










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.20 n.64 Murcia Oct. 2021 Epub Oct 25, 2021
https://dx.doi.org/10.6018/eglobal.474161
Originals
Assessment of Quality of Life in Multiple Sclerosis through the MSQOL-54 and its relation to the health of the caregiver
1. Universidad de Murcia. España. liminana@um.es
2. Hospital Clínico Universitario Virgen de la Arrixaca. Murcia. España.
Objective:
The aim of the present study was to evaluate the health-related quality of life (HRQoL) in patients with Multiple Sclerosis (MS) through the MSQOL-54 questionnaire and to analyse its relationship with the health of primary caregivers through the GHQ-12 questionnaire and a questionnaire on self-perceived physical health.
Materials and Methods:
A total of 115 subjects diagnosed with MS and 79 primary caregivers were evaluated.
Results:
The results obtained show the significance of effects on HRQoL of patients with MS and its relationship to the health of primary caregivers. Significant relationships were found between the physical and mental health of the person with MS and an increased number of illnesses, poorer mental health and lower self-perception of health in the caregiver.
Conclusions:
The results obtained point to the significant impairment of the HRQoL of people with MS, and its direct relationship with the health of primary caregivers.
Keywords: multiple sclerosis; quality of life; health-related quality of life; caregivers; mental health
INTRODUCTION
Multiple sclerosis (MS) is a clinically highly heterogeneous, progressive and unpredicTable autoimmune disease which impacts greatly on the quality of life of patients and their families1. Numerous studies agree that its negative effects are more intense than with any other chronic disease and that they worsen in at least a third of patients after diagnosis2. For a person with MS, quality of life is the result of the interaction of many factors, such as the type of disease and its evolution, the stage in which the disease occurs, the personality of the sufferer and their ability to adapt to the disease, the intensity with which it affects their environment and changes their life, or the social support they perceive, among others3.
The application of the concept of quality of life in the field of health leads to the term "health-related quality of life" (HRQoL), and encompasses most specifically the physical, emotional and social aspects of health4. With regard to the physical domain, the principal factors identified as relevant in the HRQoL of the person with MS are those that cause functional disability (motor or sensory alterations), fatigue, pain and sexual or urinary problems. In the emotional or psychological domains, of note are factors such as anxiety, depression, loss of cognitive functions, or attitude towards the disease5. With regard to the social domain, of relevance are the stigmatization that the pathology produces in the patient's social network, the loss of friendships and relationships due to lack of adaptation to the new situation, and possible negative repercussions in the person's working life6.
The measuring of HRQoL is considered fundamental in MS patients, as it facilitates the assessment of the impact the condition has on the person concerned. This helps to the identify the patient’s needs; to predict the impact of the condition on the physical and psychological domains of their quality of life and, through periodical evaluation, to assist in the identification of possible changes and to optimise treatment. In recent years, various studies have highlighted the impact of MS on HRQoL, not only in patients, but also in their caregivers, indicating the importance of research into the relationship between these two measurements8,9.
The purpose of this study is to obtain an adequate measurement of HRQoL in people with MS and of the health of primary caregivers in order to analyse the relationship between the two. The aim is to confirm the main repercussions of this disease and to offer new evidence to assist in the development of actions that are effective both in prevention and in improvement of HRQoL of MS patients and the health of caregivers. For this, two objectives are considered: a) to evaluate the physical and mental HRQoL of people with MS using a specific measurement tool for the disease, and b) to explore the health of caregivers and its relationship with HRQoL of MS sufferers.
METHOD
The prevalence of MS in the region of Murcia has been estimated at 88 cases / 100,000 inhabitants10. The study sample consisted of 115 people with a diagnosis of MS, of whom 30 were from the Multiple Sclerosis Association of the Region of Murcia and 85 from the Multiple Sclerosis Unit of the Virgen de la Arrixaca University Clinical Hospital in Murcia (HCUVA), and a sample of 79 informal caregivers from the aforementioned Multiple Sclerosis Unit of the HCUVA. Of those diagnosed with MS, 70.4% (n = 81) were women and 29.5% (n = 34) were men; in the group of caregivers, 57% (n = 45) were women and 43% (n = 34) men. Participants were selected using purposive sampling or convenience sampling, over approximately 12 months, from January 2013 to January 2014.
All participants received comprehensible and sufficient information provided by those responsible for the project, approved by the Ethics Commission of the University of Murcia. Their participation was voluntary and they signed an informed consent.
Participants with MS completed two questionnaires:
A brief Questionnaire on sociodemographic and clinical variables, in which data related to the disease and the degree of disability were collected (according to Spanish law RD 1856/2009, of December 4th) and subsequently completed with the data from their medical records.
