










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.18 n.56 Murcia Oct. 2019 Epub Dec 23, 2019
https://dx.doi.org/10.6018/eglobal.18.4.358801
Originals
Sociodemographic and prenatal factors associated with anemia in Peruvian pregnant women
1General coordinator of the Research Department. Faculty of Health Sciences. Catholic University Sedes Sapientiae. Peru. yortiz@ucss.edu.pe
2Nurse. Research Department. Faculty of Health Sciences. Catholic University Sedes Sapientiae. Peru.
3Student of Nursing. Faculty of Health Sciences. Catholic University Sedes Sapientiae. Peru.
Objective
To determine the association between sociodemographic and prenatal factors with anemia in Peruvian pregnant women.
Method
Secondary analysis of the ENDES 2017 sample. The sample consisted pregnant women between 15 and 49 years old. The dependent variable was iron deficiency anemia and the independent variables were sociodemographic and prenatal factors. For the bivariate analysis. prevalence ratio was calculated.
Results
Regarding sociodemographic factors and anemia, pregnant women with a higher educational level have less possibility of presenting anemia (PR: 0,91; 95% CI: 0,42-1,96; p = 0,041). On the other hand, among the obstetric and prenatal factors associated with anemia were: initiate prenatal control in the third month (PR: 1,4; 95% CI: 0,74-1,58, p = 0,03) and be found in the second trimester of pregnancy ( PR: 1,35, 95% CI: 0,74-1,58; p = 0,04). While pregnant women who have more children (PR: 0,87; 95% CI: 0,78-0,97; p = 0,02) are less likely to have anemia.
Conclusion
The higher educational level and having more children are protective factors of anemia. The start of prenatal control from the third month and the second trimester of pregnancy were associated with the presence of anemia in pregnant women.
Keys words: Anemia; women; prenatal education
INTRODUCTION
Anemia in pregnant women, considered as a blood hemoglobin (Hb) concentration lower than 110 g / l, is one of the most important public health problems1. The World Health Organization (WHO) reports that 56,4 million pregnant women have anemia worldwide2. The highest prevalence of this pathology occurred in Africa and Southeast Asia, that is, in developing countries3. The prevalence of anemia in pregnant women in 2016 in Latin America and the Caribbean was 29,5%4and in Peru it was 25,8%5. With respect to the provinces of Peru, Huancavelica and Puno registered 45,5% and 42,8% respectively5.
During pregnancy, anemia has a significant impact on both the health of the fetus and the mother. Consequently, premature rupture of membranes, premature birth, oligohydramnios, susceptibility to develop infections, hemorrhages, etc6,7. As for the newborn, it conditions the appearance of cardiovascular diseases in his adult life8, In addition, an anemic pregnant woman who presents with obstetric hemorrhage and puerperal infection has a higher probability of death in relation to those who do not present this pathology9,10.
Taking into account that anemia in pregnant women can be prevented, there are certain factors that constitute this pathology. Among them are not attending regularly or going too late to their prenatal check-ups11,12; have lower levels of education10,11,13, which lead to ignorance of care before and during pregnancy12; being a primiparous mother11,14and being in the second trimester of pregnancy15,16.
In consideration of the above, anemia in pregnant women is one of the causes of maternal-fetal death17so it is important to know the factors to prevent it. For this reason, the objective of this study was to determine the relationship of sociodemographic, obstetric and prenatal factors to anemia in pregnant women according to the Encuesta Demográfica y de Salud Familiar (ENDES) 2017.
METHOD
Study of quantitative, non-experimental and analytical approach. A secondary analysis of the database of the Encuesta Demográfica y de Salud Familiar 2017 (ENDES 2017) was carried out. The ENDES was done by the Instituto Nacional de Estadística e Informática (INEI)11to obtain data that may have a national representativeness. The sample design was two-stage through conglomerates and homes.
