










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.22 n.70 Murcia Apr. 2023 Epub June 26, 2023
https://dx.doi.org/10.6018/eglobal.547181
Originals
Validation of a knowledge and attitude instrument for nurses for the prevention of the diabetic foot
1Master's student in Nursing. Faculty of Nursing. Benemérita Universidad Autónoma de Puebla. México
2PhD in Nursing Sciences. Faculty of Nursing. Benemérita Universidad Autónoma de Puebla. México
3DPhD in Chemical Sciences in the area of Biochemistry and Molecular Biology. Benemérita Universidad Autónoma de Puebla. México
Introduction:
The prevalence of type 2 diabetes has increased drastically, and people who suffer from this metabolic and chronic disease present alterations such as neuropathy and reduced blood flow, which increase the risk of diabetic foot, and thus its prevention is important. The objective was to perform the validation of a knowledge and attitude instrument for nurses for the prevention of the diabetic foot.
Materials and methods:
A descriptive, cross-sectional study with convenience sampling was carried out using a population of 148 nursing professionals working in a first-level care facility in the State of Puebla.
Results:
A valid and reliable instrument was obtained, with a Cronbach's Alpha coefficient of .84 for the knowledge subscale and of .62 for the attitude subscale, and a value of p<.000 in the Bartlett sphericity test and the Kaiser-Meyer-Olkin test. The values of the Kiaser-Meyer-Olkin test were .863 for the knowledge subscale and .563 for the attitude subscale.
Discussion:
We contribute with an instrument adapted and valid for the Mexican context, which allows measuring the knowledge and attitude variables for the prevention of the diabetic foot.
Conclusion:
The empirical indicator adapted to the Spanish language, which measures the study variables in nursing professionals, emphasizes the importance of knowledge translation and application of evidence-based practice in diabetic foot prevention.
Keywords: Validation; Knowledge; Attitude; Diabetic foot
INTRODUCTION
According to the World Health Organization (1, there are 422 million people with type 2 diabetes (T2D) worldwide. This is a chronic degenerative disease characterized by high blood glucose levels, which over time leads to serious damage. The Organization for Economic Co-operation and Development mentions that Mexico has the highest numbers of T2D in adults (13.1%), with complications of blindness, kidney failure, stroke, and amputation, and 1.5 million deaths have also been reported as a consequence of this health problem (2.
The International Working Group on the Diabetic Foot3 has established that people with T2D that present diabetic neuropathy and reduced blood flow have an increased risk of developing ulcers and infections that cause the destruction of soft tissue in the lower limbs, which is the main cause of the diabetic foot (DF). The diabetic foot has a large impact on the morbidity and mortality of patients with T2D. According to Leciñena et al.4, one in every five patients will develop DF in their lifetime and an amputation occurs every 30 seconds, which results in a problem requiring long therapeutic periods, since half the cases will have a healing interval of more than six months, making it the most costly complication in the Health System.
Eighty percent of DF, foot ulcer, and amputation cases could be prevented by activities focused on the anticipation of complications through health education and periodic clinical examinations, whose times are established according to the presence of risk factors. However, the lack of self-care in patients with T2D is an underlying problem limited by prevention and timely action by health care professionals (5.
In this sense, nurse professionals play a leading role in care actions for people with T2D by identifying risk factors and preventing complications. In the case of DF, these actions include the identification of changes in the skin and distal sensation and perception, foot care, and the application and use of emerging technologies, as well as the development of knowledge, attitudes, and abilities to identify in a timely manner conditions that may cause complications, which requires the use of valid and reliable empirical indicators (6,7.
A literature review allowed to identify two instruments that measure knowledge for the prevention of the diabetic foot. The first one, proposed by Abdullah et. al.,8 measures the knowledge and practice level for the prevention of diabetic foot complications. The questionnaire consists of a structured interview and a checklist of observations, which were developed based on literature related to the prevention of diabetic foot complications in patients with diabetes. In addition, these authors used the KAP model, which was employed in the 1950s in family planning and population studies, and is an illustrative model applied to a specific population to determine the knowledge (K), attitudes (A), and practices (P) of the population regarding a particular subject9,10. The second instrument was proposed by Kaya and Karaka11 and measures the knowledge level of nurses on diabetic foot management. This instrument consists of 68 questions with a dichotomous scale (true/false) divided into four sections: “Risk factors”, “Foot examination”, “Foot complications”, and “Footwear selection”.