The Multiple Sclerosis Quality of Life-54 questionnaire (MSQOL-54)11, Spanish version12, a multidimensional measurement of HRQoL combining generic and specific elements regarding MS. This consists of 54 Likert-type items that assess intensity or frequency reported in the previous four weeks. The total score for each dimension ranges from 0 to100, where a higher value indicates improved HRQoL. Two subtotals are obtained from the scores of each dimension, corresponding to two scales: Mental Health and Physical Health. The 12 subscales of the tool show good internal consistency, with Cronbach's alphas ranging from 0.75 to 0.96. The test-retest reliability for these 12 subscales is also correct, with intraclass correlation coefficients ranging from 0.66 to 0.96. The internal consistency values in the sample under study were good (α = 0.783).
The caregivers first completed a questionnaire on sociodemographic and care variables, with high internal consistency for our sample (α = 0.87), and several health measures:
The General Health Questionare-12 (GHQ-12)13, a screening and detection tool for psychological distress, validated for the Spanish adult population by Sánchez-López and Dresch14. This consists of 12 Likert-type items each with four response options (0-1-2-3), with a range of 0 to 36 points, where scores over 16 were considered indicative of psychological issues. The internal consistency of this measure in the Spanish population as a whole is α = 0.76, whilst in the sample under study a value of α = 0.89 was recorded.
A questionnaire on self-perceived physical health (Likert scale of 5 points where 1 = very good and 5 = very bad), with an internal consistency of α = 0.87 for our sample, and another regarding the number of health issues (28 ailments or diseases). Both questionnaires are based on the health indicators of the Spanish National Health Survey15.
Two procedures were followed for data collection. Initially, this was done in the Multiple Sclerosis Association of the Region of Murcia, through ordinary mail, a slow process in which 30 of the 60 questionnaires distributed were collected. Subsequently, data collection was carried out in the Multiple Sclerosis Unit of the Virgen de la Arrixaca University Hospital in Murcia, a unit of regional and national reference, with an approximate annual average of 700 patients treated. The procedure consisted of the distribution of the questionnaires directly to the volunteer participants, thanks to the collaboration of the professionals in the Unit.
A descriptive and correlational design was made, using the SPSS statistical package, version 22. Descriptive statistics were used and separated according to sex, given the relevance of gender considerations in research carried out in health contexts16. The t statistic and the F statistic were used to compare means based on sex, age, educational level, employment status and marital status, and Pearson's r statistic was used to find the sense and significance of the relationship between HRQoL variables of people with MS and clinical and health-related variables of caregivers.
RESULTS
Table 1 shows the total descriptive statistics by sex for the demographic variables in the 115 patients with multiple sclerosis and the 79 primary caregivers.
Table 1. Descriptive statistics of people with MS and of primary caregivers

a. mean ± standard deviation of time in years
Table 2 presents the descriptive statistics for the scores of the subscales that make up the MSQOL-54 and the results of the comparison of means based on sex. The results in Total Physical Health, with a mean total score of 53.4 over 100, indicate that the participants in our sample have a moderate Physical HRQoL and that the subscale with the lowest scores is that relating to physical limitations caused by the disease. Regarding Mental HRQoL, with an average total score of 57.18, the subscale relating to cognitive function is where we see the greatest impact. No significant differences were found between men and women, neither in the total score of the Physical Health and Mental Health scales nor in any of the subscales (p>.05).
Table 2. Mean scores of the Multiple Sclerosis Quality of Life 54 (MSQOL-54) and comparison according to sex

Age was a relevant factor showing a positive relationship mainly with Physical HRQoL (see Table 3). In Total Physical Health, post hoc analyses revealed that the differences in this variable occurred between the youngest age group -20 to 30 years old- and the older groups of 41 to 50 (p =.024) and 51 to 65 (p =.000). As can be observed, the youngest group showed a higher average in Physical Health, with the difference with the rest of the groups increasing with age. The mean in the 31 to 40 group was also significantly higher than that of the 51 to 65 group (p =.020). The Physical Health subscale also presented significant results depending on age: the differences occurred between the age range of 20 to 30 years and the ranges 31 to 40 (p =.001), 41 to 50 (p =.000) and 51 to 65 (p =.000). As can be seen, the youngest group returned a higher average in this subscale, and the difference with the rest of the groups is shown to increase with age. The means in the 31 to 40 and 41 to 50 age groups were also significantly higher than that of the 51 to 65 age group (p =.000 and p =.041 respectively), but with little differentiation between the two. In Physical Limitations, there were significant differences (p <.05) depending on the age of the MS patient: the differences were observed between the 20 to 30 age group and the 41 to 50 (p =.014) and 51 to 65 (p =.001) groups, with the youngest group having a better quality of life with regard to physical limitations.
Another of the variables that showed significant differences (p <.05) according to age was the degree of pain. The results of the post hoc comparisons showed differences between the 51 to 65 age range with those of 41 to 30 (p =.033) and 20 to 30 years (p =.013). Beyond 41 years of age, no significant differences were found in quality of life with regard to the degree of pain. The youngest groups were shown to have better quality of life in this variable. Sexual Function was the last subscale of Physical Health in which significant differences were noted according to age group (p <.05). In post hoc comparisons, the 51 to 65 group differed significantly from all the other age ranges: 20 to 30 years (p =.003) 31 to 40 (p =.023), and 41 to 50 (p =.012). These groups did not differ significantly from each other. Therefore, quality of life in relation to sexual function is shown to decrease with age, although this decrease is not significant until the age of 51.