The effective sample consisted of 639 women between 15 - 49 years. Only women who are between the first to the ninth month of their pregnancy and who have been able to answer the obstetric and prenatal questions were included.
The main variable was anemia, defined as the concentration of hemoglobin less than 11 g / dl in pregnant women18. It was categorized into iron-deficiency anemia (less than 11 g / dl) and did not present anemia (greater than or equal to 11 g / dl). For the measurement of this variable, the Hemocue® instrument (an instantaneous and reliable photometric method) was used as well as being adjusted by the subject's altitude applying the formula ofPediatric Nutrition Surveillance System(CDC / PNSS) andDirren19.
For the measurement of sociodemographic variables, age in years, quantitative variable; natural region, (metropolitan Lima, rest of coast, mountain and jungle); educational level, qualitative polytomous variable (without education, primary, secondary and higher); residence, dichotomous qualitative variable (urban and rural); quintile of wealth defined in relation to wealth in the households surveyed, was taken into account. Instead of income, the wealth quintile depends on the availability of goods and services as well as the characteristics of the dwellings. It is an ordinal qualitative variable (upper quintile, fourth quintile, quintile intermediate, second quintile and lower quintile)20and marital status: single, married, cohabiting and others. Regarding the obstetric and prenatal variables were: number of children, quantitative variable; gestational age, qualitative polytomous variable (first trimester, second trimester and third trimester); beginning of prenatal control, qualitative polytomous variable (1st month, 2nd month, third month to more) and number of controls, quantitative variable.
For the statistical analysis of the study, the statistical package Stata version 14 was used. Descriptive statistical analysis was performed obtaining frequency and percentages for the qualitative variables and averages and standard deviation for the quantitative variables. In the inferential analysis we used the normality and variance test of the quantitative variables to be able to use the correct statistical analysis when they intersect with other variables. TheStudent's Ttest and the Chi-square statistical test were performed. In the unadjusted bivariate analysis, Poisson regression was used with the robust variance estimate, calculating the crude prevalence ratio (PR)21and 95% confidence intervals. All these analyzes had a statistical significance less than 0,05. Regarding the ethical aspects, ENDES is a public access database in which women were surveyed with verbal consent.
RESULTS
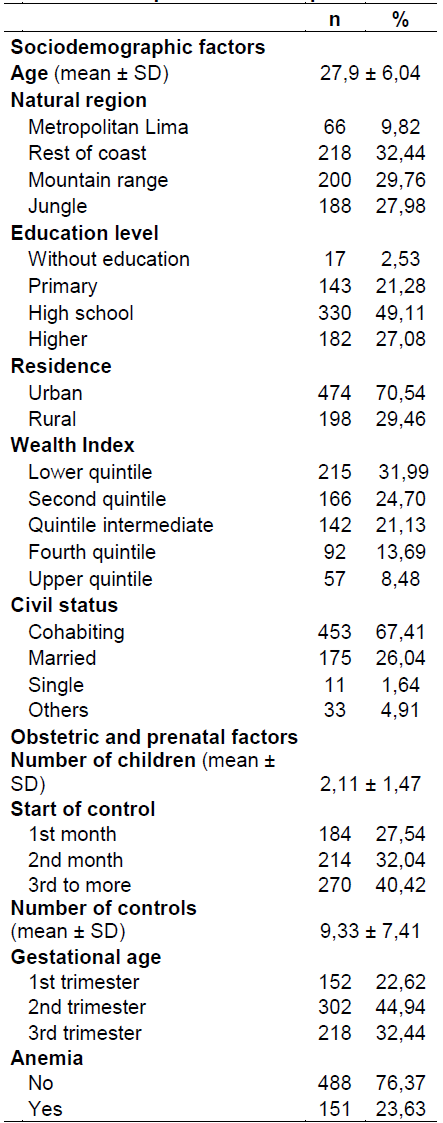
Of the total of 639 pregnant women, the average age was 27 years, 49,1% had a secondary education level, 31,9% belonged to a lower quintile and 67,4% were cohabiting. In addition, of the total number of respondents, the mean number of children was 2,11, 40,4% started their control after the third month, 44,9% were found in the second trimester of pregnancy, 76,3% had anemia and 23,6 did not present the same (see Table 1).
