










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.19 n.60 Murcia Oct. 2020 Epub Dec 21, 2020
https://dx.doi.org/10.6018/eglobal.417261
Originals
Compassion satisfaction and compassion fatigue in oncology nursing staff: descriptive and correlational study
1Bilbao School of Education. Department of Evolutionary and Educational Psychology. University of the Basque Country. Leioa. Spain. silvia_arribas@ehu.eus
2Faculty of Education, Philosophy and Anthropology. Department of Evolutionary and Educational Psychology. University of the Basque Country. Donostia. Spain.
Objectives:
(1) To determine the perception of Compassion Satisfaction and Fatigue of oncology nursing staff; (2) to study the correlation between Compassion Satisfaction and Fatigue and sociodemographic, professional and adaptive variables (resilience, attitudes toward death, personality); and (3) to identify predictors of the two dimensions.
Method
Descriptive, correlational, cross-sectional study. 69 nurses (62.7%) and 41 auxiliary care technicians (37.3%) from the Oncology Services in Biscay (Basque Health Service) completed the ProQOL-V, CD-RISC-10, DAP-R, and NEO-FFI-3. Data were collected between September 2018 and March 2019. The statistical analysis with SPSS.22 included chi-square tests, comparison of means, Pearson´s correlation, and multivariate logistic regression.
Results:
66.4% (n=73) showed high Compassion Satisfaction, and 41.8% (n=46) were at moderate levels of Compassion Fatigue. People with prior studies related to death and/or grief were more satisfied. Compassion Satisfaction had stronger correlations with resilience and extroversion, and Compassion Fatigue did so with neuroticism and resilience. Four predictor variables emerged for Compassion Satisfaction: age, prior learning, resilience, and agreeableness; and four for Compassion Fatigue: attitudes of avoidance and escape concerning death, neuroticism, and openness.
Conclusions:
The high relationship found between training and resilience with Compassion Satisfaction can serve as a guide for academic and health care institutions to orient training, preventive and interventional strategies to provide oncology nursing teams with resources that allow them to optimize their care role.
Keywords: Compassion Satisfaction; Compassion Fatigue; oncology nursing; resilience; attitudes towards death; personality
INTRODUCTION
Caring for suffering people is a very complex task, not only because of the technical nature of many of the procedures required but because of the enormous emotional investment made by the people who take care of them, especially when the suffering is pronounced and health improvement is uncertain or scarce. At the beginning of the last century, McDougall defined the emotion of tenderness and compassionate pain as responses that could appear in care professionals when faced with the perception of intense negative emotion in patients1. Despite this, the emotional impact that the care process has on nursing staff has long been assumed to be natural2. This fact has facilitated the postponement of the study of its effects on the personal and professional well-being of nurses until the appearance of the term “compassionate fatigue”3, which was later included within the Quality of Professional Life construct4.
Stamm 4 defined Professional Quality of Life as “the quality one feels in relation to one's work as a helper” (p. 8) and developed an instrument called the Professional Quality of Life Scale (ProQOL, currently, in version V) to measure it. This construct both encompasses positive experiences-resulting from perceiving that helping itself, is worthwhile (compassion satisfaction, henceforth CS)-and negative experiences-which include burnout syndrome at work and secondary traumatic stress, with symptoms comparable to the posttraumatic stress disorder (PTSD). These last two dimensions make up compassion fatigue. However, the literature refers to CS, burnout, and compassion fatigue, the last one being understood as secondary traumatic stress (hereinafter CF/STS). Taking into account that research on burnout is more extensive, the present study focuses on the analysis of CS and CF/STS, intending to increase the understanding of the two processes.
CF/STS, together with CS, seem to be exclusive of those professions characterized by the establishment of a helping relationship between professionals and patients and can be understood as a consequence of contact with the traumatic experiences of suffering people. Circumscribed to the field of nursing, it has been defined as "a cumulative and progressive process of absorption of the patient's suffering, formed from the sympathetic and caring interactions (...), with consequences so extensive that they threaten the existential integrity of the nurse"5 (p. 43). Moreover, the literature reflects a profile of a professional who is more prone to develop CF/STS6 and describes a state of greater physical and emotional vulnerability, as well as a decrease in the effectiveness and efficiency of the care provided, a reduction in the capacity to empathize, and a greater risk of leaving the profession or changing units in those professionals who are at high risk or who, in fact, develop CF/STS7,8.