Within the subscales related to Mental Health, only marginally significant results were obtained in Overall Quality of Life between the 20 to 30-year-old group and the 51 to 65 group (p=.055)
Tabla 3. Results of ANOVAs for the scales and subscales of the MSQOL-54 according to age.

*p<.05; amarginally significant p = .055
HRQoL also presented significant differences depending on level of education (see Table 4). In Physical Health, those who had completed higher education scored better than those with only primary education (p =.000). In Mental Health, post hoc analyses revealed that the differences in this variable only occurred between those with higher education and all other levels: primary studies (p =.000); secondary studies (p =.029) and vocational training (p =.012).
Table 4. Results of ANOVAs for the scales and subscales of the MSQOL-54 according to educational level.
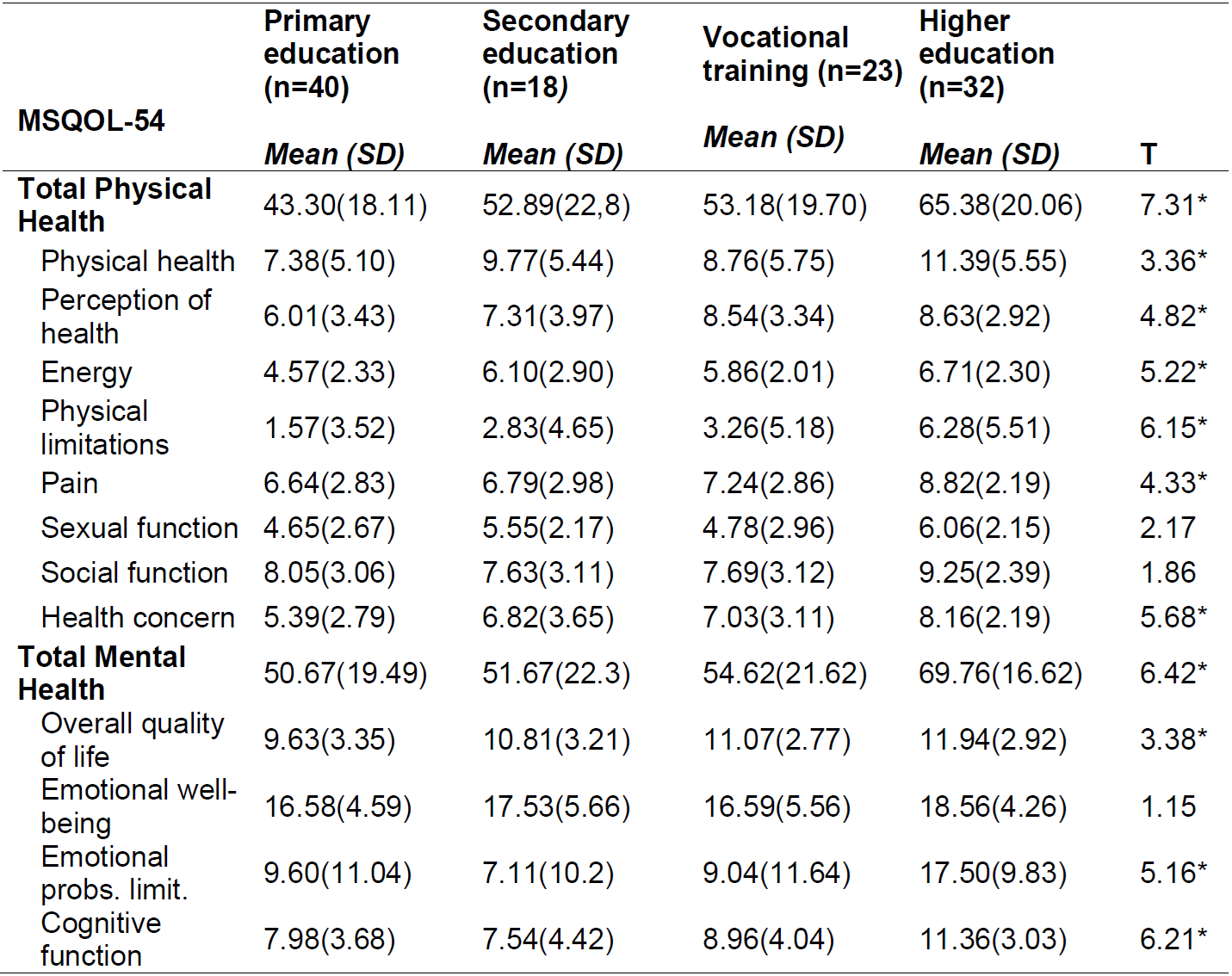
*p<.05
Employment status was shown to have a significant relationship in all outcome measures, indicating that working patients have better HRQoL in the physical and mental health aspects than those who do not work (Table 5).