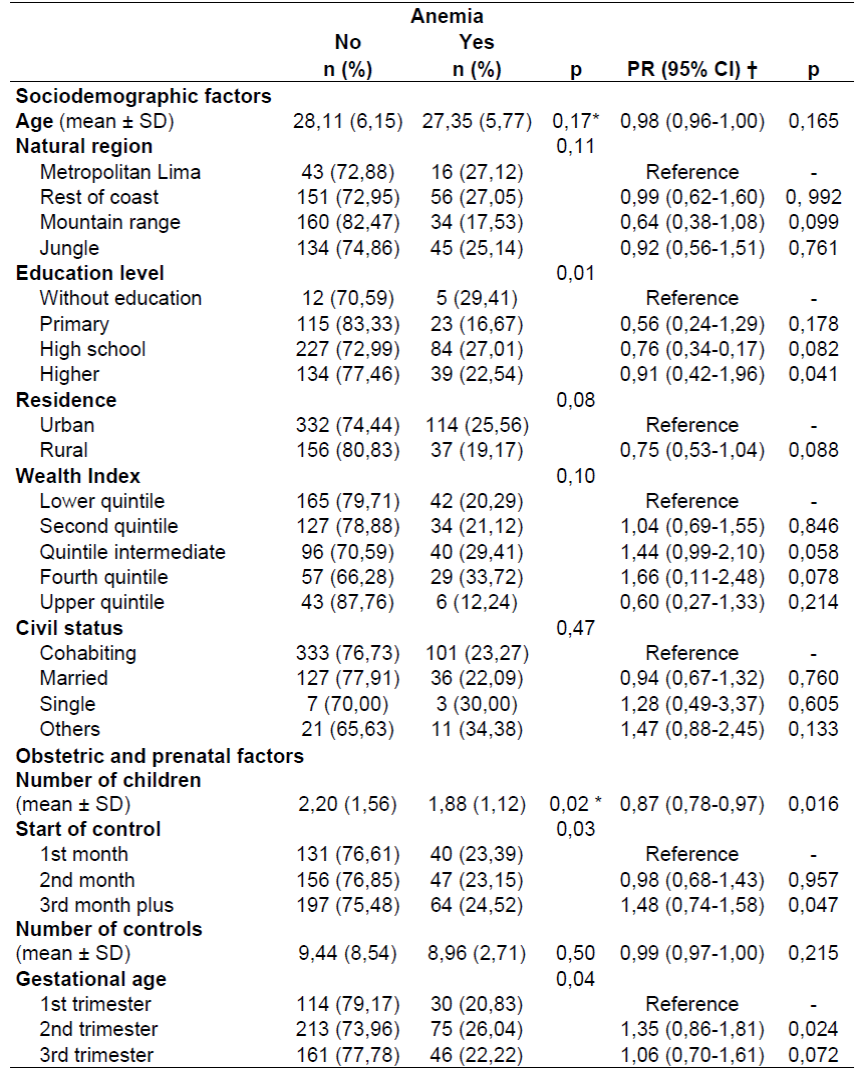
In Table 2, both in the descriptive bivariate analysis and the unadjusted (crude) model, the sociodemographic factor associated with anemia was the educational level (p = 0,041). That is, pregnant women with a higher educational level are less likely to have anemia compared to those without education (PR: 0,91, 95% CI: 0,42-1,96). On the other hand, having fewer children (p = 0,02), starting prenatal control in the third month (p = 0,03) and being in the second trimester of pregnancy (p = 0,04) were associated with the presence of anemia. The rest of the associations were not significant, Regarding the analysis of the unadjusted (crude) model, the obstetric and prenatal factors associated with anemia were: the number of children (0,016), the start of prenatal control (p = 0,047) and gestational age (p = 0,024), Pregnant women with more children are less likely to have anemia compared to those with fewer children (PR: 0,87, 95% CI (0,42-1,96). On the other hand, pregnant women who initiate their control as of third month they have 1,48 times more chance of presenting anemia than those who started their control in the first month (PR: 1,4, 95% CI: 0,74-1,58). The second trimester of pregnancy is 1,35 times more likely to have anemia than those found in the first trimester (PR: 1,35, 95% CI: 0,74-1,58).