Thus, nursing staff has been frequently studied in this field, especially the group of professionals who provide care in oncological areas9,10,11,12. Although studies at the international level are quite abundant, in Spain, just a few of them have been carried out using the ProQOL to assess the perception of professional quality of life. Sansó13 tried to establish, among other things, the relationship between coping skills and the three dimensions of professional quality of life in a sample of 387 professionals belonging to the Spanish Society of Palliative Care. The data reflect moderate-to-high levels of CS in 95.7% of the sample, whereas 79.5% obtained moderate-to-high scores of CF/STS. The study does not provide data differentiated by profession, but it does support the hypothesis that adequate coping with death predicts CS positively and CF/STS negatively. Buceta14 studied CS and burnout in a multidisciplinary sample of 480 healthcare professionals, in which nursing staff represented 39.6% of the total. Results indicated higher CS among technicians in auxiliary care of nursing. Vocation, satisfaction with the role of care, self-efficacy, and burnout were the main predictors of CS. Finally, Arimon-Pagès et al.9 studied the relationship between CS and CF/STS in a sample of 297 nurses in cancer units in Catalonia. The data show that 81.8% had moderate-to-high CS, whereas 88.6% obtained moderate and high scores in SC/STS.
Stamm4 defended that the healthcare staff’s perception of their professional quality of life is built around the characteristics of the work environment, their own personal characteristics, and the exposure to primary and secondary traumas at work. Therefore, it seems interesting to explore and analyze the relationship between CS and CF/STS dimensions and different adaptive and personality variables. Thus, some studies have contemplated, among others, resilience as a necessary mediator in CS and CF/STS, concluding that more resilient people would present less negative psychological symptoms and higher CS15. On the other hand, given the high presence of the possibility of death in oncological areas, it seems logical that nurses’ attitudes toward death will condition the emotional value they attach to their caregiver role. In this sense, some studies have explained the high prevalence of the death-avoidance dimension, taking into account professionals’ need to build a protective barrier against emotional impact16. Finally, if the relationship between personality traits and CS-CF/STS is considered, positive correlations have been established between CS and traits of extraversion, responsibility, and friendliness, as well as between CF/STS and neuroticism, and openness17,18.
Determining which factors lead to CF/STS can help to develop interventions that prevent it, and also promote strategies to strengthen CS. Thus, the main contribution of this research work lies in generating an approach to predictive models of CF/STS and, above all, of CS. This interest is sustained by the conviction that people who derive gratification from their role as caregivers connect better with patients and families, and understand their situation more deeply and respectfully. Also, they are more capable of developing optimal therapeutic alliance processes, thus increasing patients’ adherence to treatment, and they acquire higher levels of commitment to the profession, improving staff retention14,19.
Hence, the objectives of this research are (1) to explore the CS and CF/STS of oncology nursing staff of Biscay, in the Basque Health Service, and possible differences according to sex, age, and professional variables (professional category, previous training, and job tenure); (2) to analyze the relationship between CS and CF/STS and resilience, attitudes toward death, and personality; and (3) to obtain a predictive model for the two constructs.
MATERIAL AND METHODS
A descriptive, correlational, cross-sectional, study was carried out. A convenience sample of 110 professionals (65.09% of the staff) was recruited from the Oncology Nursing staff of the Basurto and Cruces University Hospitals, both belonging to the Basque Health Service, geographical demarcation of Biskay.
The investigation followed the ethical values required in research with human beings, respecting the fundamental principles included in the Declaration of Helsinki: the right to information, protection of personal data and guarantees of confidentiality, non-discrimination, free of charge, voluntary and the possibility of leaving the study at any stage. Ethical approval was obtained from the Basque Country Research Ethics Committee (CEIm-E PI2018066), and permission was also obtained from the Nursing Managers of each hospital. Information on the project was provided through numerous meetings held with the target population of the study and was reinforced through a letter attached to the dossier of assessment tests. The dossiers were distributed in the selected units, along with the pertinent instructions for completing the tests, which were self-applied and anonymous. Once completed, they were placed in an opaque, closed urn. Since its collection, the evidence was appropriately guarded and was not used for any other purpose than the original one. Data collection covered the period from September 2018 to March 2019. All scales and assessment instruments, listed below, have adequate psychometric properties.