Table 5. Results of the comparison of means of the scales and subscales of the MSQOL-54 according to employment status.

*p<.05, **p<.01, ***p<.001
Lastly, differences were also found in Physical and Mental HRQoL according to marital status (see Table 6). Total Physical (F111=6.54, p<.50) and Mental Health (F111=8.56, p<.05) was highest in single people, followed by married, and lowest in separated people. Post hoc analyses revealed that differences in Physical Health occurred between single and married subjects (p =.029), single and separated (p =.000), and married and separated (p =.023); and in Mental Health between the separated and single groups (p =.000), and between single and married (Mean = 56.74, p =.000).
For Total Physical Health, post hoc analyses revealed that the differences in this variable occurred across the three groups: singles with married (p =.029) and separated (p =.000), with these two groups also differing from each other (p =.023). The mean of Physical Health was highest in the singles group, followed by married, with separated being the lowest. As can be seen in Table 6, significant differences were found for all subscales according to the marital status of the patients. For the Physical Health and Pain subscales, singles differed significantly in post hoc results from married people (p =.000 and p =.005 respectively) and separated people (p =.004 and p =.015 respectively) -groups which did not differ from each other- and the quality of life in relation to these two subscales was higher among singles. In Perception of Health and Physical Limitations, significant differences were found only between single and separated people (p =.029 and p =.022 respectively), with quality of life in relation to these subscales highest among singles. In energy/fatigue, no differences were observed between single and married subjects, but there was between these two groups and the separated group (p<.000 y p<.008), with the highest results among single people.
For Total Mental Health, the post hoc differences occurred among subjects who were separated compared to those who were single (p =.000) or married (p =.000). For the Quality of Life subscale, however, the differences occurred across the three groups: single with married (p =.009) and separated (p =.000), and between married and single (p =.004). The highest mean average was in single subjects, followed by married with separated individuals the lowest. For the subscale of Emotional Problem Limitations, we again find significant differences in the post hoc analysis between separated people and both singles (p =.000) and married people (p =.000), the latter two groups showing no difference between them. Again, in the Cognitive Function subscale, differences were appeared only between separated individuals and both singles (p =.001) and married people (p =.003), with the latter two not differing from each other. These results must be interpreted with caution given the low n in the separated group.
Table 6. Results of ANOVAs for the scales and subscales of the MSQOL-54 according to marital status.

*p<.05; **p<.01; ***p<.001
Lastly, the duration of the illness was inversely related to physical health, and the degree of disability presented significant relationship to all physical health measures, except for the Pain scale, and lower levels for Mental Health measures (Table 7).