DISCUSSION
In this study of the total of pregnant women, 23,6% presented anemia. In addition, the sociodemographic protective factor associated with anemia was the higher educational level. Regarding the obstetric-prenatal factors associated with anemia, the beginning of prenatal control was started from the third month and the second trimester of pregnancy. A protective factor was having more children.
In the present study it was evidenced that pregnant women with a higher educational level have less possibility of presenting anemia compared to those without education. Studies reported that low educational level and awareness of anemia also contributed to the increase of this pathology in pregnant women10,13. Women with a lack of education are generally of low socioeconomic class, therefore they do not have access to good maternal health services. Therefore, they are more prone to poor nutrition and other infections during pregnancy10. It should be noted that pregnant women who presented anemia before pregnancy, a condition that had to be treated previously, brings a series of complications both for the health of the fetus and the mother and even the death of both10, due to lack of knowledge in preparing to have a future baby. Studies report that the key to reducing the prevalence of anemia is the educational and economic empowerment of women13,22.
Another finding of the study was that pregnant women with more children have fewer times of presenting anemia compared to those with fewer children. Studies reported that primiparous women had anemia compared to multiparous women14,23. Although anemia in pregnancy is often related to the increase in parity due to repeated drainage of iron stores22. It usually happens that in primiparous women due to lack of knowledge, lack of prenatal care and not preparing for the birth of their baby (with the iron and folic acid supplement before getting pregnant) they have anemia and they get worse with the advance of the months of pregnancy22,23. Given the above, the socio - demographic profile of pregnant women in the study, most have a lower quintile and low educational levels, therefore pregnant women who have fewer children have not become aware of the importance of nutrition during pregnancy24and do not know that the healthy diet in relation to daily requirements is three main meals plus an additional ration and consume supplements that provide vitamins and minerals orally7,25.
In the same way, pregnant women who are in the second trimester of pregnancy presented anemia, Studies report that anemia occurs in pregnant women as pregnancy progresses10,15. Another study showed that in the second trimester of pregnancy (week sixteen) the hemoglobin levels were lower than 10,5 g / dl16, since in this trimester of pregnancy the level of hemogline is decreased due to hemodilution by the increase in plasma volume by 45% to 50% for the needs of the uterus and growing fetus; an underlying maternal infection and untreated anemia in the first trimester of pregnancy.
Significantly, most pregnant women in the study began prenatal care after the third month, this is similar to reports from other studies14,15where the prevalence of anemia was 4,08% in the first weeks of gestation and it increased as the pregnancy progressed to 16,32%15. Finally, in the United Arab Emirates, it was found that pregnant women who had fewer prenatal controls increased the risk of anemia14. In the prenatal controls, relevant information is extracted from the mother and from them nutritional counseling is provided, including vitamin and mineral supplements such as folic acid and iron, The growth and optimal development of the embryo or fetus is also controlled25. That is why, if the pregnant woman initiates her controls early and continues with the counseling in each trimester, she will reduce the risk of anemia and its complications7.
Limitations
The study was limited to the secondary analysis of the ENDES 2017 database; that is, there was no control in the collection and processing of the variables for the analysis. For that reason, do not consider the interest on other study that could be considered in future studies with multivariate analysis considering medical history as urinary tract infections and family history in order to better address the phenomenon and its multiple causes. Regarding the strengths, this study was analyzed in a representative sample, since ENDES 2017 was carried out at a national level, and there are few studies that link anemia with databases at the national level.
