23. Marôco J. Análise de equações estruturais: Fundamentos teóricos, software & aplicações. 2.ed. Pero Pinheiro: ReportNumber, Lda; 2014. [ Links ]
Received: August 31, 2016; Accepted: October 02, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