Professional Quality of Life: Compassion Satisfaction and Fatigue Subscales V (ProQOL V)4, in its translated version in Spanish20. This multidimensional assessment system consists of 30 items that are rated on a five-point Likert-type scale ranging from 1 (Never) and 5 (Very frequently). Items are distributed in three scales: Compassion Satisfaction (e.g., "I like my work as a helper"), Compassion Fatigue (e.g., "I find it difficult to separate my personal life from my life as a helper"), and Burnout (e.g., "I feel worn out because of my work as helper"). The test allows for the categorization of scores into high, medium, and low levels, as well as offering mean scores for comparison. Cronbach's alpha values obtained in this study were α = .88 for CS and α = .83 for CF/STS.
Connor and Davidson Resilience Scale, simplified version (CD-RISC)(21), in its Spanish version22. This 10 item-scale, which provides a global measure of resilience, is rated on a five-point Likert scale ranging from 0 (Disagree) to 4 (Fully agree). Some examples are: "I can adapt to change," "I can maintain concentration under pressure," or "I manage to achieve my goals despite difficulties." The Cronbach alpha obtained in this study for this one-dimensional test was α = .89.
Death Attitude Profile-Revised (DAP-R)23, in its validated Spanish version24. This is a 32-item multidimensional scale of attitudes toward death, which is rated on a seven-point Likert scale, ranging from 1 (Totally Disagree) to 7 (Totally agree). It has five factors: Fear of Death (e.g., "The uncertainty of not knowing what happens after death worries me"), Death Avoidance (e.g., "I avoid thinking about death altogether"), Neutral Acceptance (e.g., "Death is simply a part of the process of life"), Approach Acceptance ("I see death as a passage to an eternal and blessed place"), and Escape Acceptance (e.g., "I see death as a relief from the burden of life"). Cronbach's alpha obtained in this study for the total test was α = .84. By scales, it was α = .82 for Fear of Death, α = .81 for Death Avoidance, α = .60 for Neutral Acceptance, α = .94 for Approach Acceptance, and α = .81 for Escape Acceptance.
NEO Five-Factor Inventory (NEO FFI 3)25, in its validated version in Spanish26. This is a multidimensional personality assessment system, consisting of 60 items, rated on a five-point Likert scale, ranging from 0 (Disagree) to 4 (Totally agree). It contains five factors: Neuroticism, Extraversion, Openness, Agreeableness, and Conscientiousness. Some sample items are "I often feel inferior to others," "I tend to think the best of people," or "I enjoy talking to people." Cronbach's α obtained in this study for the total test was α = .73. By scales, it was α = .83 for Neuroticism, α = .85 for Extraversion, α = .75 for Openness, α = .72 for Agreeableness, and α = .76 for Conscientiousness.
Ad-hoc questionnaire to collect information about participants’ sociodemographic and professional profile, including data related to gender, age, professional category, prior training related to the subject of bereavement, death and/or palliative care, and job tenure in the field of care.
Data were analyzed using the IBM SPSS Statistics 22.0 statistical package. Firstly, contingency tables with chi-square tests were calculated for sociodemographic and professional variables, and means comparisons were performed with Student’s t-test to compare CS and CF/STS as a function of the sociodemographic (gender and age) and professional characteristics of the sample: professional category (nurse vs. auxiliary care technician), job tenure (more or less than 5 years), and prior training (with or without prior training). Secondly, Pearson correlation analyses were performed to determine the relationship between the CS and CF/STS dimensions and other adaptive and personality variables. Finally, a predictive model of CS and CF/STS was obtained through multivariate logistic regression analysis, following the intro method. The CS and CF/STS variables were contemplated dichotomously, rejecting the low level of CS and high level of CF/STS, based on their n = 1.