The instruments mentioned above have been used in countries such as Saudi Arabia, Ethiopia, Malaysia, Pakistan, and Sri Lanka. However, no scales have been identified for the measurement of these variables in Mexico, and thus it is necessary to have a valid and reliable empirical indicator that allows the measurement of knowledge and attitude in nursing staff for the prevention of the diabetic foot in the Mexican context. The measurement of these variables is of great importance because it will allow to identify care strategies and develop intervention programs focused on the care of people with T2D. Thus, the objective of the present study was to adapt and validate a knowledge and attitude instrument for nurses for the prevention of the diabetic foot (8.
MATERIALS AND METHODS
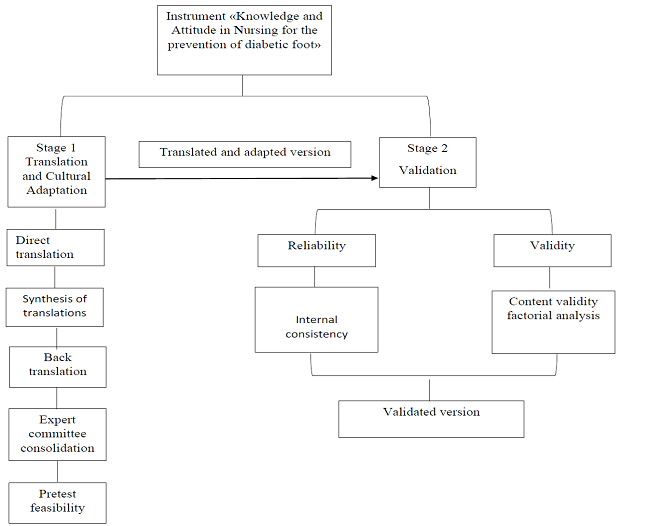
Following Ramada-Rodilla, Serra-Pujadas, and Delcós-Clanchet12, a process of translation, cultural adaptation, and validation (TCAV) was conducted from January to August 2022. This process is fundamental when intending to use measuring instruments developed in other countries. The process consisted of two stages, where the first stage was Translation and cultural adaptation, which included five steps. The first step was the translation from English to Spanish by two translators (A-B). Translator A had experience in technical translation, English was their second language, and was familiar with the objectives and concepts concerning the instrument. Translator B was a native English speaker and was not familiar with the concepts and objectives of the instrument. The second step consisted in creating the first Spanish version of the instrument using the translated versions (translation summary). In the third step, a back-translation was made by two translators that were not familiar with the concepts of the instrument, which resulted in an integrated first version of the instrument.
In the fourth step, an evaluation form for content validity was sent digitally to seven experts in the care of people with wounds. Content validity was evaluated using a Likert-type response scale with a five-point score (0= Definitely not related, 1 = Not related, 2 = Not sure of the relationship, the item requires further review, 3 = Related, but minor modifications are required, and 4 = Extremely related, no changes). The scoring and comments by each expert were compared and analyzed, which resulted in a second version of the instrument.
In the fifth step, a pilot test was performed with 34 nurse professionals working in first-level care facilities in the state of Puebla. As a follow-up to the results, a final test was conducted using a descriptive, cross-sectional design with convenience sampling on a total sample of 148 nurse professionals from a Health Center with Expanded Services of the State of Puebla. The data were collected virtually using Google Forms, where the authorization of the participants was obtained through informed consent and voluntary and confidential participation.
The second stage of the process consisted of the validation of the instrument using SPSS version 24, where the internal validity and rotated component matrix were calculated, as well as the values of the Bartlett sphericity and Kaiser-Meyer-Olkin (KMO) tests and Cronbach’s alpha coefficient.
The research project was approved by the Research and Graduate Studies Committee of the Nursing Faculty-BUAP, with registration number SIEP/051/2022, and the study complied with the Regulations of the General Health Law on Research (13.
RESULTS
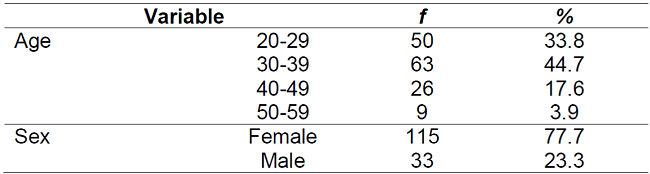
The sample consisted of 148 nurses working in a Health Center with Expanded Services of the state of Puebla. The mean age was 34.47 years, 77% were female, and the mean working experience was M=6.86 years (SD:5.3); (Table 1).