CONCLUSIONS
In this study, 23,6% of pregnant women have anemia. Higher educational level and having more children are protective factors of anemia in pregnant women. The start of prenatal control from the third month and the second trimester of pregnancy was associated with the presence of anemia in pregnant women.
Recommendations
Nursing professionals are recommended to treat anemia in women as a priority and duty in continuous monitoring through training and multidisciplinary work. Therefore, it is necessary to educate the pregnant women about the importance of attending their prenatal check-ups regularly, motivate and encourage the supplemental consumption of iron and folic acid and healthy and balanced diets. Also, adequate follow-up during pregnancy, mainly in the second trimester to avoid complications. In the same way, nurses should make women aware of how to prepare for a pregnancy through the early consumption of ferrous sulfate and folic acid, the control of the blood hemoglobin test, healthy diets, etc. in order to avoid not only the appearance of anemia during pregnancy but other infections and / or complications.
REFERENCIAS
1. World Health Organization. The global prevalence of anaemia in 2011. The global prevalence of anaemia in 2011 [Internet]. Geneve: WHO; 2015 [citado el 17 de noviembre de 2018]. Disponible en: http://apps.who.int/iris/bitstream/handle/10665/177094/9789241564960_eng.pdf?sequence=1 [ Links ]
2. Organización Mundial de la Salud. Sistema de Información Nutricional sobre Vitaminas y Minerales (VMNIS) [Internet]. Ginebra: OMS; 2018 [citado el 17 de noviembre de 2018]. Disponible en: https://www.who.int/vmnis/database/anaemia/anaemia_status_summary/es/ [ Links ]
3. Organización Mundial de la Salud. Recomendaciones de la OMS sobre atención prenatal para una experiencia positiva del embarazo [Internet]. Washington, DC: Organización Panamericana de la Salud; 2018 [citado el 17 de noviembre del 2018]. Disponible en: http://www.clap.ops-oms.org/publicaciones/9789275320334esp.pdf [ Links ]
4. Banco Mundial. Prevalencia de anemia entre embarazadas [Internet]. Washington, DC: BM; 2018 [Citado el 17 de noviembre de 2018]. Disponible en: https://datos.bancomundial.org/indicador/SH.PRG.ANEM?end=2011&locations=ZJ&start=1990 [ Links ]
5. Banco Mundial. Prevalencia de anemia entre embarazadas [Internet]. Washington, DC: BM; 2018 [Citado el 17 de noviembre de 2018]. Disponible en: https://datos.bancomundial.org/indicador/SH.PRG.ANEM?end=2016&locations=PE&start=1990 [ Links ]
6. Espitia F, Orozco L. Anemia en el embarazo, un problema de salud que puede prevenirse. Revista Médicas UIS. 2013; 26(3):45-50. [ Links ]
7. Jiménez S, Rodríguez A, Pita G. Prevalencia de anemia durante el embarazo en Cuba. Evolución en 15 años. Revista Española de Nutrición Comunitaria. 2014; 20(2):42-47. [ Links ]
8. Barretto L, Mackinnon MJ, Poy MS, Wiedemann A, López LB. Estado actual del conocimiento sobre el cuidado nutricional de la mujer embarazada. Revista Española de Nutrición Humana y Dietética. 2014; 18(4): 226-237. [ Links ]
9. Gil F. Situación Epidemiológica de la Muerte Materna en el Perú 2015. Boletín Epidemiológico (Lima-Perú). 2016; 25(4): 66-74. [ Links ]
10. Nwizu EN, Iliyasu Z, Ibrahim SA, Galadanci HS. Socio-demographic and maternal factors in anaemia in pregnancy at booking in Kano, northern Nigeria. African journal of reproductive health. 2011; 15(4):33-41. [ Links ]