RESULTS
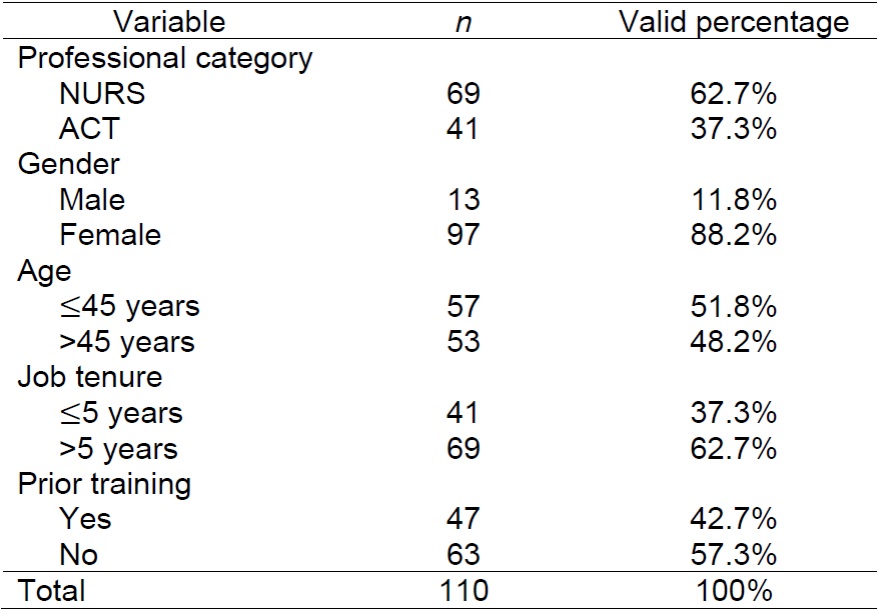
Concerning professional category, 62.7% (n = 69) of the sample was working as a nurse (hereinafter NURS), and the remaining 37.3% (n = 41) were Auxiliary Nursing Care Technicians (hereinafter ACT). In terms of gender, 88.2% (n = 97) were women. Concerning age, initially, three ranges were established (18-25, 26-45, 46-65 years). However, the lowest range registered a very low percentage of participants, so we decided to convert the variable into a dichotomous one (18-45, 46-65), establishing the cut-off point at 45 years, to balance the sample and optimize statistical analyses. Thus, 51.8% (n = 57) of the professionals were under 45, and 48.2% (n = 53) were over 45. It is interesting to note the younger age of NURS versus ACT, with 66.7% (n = 46) of NURS versus 26.8% (n = 11) of ACT under 45 years, with the difference being statistically significant, χ2(1)= 16.35, p < .001. Thus, the probability of being younger than 45 years is 5.46 times higher among NURS than among ACT (95% CI [2.32, 12.80]).
Taking into account job tenure, 62.7% (n = 69) of the sample had worked in the care setting for more than 5 years, χ2(1) = 18.01, p < .001, and the older they were, the more years they had worked (OR = 6.26, 95% CI [2.58, 15.0]). Finally, 42.7% (n = 47) had had specific training in bereavement, death, and/or palliative care. The characteristics of the study sample are presented in Table 1.
Descriptive analysis of CS (M = 42.90 ± 5.45) reflected that practically all the participants (99.9%, n = 109) positively experienced their healthcare role; among them, 66.4% (n = 73) obtained high CS scores Concerning CF/STS (M = 22.51 ± 5.59), 57.3% (n = 63) of the professionals presented low levels and 41.8% (n = 46) had moderate levels of CF/STS.
Student’s t-test results comparing CS and sociodemographic and professional variables did not yield significant differences for professional category, t(108) = -.94, p = .347; gender, t(108) = -.20, p = .842; age, t(108) = 1.01, p = .317; or professional experience in the field of care, t(108) = -.73, p = .468. Only specific training in death and/or bereavement issues showed statistically significant differences [t(108) = 2.76, p = .007], sucho that those who had prior training in this area perceived themselves more satisfied than those who did not have such training.
No statistically significant differences were found between the CF/STS dimension and any variable: professional category, t(108) = -.43, p = .671; gender, t(108) = .60, p = .55; age, t(108) = -.07, p = .945; care experience, t(108) = -.45, p = .652; prior training, t(108) = -1.14, p = .258.
Person´s coefficient showed positive significant relationships between CS and CF/STS and some variables, as shown in Table 2. For SC, positive correlations were established with Resilience (r = .55), Neutral Acceptance of death ( r = .24), and the personality traits of Extraversion (r = .55), Openness (r = .27), Agreeableness (r = .37), and Conscientiousness (r = .33). CS correlated negatively with CF/STS (r = -.34), Death Avoidance (r = -.21), and Neuroticism (r = -.40).
CF/STS correlated positively with Fear of Death (r = .44), Death Avoidance (r = .32) and Neuroticism (r = .60), and negatively with CS (r = -.34), Resilience (r = -.55), Neutral Acceptance of death (r = -.24), and rgw personality traits of Extraversión (r = -.37), Agreeableness (r = -.33), and Conscientiousness (r = -.30).