With respect to the content validity of the instrument, once the first Spanish version of the questionnaire was obtained, the instrument Knowledge and Attitude for the prevention of the diabetic foot, containing a total of 27 questions, was sent for review by expert judges in the area of care of people with wounds. The judges answered an instrument with a Likert-type scale that allowed to identify the consistency of each item. The evaluation also included the content validity ratio proposed by Lawshe14, which allows to obtain a score for each question, and the index proposed by Davis14, which should be higher than .80 for the items to be adequate within the instrument. The result of this index in the present study was .84, which is an acceptable score for internal validity.
Once the content validity was obtained, the following modifications proposed by the experts were made: item number 2 was added to the knowledge questionnaire (neuropathy is assessed with the tuning fork, Semmes-Weinstein monofilament, and hammer) and item 8 was added to the attitude subscale (it is not my responsibility to educate patients with diabetic ulcers). The second version of the instrument was then integrated, and a pilot test was conducted with 34 nurses. Based on those results, the response options (Likert-type) were adjusted in the subscale of knowledge for the prevention of the diabetic foot, resulting in the options “do not agree at all”, “moderately agree”, and “strongly agree”.
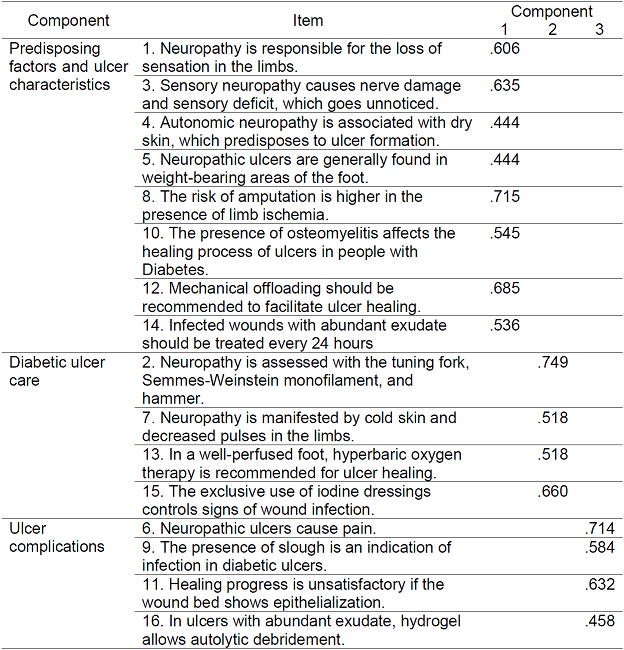
Kumarasinghe et.al.15 describe four components in the subscale of Knowledge for the prevention of the diabetic foot, but in the present study three components were identified according to the factor analysis: predisposing factors and ulcer characteristics (1,3,4,5,8,10,12, and 14), ulcer complications (6,9, and 11), and diabetic ulcer care (2,7,13, and 15) (Table 2).
Table 2. Rotated component matrix, Subscale of Knowledge for the prevention of the diabetic foot.
Source: Created by the authors
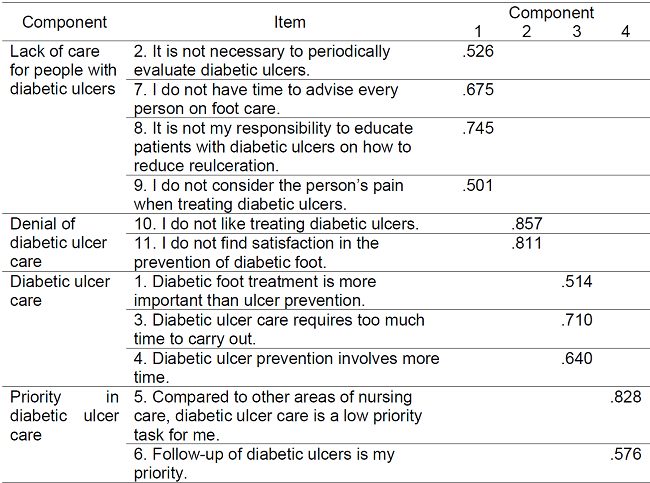
In the subscale of attitude for the prevention of the diabetic foot, four components were obtained, which contrasts with the main authors that did not perform this analysis in this subscale Kumarasinghe et.al.15, and thus the following components are proposed in the present study: Lack of care for people with diabetic ulcers (2,7,8,9), denial of diabetic ulcer care (10,11), diabetic ulcer care (1,3,4), and priority in diabetic ulcer care (5,6); (Table 3).