Table 7. Pearson correlations between the scales and subscales of the MSQOL-54 and length of illness and degree of disability variables in women and men with MS.
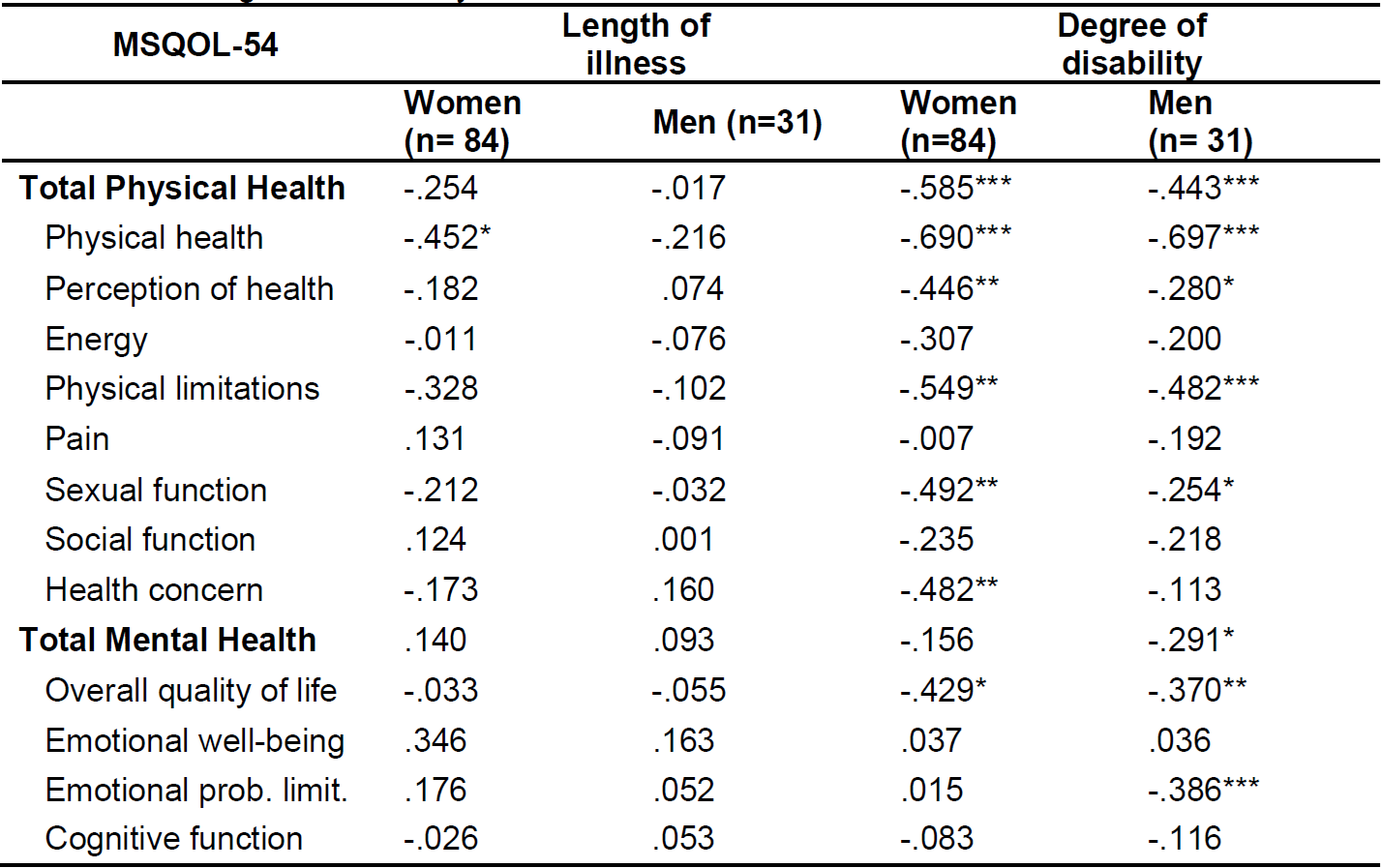
*p<.05; **p<.01; ***p<.001
Regarding the evaluation of caregivers and measurements of their health, the mean score of the total sample in the GHQ-12 was 12.89 (SD=5.49). The results showed significant differences in the GHQ-12 according to the sex of the primary caregiver [t (77) = 2.714, p =.008], the mean of women being higher (Mean = 14.29, SD= 5.88) than that of men (Mean = 11.03, SD= 4.35), that is, women were shown to have poorer mental health than men. The total scores, by sex, are significantly higher than the normative data for the Spanish version of the questionnaire14, with significant differences in the total score [t (78) = 7.06, p =.000] and in that of men [t (33) = 4.94, p =.000] and of women [t (44) = 5.68, p =.000].
With regard to self-perceived physical health, 48.7% of the sample rated their health as good, 28.2% fair, 15.4% very good, 5.1% bad and 2.6 % very bad. The level of self-perceived health considered positive in the National Health Survey15 is 80%, while in our sample of caregivers it is 64%. Female caregivers perceived poorer health than women in the general population. Only 59.1% claimed good self-perceived health, compared to 71.3% of Spanish women in general. The results for male caregivers were similar: 76.5%, compared to 79.4% for men in the general Spanish population.
Concerning the illnesses they were suffering or had suffered from, the most frequent ailments were chronic lumbar back pain (36.4%) and cervical back pain (35.1%). Other relatively frequent conditions were depression, anxiety or other mental disorders (26.9%), haemorrhoids (23.1%) and frequent migraines or headaches (21.8%).
Table 8 shows the results of the correlations between health variables and the MSQOL-54 subscales of people with MS and the health variables of female and male caregivers.
Table 8. Pearson correlations between the scales and subscales of the MSQOL-54 and health variables of the caregiver.

*p<.05 **p<.01; SP = Self-Perception of Health; NI= No. illnesses
Among the female caregivers, the results revealed significant inverse relationships between the psychological distress of the caregivers with the duration of illness, the subscales of Energy and Social Function, Total Mental Health, and the subscales of Overall Quality of Life, Emotional Well-being and Limitations due to Emotional Problems. That is, the greater the psychological discomfort of the caregivers, the lower the Physical HRQoL in the Energy and Social Function scales, and the lower the quality of life in Total Mental Health and in the subscales of Overall Quality of Life, Emotional Well-being and Emotional Problem Limitations. Self-perception of health in female caregivers was also inversely related to Physical Limitations, Total Mental Health and Emotional Problem Limitations, such that a higher self-perception of health in female caregivers resulted in improved quality of life score of people with MS on these subscales. The number of illnesses in female caregivers was directly related to the degree of disability, and inversely to the quality of life on the Physical Limitations scale. In male caregivers, direct relationships between the caregiver's psychological distress and quality of life appeared only on the Sexual Function subscale.