Table 2: Correlations among variables
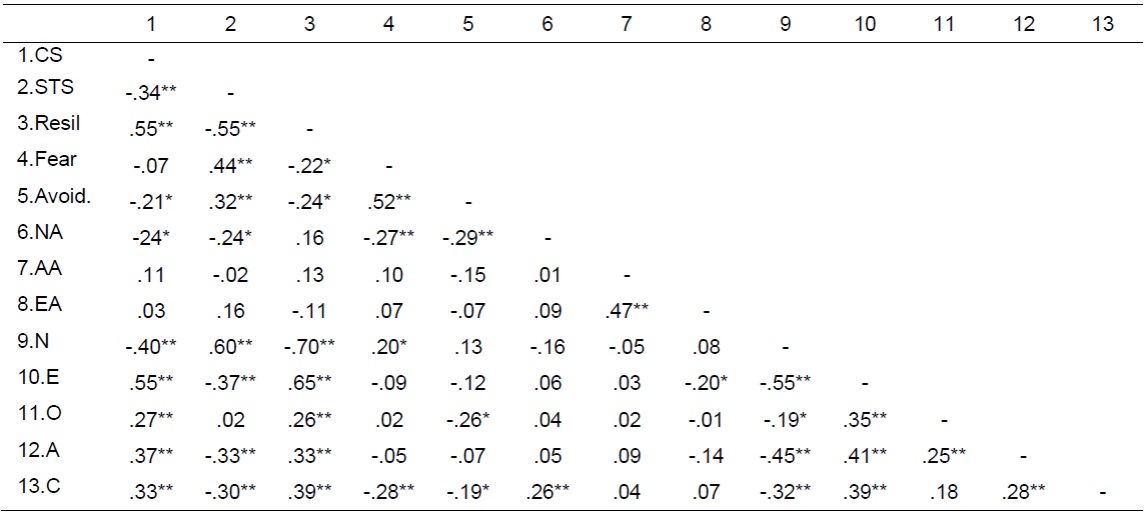
Note: ** significant at level .01; * significant al level .05; Resil. = Resilience; Fear = Fear of Death; Avoid. = Death Avoidance; NA = Neutral Acceptance; AA = Approach Accpeptance; EA = Escape Acceptance; N = Neuroticism; E = Extraversión; O = Openness; A = Agreeableness; C = Conscientiousness
Finally, independent predictors of high CS and moderate CF/STS were extracted through a multivariate logistic regression analysis. For CS, four factors were included in the final model (see Table 3), which explained 34.7% of the variance, according to the Nagelkerke index. The model had acceptabe fit and its percentage of correction classification was 76.1%, establishing the cut-off point at .60.
Table 3: Predictive models for high CS
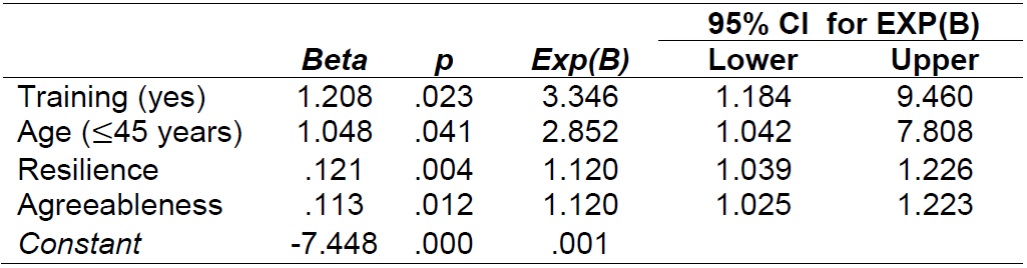
Note: R2 = .63 (Hosmer-Lemeshow), .25 (Cox & Snell), .35 (Nagelkerke).
Model x2(4) = 31.23, p < .001.
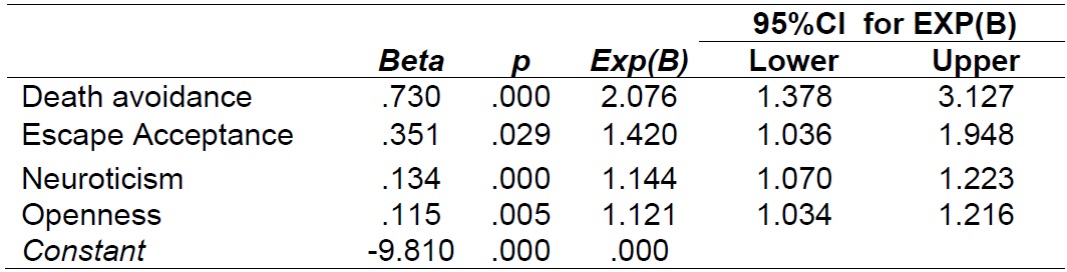
For moderate CF/STS, four independent predictors were identified, explaining 39.9% of the variance, according to Nagelkerke's index (see Table 4). The model's goodness of fit was satisfactory, and the percentage of correct predicts was 75.9%, with the cut-off point set at .50.