11. Instituto Nacional de Estadística e Informática. Encuesta Demográfica y de Salud Familiar-ENDES 2017 [Internet]. Lima: INEI; 2018 [citado el 13 de noviembre de 2018]. Disponible en: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1525/index.html [ Links ]
12. Castillo IY, Fortich LM, Padilla J, Monroy MA, Morales Y, Ahumada AM. Factores asociados al uso adecuado del control prenatal en 13 municipios de Bolívar, Colombia. Revista Cubana de Enfermería. 2017; 33(1): 1-14. [ Links ]
13. Noronha JA, Bhaduri A, Bhat HV, Kamath A. Maternal risk factors and anaemia in pregnancy: a prospective retrospective cohort study. Journal of Obstetrics and Gynaecology. 2011; 30(2): 132-136. [ Links ]
14. Ahmed A, Nasir H, Shafiq QA, Naeem B, Ghelani Y, Shaikh RB. The Effect of Anemia on Pregnancy and Fetal Outcome: GMC Hospital, Ajman, UAE. Gulf Medical Journal. 2015; 4(S1):S76-S82. [ Links ]
15. O'Farrill F, O'Farrill M, Fragoso LE. Evaluación del tratamiento a mujeres embarazadas con anemia ferropénica. Ginecología y Obstetricia de México. 2013; 81(7): 377-381. [ Links ]
16. O'Brien K, Ru Y. Iron status of North American pregnant women: an update on longitudinal data and gaps in knowledge from the United States and Canada. The American Journal of Clinical Nutrition. 2017; 106(6): 1647-1654. [ Links ]
17. World Health Organization. The prevalence of anaemia in women: a tabulation of available information. Geneva: WHO; 1992 [citado el 19 de diciembre de 2018]. Disponible en: http://www.who.int/iris/handle/10665/58994 [ Links ]
18. Organización Mundial de la Salud. Concentraciones de hemoglobina para diagnosticar la anemia y evaluar su gravedad [Internet]. Ginebra: OMS, 2011 [citado el 3 de enero de 2019]. Disponible en: https://www.who.int/vmnis/indicators/haemoglobin_es.pdf [ Links ]
19. Gómez I, Rosales S, Agreda L, Castillo A, Alarcón E, Gutiérrez C. Nivel de hemoglobina y prevalencia de anemia en gestantes según características socio-demográficas y prenatales. Revista Peruana de Epidemiología. 2014; 18(2): 1-6. [ Links ]
20. Enríquez Y, Ortiz K, Ortiz Y. Análisis de los determinantes próximos e impacto de la ocupación en la fertilidad de mujeres peruanas. Rev Panam Salud Publica. 2017; 41: 1-9. [ Links ]
21. Espelt A, Marí M, Penelo E, Bosque M. Estimación de la Razón de Prevalencia con distintos modelos de Regresión: Ejemplo de un estudio internacional en investigación de las adicciones. Adicciones. 2017; 29(2):105-112. [ Links ]
22. Bukar M, Audu B, Yahaya U, Melah G. Anaemia in pregnancy at booking in Gombe, North-eastern Nigeria. Journal of Obstetrics and Gynaecology. 2008; 28(8): 775-778. [ Links ]
23. Olubukola A, Odunayo A, Adesina A. Anemia in pregnancy at two levels of health care in Ibadan, south west Nigeria. Annals of African medicine.2011; 10(4): 272-277. [ Links ]
24. Paredes IE, Choque LF, Linares A. Factores asociados a los niveles de anemia en gestantes del hospital Hipólito Unanue, Tacna 2016. Revista Médica Basadrina. 2018; 12(1): 28-34. [ Links ]
25. Aguilar LA. Consejería nutricional en el marco de la atención integral de salud de la gestante y puérpera: guía técnica [Internet] Lima: MINSA, INS; 2016 [citado el 22 de noviembre de 2018]. Disponible en: https://web.ins.gob.pe/sites/default/files/Archivos/cenan/deprydan/documentosNormativos/2_Guia_Gestante_final-ISBN.pdf [ Links ]
Received: January 16, 2019; Accepted: February 20, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