DISCUSSION
The results obtained confirm that the HRQoL evaluated using the MSQOL-54 is lower in people with MS than in the general population. According to data from the 2011/12 Spanish National Health Survey, regarding Health-related Quality of Life in the Spanish adult population15, the mean HRQoL score for the age range of 35 to 44 years is 81.4 over 100 points and the mean for the age range of 45 to 54 years is 77.2 over 100 points. In both age groups, HRQoL is also higher than that obtained for Physical and Mental Health in our sample. These results concur with those obtained in the study by Aymerich et al.8 on the HRQoL of patients with MS in which, according to the eight dimensions of the SF-36, this was lower in all dimensions compared to the normative data for the general population.
Our results also confirm that the HRQoL of people with MS, evaluated using the MSQOL-54, is affected on a general level, with physical HRQoL slightly more so than mental HRQoL, being related mainly to the physical limitations associated with the disease and to cognitive function respectively. No significant differences between the men and women in the sample were noted. With regard to Physical Health, the results show that the disease causes physical limitations for performing effort-intense activities such as running, climbing stairs, walking long distances, etc., and fewer limitations in carrying out those activities associated with personal autonomy, such as bathing or dressing. Other studies have indicated that in early stages of the illness, body pain and vitality are the dimensions that are most affected, and that as the illness progresses, those dimensions on the SF-36 questionnaire related to physical function are increasingly affected17. Again we see similarities with our findings, in which the patients are in an early stage and the presence of pain is considerable, limiting the performance of day-to-day physical activities, and also in the social function for carrying out standardized work activities. Similarly, Grasso et al.18 consider that the main repercussions of pain consist of the reduction of vitality, the worsening of physical function and the deterioration of mental health. With regard to cognitive function, according to the study by Amato, Ponziani, Siracusa and Sorbi19, it principally affects speed of information processing and episodic and working memory. This effect can have a marked impact on day-to-day activities, implying greater dependence for personal care, help with household tasks, a reduction of participation in social activities and increased difficulties in the workplace.
Coinciding with the results of the study by Aymerich et al.8, no differences were found in the HRQoL dimensions between men and women. However, as with the study by Alarcón et al.20, the importance that sociodemographic variables such as age, education, occupation and marital status have on HRQoL is confirmed. Age is a determining factor in the HRQoL of people with MS, with younger people, between 20 and 30 years old, having better HRQoL. Likewise, employment status, educational level and marital status were shown to relate to HRQoL of the MS patient. People with MS who work and those with a higher level of education have a better HRQoL in practically all dimensions of Physical and Mental Health. Single people also obtained a higher Physical and Mental HRQoL than married or separated people.
As was to be expected, the longer the duration of the disease, the lower the Physical HRQoL in MS patients. The degree of disability, coinciding with similar studies21, was related to reduced Physical and Mental HRQoL in almost all its dimensions, affecting physical health and quality of life in general the most, and to a lesser degree, self-perception of health, social function, energy and limitations due to emotional problems.
Regarding the health of the primary caregiver, the results found indicate this to be lower than that of the general population, with regard to both self-perceived physical health and mental health. These results are in line with previous research on health variables and psychological adaptation in caregivers22)(23)(24. Furthermore, these results are consistent with studies carried out with caregivers of patients with MS that indicate their quality of life to be lower than that of the general population6)(8)(25)(26, and that they present a higher prevalence of symptoms of anxiety and depression8)(25. The poorer health of female caregivers compared to that of male caregivers has also been identified in previous studies27)(28)(29. Our results confirm these differences in a specific sample of caregivers, underlining the importance of including gender considerations in research on the health of caregivers of patients with MS.
Regarding the relationship between the HRQoL of the person with MS and the health of caregivers, the results of the study confirm this relationship and point to different significant associations. The effect on the physical health of the person with MS and the limitations in their daily life due to the disease are associated with an increased number of illnesses in the caregiver (especially lumbar and cervical back pain, haemorrhoids, migraines or frequent headaches, depression and anxiety). Likewise, the degree of limitations due to emotional problems and those related to the sexual function of the patient are related to a poorer self-perception of health in the caregiver. Moreover, a lower degree of emotional well-being, mental health and quality of life in general in the person with MS is associated with poorer mental health in caregivers.
The results found offer new data that complement previous research on the subject, which has pointed to the importance of the relationship between the severity and physical deterioration of the person with MS and the health of the caregiver30)(31. Said research considers that treatments to delay the loss of functions of the person with MS are an essential factor not only for the patients’ HRQoL, but are also of relative importance to caregivers, for whom they also beneficial.
The limitations of the study could include the characteristics of the sample that, although it included people of both sexes and subjects from hospital and non-hospital settings, was composed mainly of people in early stages of the illness, thus limiting the generalization of the findings. Also, participants were selected using purposive sampling or convenience sampling, and were invited to participate voluntarily in the study, which explains why the number of caregivers was fewer than that of people with MS.