DISCUSSION
To care for others properly, one must be well. It is therefore important to know the perception of the Professional Quality of Life of the nursing staff who assist suffering people. However, to date, this is the first study carried out in the Basque Health Service that aims to measure and provide evidence of the importance of CS, as well as of CF/STS in oncology nurses and auxiliary care technicians.
CS and CF/STS levels obtained in this sample are higher than those reported in other studies11 and very similar to those of Wu et al.10 with American and Canadian populations. In contrast to similar studies9,12,20, the studied sample presents higher levels of CS and lower levels of CF/STS. Data obtained show the relationship between the two constructs studied, as reflected by Stamm4 in her conceptual model, defending the compatibility of the perceptions. In fact, the high levels of CS found in the sample under study reflect professionals’ high capacity to extract positive meaning from their role of care, enjoy the assistance provided and the esteem they feel for the patients and families, despite the emotional burden of caring for suffering people. However, when CF/STS increases, professionals’ capacity to develop CS may break down, leading to a worse perception of personal well-being and a decrease in the effectiveness and efficiency of care. Coupled with the relationship between CF/STS and the intention to leave the profession or change the work unit, it is necessary to interpret the obtained data with some caution, as nearly 5 out of 10 people in this study are at risk of developing CF/STS.
Most of the sample was composed of women, which is not surprising, given that, historically, women, more than men, have been responsible for the task of caring. However, none of the sociodemographic or professional variables considered were decisive in establishing significant differences between CS and CF/STS levels, except for the fact of having prior training in death, bereavement, and/or palliative care. Specific training was associated with higher levels of CS, supporting the importance of providing healthcare staff not only with technical but also with attitudinal and emotional resources, as also concluded by other researchers15.
On another hand, the high correlation found between resilience and CS and CF/STS suggests that health professionals with more personal resources to give meaning to their own or others´ traumatic events will feel more emotional gratification from caring and will develop less fatigue. Accordingly, the correlations established with neuroticism support the idea that people with greater emotional instability tend to present higher levels of CF/STS, as well as lower levels of CS, a conclusion also observed in the literature17,18. The attitude of death avoidance also requires some reflection. People who consider death as part of the natural process of life will present higher levels of CS. Conversely, those who fear death or avoid thinking about it or approaching people immersed in the process of dying will reflect higher CF/STS levels. These data again reinforce the importance of training nursing professionals in understanding the process of dying, as a basic strategy for managing emotional impacts.
Finally, one of the major goals of this study was to outline a predictive model of CS and CF/STS for oncology nursing staff. The independent factors that explain higher CS are being younger than 45 years old, having prior training related to death and/or grief, being resilient, and high agreeableness as a personality trait. Consistent with reported data, the presence of resilience as a predictive factor reveals the need for health professionals to acquire and develop personal resources to manage potentially stressful situations, thus compensating for their possible vulnerability to the emotional impact of others’ suffering. As a consequence, the fact that nursing staff can overcome, learn from, and be strengthened from the process of accompanying people who are suffering, together with a predisposition to help, will allow them to adapt their actions and offer quality care with warmth. The findings are consistent with those outlined by Frey15, who found that high levels of resilience and specific training in palliative care became predictors of CS among nurses. The resulting model, which explains moderate CF/STS, includes avoidance and escape approach attitudes toward death, and neuroticism and openness within the personality traits. If the care-taker has difficulties to face thoughts about death, they will probably feel greater discomfort in the process of accompanying people with a high degree of suffering, thus putting at risk their perception of professional quality of life. According to the study by Yu et al. 11, professionals with emotional instability, who are reactive to external circumstances and have emotion self-regulation difficulties after high-impact events such as the suffering and death of the people they assist will be the most likely to develop CF/STS. Focus on suffering and concern about possible inefficiency in the accompaniment task, plus difficulties in attaching meaning to suffering and dying, could promote oncology nursing staff’s highlighting the emotionally most negative aspects of a profession made for people (Flinton)27.
Limitations
There are several limitations to this study. On the one hand, the type of research. As in all cross-sectional studies, it was not possible to assess changes over time or to establish the direction of causality. For example, highly resilient people may be more concerned about training in the area of death and bereavement to offer better quality care, but the fact of receiving training in this area may also favor more resilient attitudes in healthcare professionals. A second limitation has to do with the sample size and its selection such that the results obtained are only descriptive of oncology nursing staff in the Basque Health Service of Biscay.