Table 3. Rotated Component Matrix, Subscale of Attitude for the prevention of the diabetic foot.
Source: Created by the authors
An instrument consisting of 27 questions was obtained, where 16 items correspond to the Knowledge subscale and 11 to the Attitude subscale. The values obtained for Bartlett’s sphericity test14) and the Kaiser-Meyer-Olkin (KMO) adequacy test16) were significant in both subscales (Table 4).
Table 4. Bartlett’s sphericity test and Kaiser-Meyer-Olkin (KMO) test.

Source: Created by the authors
The reliability of the instrument was subsequently determined using Cronbach’s Alpha Coefficient, which indicates the degree of correlation between the variables and the internal consistency of the scale. The Cronbach’s Alpha values obtained for the subscales of Knowledge and Attitude for the prevention of the diabetic foot were .84 and .62, respectively (17, which is considered an acceptable internal consistency.
DISCUSSION
The objective of the present study was to carry out the cultural adaptation and validation of the instrument Knowledge and Attitude for the prevention of the diabetic foot (8, since type 2 diabetes has a significant impact on the quality of life of the people who suffer from this disease. Furthermore, complications such as the diabetic foot also have important effects on the quality of life of people, as well as an impact on the care provided by the health service system. Therefore, the prevention of DF is one of the most important challenges for nurse professionals, and the lack of a tool for measuring these variables in the Mexican context emphasizes the importance of carrying out a cultural adaptation using the methodology proposed by Ramada-Rodilla et al.12). The evaluation by an expert committee allowed a more comprehensive analysis and understanding of the items, as noted by Kaya and Karaka11, since the experts provide suggestions to improve, change, or adapt the items of the instrument. Seven experts in the care of people with wounds participated in the present study, which is similar to the study by Abdullah et. al.8, where five experts were considered, two of which were part of the academic staff from the medical surgical and community health nursing fields and three were staff from the statistical department. In the study by Kaya and Karaka11, the opinion of five experts in nursing fundamentals and surgical nursing was obtained to evaluate the items in terms of statement and content validity.
There was a similarity with the original proposal of the instrument in the results of the components of the subscale of knowledge for the prevention of the diabetic foot. In the original proposal, the components predisposing factors and ulcer characteristics are combined into one component, but the other components remained the same in the present study (ulcer complications and diabetic ulcer care) (15. In the case of the subscale of attitude for the prevention of the diabetic foot, unlike Kumarasinghe et.al.,15 the present study contributes with the determination of four components. In addition, regarding the reliability of the original instrument (11, there were differences with the present study, since a higher Cronbach’s Alpha value was obtained, which allows higher precision in the application of the instrument in the Mexican context.
CONCLUSIONS
The cultural adaptation and validation of the instrument Knowledge and Attitude for the prevention of the diabetic foot is aimed at nursing staff in the Mexican context, since they are an essential part in promotion and prevention in the health of people with T2D. Having a valid and reliable instrument is a necessary and useful tool because it allows to improve the interventions in the care of a person, as well as to establish strategies for the continuous improvement of the knowledge and attitude of professionals in the prevention of DF, all of which allows to promote evidence-based practices for the timely detection of DF.