CONCLUSIONS
The results obtained indicate a significant impact on HRQoL of people with MS and its direct relationship with the health of primary caregivers. The participants in our sample have moderate Physical HRQoL, with the area of physical limitations caused by the disease being the most affected. Regarding Mental HRQoL, the greater effect on the subscale relating to Cognitive Function is highlighted. Age, employment status, educational level and marital status are determining factors in the HRQoL of people with MS.
Regarding the relationship between the HRQoL of the person with MS and the health of caregivers, the results of the study confirm the relationship between the physical limitations of the person with MS and an increased number of illnesses in the caregivers, and of the relationship between limitations due to emotional problems and problems in the sexual function, and a worse self-perception of health in the caregiver.
REFERENCIAS
1. Stenager E.N., Stenager E., Koch-Henricksen N., Bronnum-Hansen H., Hyllested K., Jensen K., Bille-Brahe U. (1992). Suicide and multiple sclerosis: an epidemiological investigation. Journal of Neurology, Neurosurgery & Psychiatry, 55(7), 542-545. http://dx.doi.org/10.1136/jnnp.55.7.542 [ Links ]
2. Mitchell A.J., Benito-León J., González J.M., Rivera-Navarro J. (2005). Quality of life and its assessment in multiple sclerosis: integrating physical and psychological components of wellbeing. The Lancet Neurology, 4(9), 556-566. http://dx.doi.org/10.1016/s1474-4422(05)70166-6 [ Links ]
3. Schwartzman L. (2003). Calidad de vida relacionada con la salud: Aspectos conceptuales. Ciencia y Enfermería, 9(2), 9-21.http://dx.doi.org/10.4067/s0717-95532003000200002 [ Links ]
4. Testa M., Simonson D.C. (1996). Assessment of Quality-of-Life Outcomes. New England Journal of Medicine, 334(13), 835-840. http://dx.doi.org/10.1056/nejm199603283341306 [ Links ]
5. Hernández M.A. (2000). Tratamiento de la esclerosis múltiple y calidad de vida. Revista de Neurología, 30(12), 1242-1245. https://www.neurologia.com/articulo/99517 [ Links ]
6. Rivera-Navarro J., Morales-González J.M., Benito-León J., Mitchell A.J. (2008). Dimensión social y familiar: experiencias de cuidadores y personas con esclerosis múltiple. El estudio GEDMA. Revista de Neurología, 47(6), 281-285. https://www.neurologia.com/articulo/2008071 [ Links ]
7. Olascoaga J. (2010). Calidad de vida y esclerosis múltiple. Revista de Neurología, 51(5), 279-288. https://www.neurologia.com/articulo/2010277 [ Links ]
8. Aymerich M., Guillamón I., Jovell A. J. (2009). Health-related quality of life assessment in people with multiple sclerosis and their family caregivers. A multicenter study in Catalonia (Southern Europe). Patient Prefer Adherence, 3, 311-321.http://dx.doi.org/10.2147/ppa.s6217 [ Links ]
9. McKeown L.P., Porter-Armstrong A.P., Baxter G.D. (2003). The needs and experiences of caregivers of individuals with multiple sclerosis: a systematic review. Clinical Rehabilitation, 17(3), 234-248. http://dx.doi.org/10.1191/0269215503cr618oa [ Links ]
10. Carreón-Guarnizo E., Andreu-Reinon E., Cerdán-Sánchez M., Carrasco-Torres R., Hernández-Clares R., Prieto-Valiente L., Meca-Lallana J.E. (2016). Prevalencia de la Esclerosis Múltiple en la Región de Murcia [Prevalence of multiple sclerosis in the Region of Murcia]. Revista de Neurología, 62(9), 396-402. [ Links ]
11. Vickrey B.G., Hays R.D., Harooni R., Myers L.W., Ellison G.W. (1995). A health-related quality of life measure for multiple sclerosis. Quality of Life Research, 4, 187-206. http://dx.doi.org/10.1007/bf02260859 [ Links ]
12. Aymerich M., Guillamón I., Perkal H., Nos C., Porcel J., Berra S., Montalbán X. (2006). Adaptación al español del cuestionario específico MSQOL-54 para pacientes con esclerosis múltiple. Neurología, 21(4), 181-187. [ Links ]
13. Goldberg D., Williams P. (1988). A user's guide to the General Health Questionnaire. Windsor, UK: NFER-Nelson. [ Links ]
14. Sánchez-López, M.P., Dresch V. (2008). The 12-item General Health Questionnaires (GHQ-12): reliability, external validity and factor structure in the Spanish population. Psicothema, 20(4), 839-843. [ Links ]
15. Instituto Nacional de Estadística INE. (2013). Encuesta Nacional de Salud 2011-2012. Ministerio de Sanidad, Servicios Sociales e Igualdad. Gobierno de España. [ Links ]