CONCLUSIONS
Knowing how CS and CF/STS interact with different sociodemographic, professional, and adaptive variables has interesting practical implications, helping to guide training, preventive, and intervention strategies of academic and healthcare institutions. Thus, already at the preparatory stage, it would be possible to provide nursing professionals with personal resources to deal optimally with the challenges associated with the nursing profession. Once in active care, knowing the basic profile that helps to predict which characteristics will make a person more likely to develop CS or CF/STS would allow institutions to implement preventive and/or intervention strategies to optimize the perception of professional quality of life, strengthening Compassion Satisfaction and minimizing and counteracting the possible onset of Compassion Fatigue.
This is the first study carried out on nursing professionals in Spain that attempts to provide a positive and not a merely preventive approach. Taking into account the results obtained in this research, it seems appropriate to focus on training in death and/or bereavement and resilience. Given that the great value of any care system lies in the people who make care possible, investing in the acquisition of effective coping resources would strengthen professionals’ resilience and optimal management of emotions. This learning would consequently favor their degree of enjoyment and satisfaction with the caring role, which will undoubtedly have a positive impact on the quality of the care provided.
Therefore, there are several possible lines of research for future studies: (1) firstly, it would be interesting to contrast the results obtained in professionals from different care areas, to expand the sample and to provide a multi-center viewpoint to the study, thus developing predictive models; (2) to elaborate and evaluate the impact of training programs that influence the meaning of and approach to grief, death, palliative care, and accompaniment, promoting attitudes of acceptance of these processes; (3) finally, to elaborate and evaluate training programs that facilitate an appropriate approach to potentially stressful and emotionally disturbing situations.
REFERENCIAS
1. McDougall W. Some general or non-specific innate tendencies. In: McDougall W, editor. An introduction to Social Psychology [Internet]. Boston: John W. Luce and co.; 1926. p. 93-124. Available from: http://www.open.edu/openlearn/health-sports-psychology/psychology/critical-social-psychology?track=5 [ Links ]
2. Secor CM. Compassion fatigue: A concept analysis. Sophia, the St. Catherine University, St. Paul, Minnesota; 2015. [ Links ]
3. Figley CR. Compassion fatigue as secondary traumatic stress disorder: An overview. In: Figley CR, editor. Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized. Philadelphia, PA, US: Brunner/Mazel; 1995. p. 1-20. [ Links ]
4. Stamm BH. ProQOL Concise Manual, 2nd Edition [Internet]. 2010. Available from: http://www.proqol.org/uploads/ProQOL_Concise_2ndEd_12-2010.pdf [ Links ]
5. Sabery M, Hosseini M, Zagheri Tafreshi M, Mohtashami J, Ebadi A. Concept development of "compassion fatigue" in clinical nurses: Application of Schwartz-Barcott and Kim's hybrid model. Asian/Pacific Isl Nurs J 2017;2(1):37-47. [ Links ]
6. Sorenson C, Bolick B, Wright K, Hamilton R. Understanding compassion fatigue in healthcare providers: A review of current literature. J Nurs Scholarsh. 2016;48(5):456-65. [ Links ]
7. Cross LA. Compassion Fatigue in Palliative Care Nursing. A concept analysis. J Hosp Palliat Nurs [Internet]. 2018;21(1):21-8. Available from: http://insights.ovid.com/crossref?an=00129191-900000000-99973 [ Links ]
8. Sorenson C, Bolick B, Wright K, Hamilton R. An evolutionary concept analysis of Compassion Fatigue. J Nurs Scholarsh. 2017;49(5):557-63. [ Links ]
9. Arimon-Pagès E, Torres-Puig-Gros J, Fernández-Ortega P, Canela-Soler J Emotional impact and compassion fatigue in oncology nurses: Results of a multicentre study. Eur J Oncol Nurs [Internet]. 2019;43(March):101666. Available from: https://doi.org/10.1016/Jejon.2019.09.007 [ Links ]
10. Wu S, Singh-Carlson S, Odell A, Reynolds G, Su Y. Compassion fatigue, burnout, and compassion satisfaction among oncology nurses in the United States and Canada. Oncol Nurs Forum. 2016;43(4):E161-9. [ Links ]
11. Yu H, Jiang A, Shen J Prevalence and predictors of compassion fatigue, burnout and compassion satisfaction among oncology nurses: A cross-sectional survey. Int J Nurs Stud [Internet]. 2016;57:28-38. Available from: http://dx.doi.org/10.1016/Jijnurstu.2016.01.012 [ Links ]
12. Duarte J, Pinto-Gouveia J The role of psychological factors in oncology nurses' burnout and compassion fatigue symptoms. Eur J Oncol Nurs [Internet]. 2017 Jun 1 [cited 2018 Nov 8];28:114-21. Available from: https://www.sciencedirect.com/science/article/pii/S1462388917301229 [ Links ]
13. Sansó N, Galiana L, Oliver A, Pascual A, Sinclair S, Benito E. Palliative care professionals' inner life: Exploring the relationships among awareness, self-care, and compassion satisfaction and fatigue, burnout, and coping with death. J Pain Symptom Manage. 2015;50(2):200-7. [ Links ]
14. Buceta MI, Bermejo JC, Villacieros M. Enhancer elements of compassion satisfaction in healthcare professionals. An Psicol 2019;35(2):323-31. [ Links ]
15. Frey R, Robinson J, Wong C, Gott M. Burnout, compassion fatigue and psychological capital: Findings from a survey of nurses delivering palliative care. Appl Nurs Res [Internet]. 2018;43:1-9. Available from: https://doi.org/10.1016/Japnr.2018.06.003 [ Links ]
16. Braun M, Gordon D, Uziely B. Associations between oncology nurses' attitudes toward death and caring for dying patients. Oncol Nurs Forum [Internet]. 2010;37(1):E43-9. Available from: http://onf.ons.org/onf/37/1/associations-between-oncology-nurses-attitudes-toward-death-and-caring-dying-patients [ Links ]
17. O'Mahony S, Ziadni M, Hoerger M, Levine S, Baron A, Gerhart J Compassion fatigue among palliative care clinicians: Findings on personality factors and years of service. Am J Hosp Palliat Med 2018;35(2):343-7. [ Links ]
18. Chen YP, Tsai JM, Lu MH, Lin LM, Lu CH, Wang KWK. The influence of personality traits and socio-demographic characteristics on paediatric nurses' compassion satisfaction and fatigue. J Adv Nurs. 2018;74(5):1180-8. [ Links ]
19. Sacco TL, Copel LC. Compassion satisfaction: A concept analysis in nursing. Nurs Forum. 2018;53:76-83. [ Links ]
20. Galiana L, Arena F, Oliver A, Sansó N, Benito E. Compassion Satisfaction, Compassion Fatigue, and Burnout in Spain and Brazil: ProQOL Validation and Cross-cultural Diagnosis. J Pain Symptom Manage. 2017;53(3):598-604. [ Links ]
21. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019-28. [ Links ]
22. Notario-Pacheco B, Solera-Martínez M, Serrano-Parra MD, Bartolomé-Gutiérrez R, García-Campayo J, Martínez-Vizcaíno V. Reliability and validity of the Spanish version of the 10-item Connor-Davidson Resilience Scale (10-item CD-RISC) in young adults. Health Qual Life Outcomes [Internet]. 2011;9(1):63. Available from: http://www.hqlo.com/content/9/1/63 [ Links ]
23. Wong PT, Reker GT, Gesser G. Death Attitude Profile-Revised: A multidimensional measure of attitudes toward death. In: Neimeyer RA, editor. Death Anxiety Handbook Research, Instrumentation, and Application. Washington, DC: Taylor & Francis; 1994. p. 121-48. [ Links ]
24. Schmidt-Riovalle J Validación de la versión española de la Escala de Bungen de Afrontamiento de la Muerte y del Perfil Revisado de Actitudes hacia la Muerte: Estudio comparativo y transcultural. Puesta en marcha de un programa de intervención [Internet]. Univerdidad de Granada: Granada; 2007. Available from: http://www.journals.cambridge.org/abstract_S1041610200006906 [ Links ]
25. McCrae RR, Costa, Jr. PT. Brief Version of the NEO-PI-3. J Individ Differ [Internet]. 2007;28(3):116-28. Available from: http://econtent.hogrefe.com/doi/abs/10.1027/1614-0001.28.3.116 [ Links ]
26. Cordero A, Pamós A, Seisdedos N. Inventario de Personalidad Neo Revisado (NEO PI-R). MAdrid: TEA ediciones; 2008. [ Links ]
27. Flinton DM, Cherry P, Thorne R, Mannion L, O´Sullivan C, Khine R. Compassion satisfaction and fatigue: An investigation into levels being reported by radiotherapy students. J Radiother Pract. 2018;17(4):364-7. [ Links ]
Received: March 04, 2020; Accepted: July 04, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