16. Sánchez-López M.P., Limiñana-Gras R.M. (2017). Health from a Gender Perspective. In M.P. Sánchez-López & R.M. Limiñana-Gras (Eds.), The Psychology of Gender and Health: Conceptual and Applied Global Concerns (pp.1-52). Elseiver/Academic Press. http://dx.doi.org/10.1016/b978-0-12-803864-2.00001-8 [ Links ]
17. Delgado-Mendili´var J.M., Cadenas-Di´az J.C., Ferna´ndez-Torrico J.M., Navarro-Mascarell G., Izquierdo G. (2005). Estudio de la calidad de vida en la Esclerosis Mu´ltiple. Revista de Neurología, 41(5), 257-262. [ Links ]
18. Grasso M.G., Clemenzi A., Tonini A., Pace L., Casillo P., Cuccaro A., Troisi E. (2008). Pain in multiple sclerosis: a clinical and instrumental approach. Multiple Sclerosis, 14(4), 506-513. http://dx.doi.org/10.1177/1352458507085553 [ Links ]
19. Amato M.P., Ponziani G., Siracusa G., Sorbi S. (2001). Cognitive dysfunction in early-onset multiple sclerosis: a reappraisal after 10 years. Archives of Neurology, 58(10), 1602-1606. http://dx.doi.org/10.1001/archneur.58.10.1602 [ Links ]
20. Alarcón G. S., McGwin G., Uribe A., Friedman A. W., Roseman J. M., Fessler B. J. (2004). Systemic lupus erythematosus in a multiethnic lupus cohort (LUMINA). XVII. Predictors of self-reported health-related quality of life early in the disease course. Arthritis Care & Research, 51(3), 465-474. http://dx.doi.org/10.1002/art.20409 [ Links ]
21. Hopman W. M., Coo H., Edgar C. M., McBride E. V., Day A. G., Brunet D. G. (2007). Factors Associated with Health-Related Quality of Life in Multiple Sclerosis. The Canadian Journal of Neurological Sciences, 34(02), 160-166. http://dx.doi.org/10.1017/s0317167100005989 [ Links ]
22. Cuéllar-Flores I., Sánchez-López M. P. (2012). Adaptación psicológica en personas cuidadoras de familiares dependientes. Clínica y Salud, 23(2), 141-152. http://dx.doi.org/10.5093/cl2012a9 [ Links ]
23. De Andrés-Jiménez Elena , Limiñana-Gras Rosa María (2014). El afrontamiento del cuidado en familiares cuidadores de personas con demencia: dimensiones cognitivas y el manejo de la ira. Revista Iberoamericana de Diagnóstico y Evaluación - e Avaliação Psicológica [Internet]. 2014;1(37),169-185. [ Links ]
24. Manso-Martínez M. E., Sánchez-López M. P., Cuéllar-Flores I. (2013). Salud y sobrecarga percibida en personas cuidadoras familiares de una zona rural. Clínica y Salud, 24(1), 37-45. http://dx.doi.org/10.5093/cl2013a5 [ Links ]
25. Figved N., Myhr K.M., Larsen J.P., Aarsland D. (2007) Caregiver burden in multiple sclerosis: the impact of neuropsychiatric symptoms. Journal of Neurology, Neurosurgery and Psychiatry, 78(10), 1097-1102. http://dx.doi.org/10.1136/jnnp.2006.104216 [ Links ]
26. Patti F., Pozzilli C., Montanari E., Pappalardo A., Piazza L., Levi A., Pesci I. (2007). Effects of education level and employment status on HRQoL in early relapsing-remitting multiple sclerosis. Multiple Sclerosis, 13(6), 783-791. http://dx.doi.org/10.1177/1352458506073511 [ Links ]
27. Cuéllar-Flores I., Sánchez-López M. P., Limiñana-Gras R. M., Colodro-Conde L. (2014). The GHQ-12 for the Assessment of Psychological Distress of Family Caregivers. Behavioral Medicine, 40(2), 65-70. http://dx.doi.org/10.1080/08964289.2013.847815 [ Links ]
28. Pinquart M., Sörensen S. (2006). Gender differences in caregiver stressors, social resources, and heath: an update meta-analysis. Journal of Gerontology, Series B: Psychological Sciences, 61(1), 33-45. http://dx.doi.org/10.1093/geronb/61.1.p33 [ Links ]
29. Yee J., Schulz R. (2000). Gender differences in psychiatric morbidity among family caregivers: a review and analysis. The Gerontologist, 40(2), 147-164. http://dx.doi.org/10.1093/geront/40.2.147 [ Links ]
30. Acaster S., Perard R., Chauhan D., Lloyd A.J. (2013). A forgotten aspect of the NICE reference case: an observational study of the health related quality of life impact on caregivers of people with multiple sclerosis. BMC Health Services Research, 13(1), 346. http://dx.doi.org/10.1186/1472-6963-13-346 [ Links ]
31. Forbes A., While A., Mathes L. (2007). Informal carer activities, carer burden and health status in multiple sclerosis. Clinical Rehabilitation, 21(6), 563-575. http://dx.doi.org/10.1177/0269215507075035 [ Links ]
Received: March 23, 2021; Accepted: July 10, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