REFERENCIAS
1. Organización Mundial de la Salud (OMS). Informe Mundial sobre la Diabetes (2022). Recuperado de: https://www.who.int/health-topics/diabetes#tab=tab_1 [ Links ]
2. Organización para la Cooperación y el Desarrollo Económico (OCDE). Diabetes en México (2019). Recuperado de: https://www.oecd.org/mexico/health-at-a-glance-mexico-ES.pdf (oecd.org) [ Links ]
3. International Working Group on the Diabetic Foot (IWGDF). Guidance on the prevention of foot ulcers in at-risk patients with diabetes (2015). Recuperado de: IWGDF guidance on the prevention of foot ulcers in at-risk patients with diabetes - Bus - 2016 - Diabetes/Metabolism Research and Reviews - Wiley Online Library [ Links ]
4. Leciñena Cucalón Gloria, Embid Gran Silvia, Pelegrín Monje Eva, Portero Garín Nuria, Lucas García Patricia, Auría Egea María. Abordaje de las complicaciones neuropáticas del paciente diabético. A propósito de un caso. (2021) Revista Sanitaria de Investigación, 2(7), 41. Recuperado de: Abordaje de las complicaciones neuropáticas del paciente diabético. A propósito de un caso. (https://revistasanitariadeinvestigacion.com/) [ Links ]
5. Wam Serrano Isela, País Lescano Aura Cecilia, Espinoza Deza Julia Gladys, Arce Barreto Amparo Socorro del Pilar. Factores de Riesgo en la Incidencia de Pie Diabético (2021). Revista científica CURAE, 4(1), 38-47. Recuperado de: FACTORES DE RIESGO EN LA INCIDENCIA DE PIE DIABETICO: REVISTA CURAE | Revista científica CURAE (uss.edu.pe) [ Links ]
6. Abate Teshager Woldegiorgis Enyew Alamirew , Gebrie Feleke, Bayuh Haregnesh. Nurses' knowledge and attitude towards diabetes foot care in Bahir Dar, North West Ethiopia. (2020). Heliyon, 6(11). Recuperado de: Nurses' knowledge and attitude towards diabetes foot care in Bahir Dar, North West Ethiopia - PubMed (nih.gov) [ Links ]
7. Ballen Elizabeth Catalina Rincón. Narrativa de enfermería: cuidado holístico de un paciente con pie diabético (2021). Revista Repertorio de Medicina y Cirugía, 2021, vol. 30, no 3. Recuperado de: Narrativa de enfermería: cuidado holístico de un paciente con pie diabético - DOAJ [ Links ]
8. Abdullah Wafaa H. Samira Al Senany, Hanaa Khaled Al-Otheimin. Capacity building for Nurses' knowledge and practice regarding prevention of diabetic foot complications (2017). International Journal of Nursing Science, 7(1), 1-15. Recuperado de: Nurses knowledge & Practice, Primary health care center, Diabetic foot complications (researchgate.net) [ Links ]
9. Launiala, B. How much can a KAP survey tell us about people's knowledge, attitudes and practices? Some observations from medical anthropology on malaria in pregnancy in Malawi Background: KAP surveys (2009). Anthropology Matters Journal, 11(1), 1-13. Retrieved from http://www.anthropologymatters.com. [ Links ]
10. Goutille, F. Knowledge, Attitudes and Practices for Risk Education: how to implement KAP surveys (2009). Pôle Publications Professionnelles, Catherine Clavel, Catherine Dixon. Retrieved from: doi: 978-2-909064-21-5. [ Links ]
11. Kaya Zahide, Karaca Anita. Evaluation of nurses' knowledge levels of diabetic foot care management. Nursing research and practice, (2018). Recuperado de: Evaluation of Nurses' Knowledge Levels of Diabetic Foot Care Management - PubMed (nih.gov) [ Links ]
12. Ramada-Rodilla José María, Serra-Pujadas Consol, Delclós-Clanchet George L. Adaptación cultural y validación de cuestionarios de salud: revisión y recomendaciones metodológicas. Salud Publica Mex (2013); 55:57-66. Recuperado de: Adaptación cultural y validación de cuestionarios de salud: revisión y recomendaciones metodológicas (scielo.org.mx) [ Links ]
13. Secretaría de Servicios Parlamentarios. Reglamento de la Ley General de Salud en Materia de Investigación para la Salud. Diario Oficial de la Federación, (2014). DOF 12-07-2018. Recuperado de: Ley General de Salud (www.gob.mx) [ Links ]
14. Suárez-Álvarez Pedrosa Ignacio, García-Cueto Eduardo Javier. Evidencias sobre la validez de contenido: avances teóricos y métodos para su estimación. Acc. Psic. 2013; 15 (2): 3-18. Disponible en http://www.redalyc.org/articulo.oa?id=344033718006 [ Links ]
15. Kumarasinghe S. A., Hettiarachchi P., Wasalathanthri S. (2018). Nurses' knowledge on diabetic foot ulcer disease and their attitudes towards patients affected: A cross-sectional institution-based study (2018). Journal of clinical nursing, 27(1-2), e203-e212. [ Links ]
16. Gutiérrez López, Luz Elena. Protocolo para realizar análisis factorial en variables que afectan las condiciones laborales. Rev Ingeniare, 2019; 15 (26): 13-33. DOI: https://doi.org/10.18041/19092458/ingeniare.26.6564. [ Links ]
17. López-Aguado Mercedes, Gutiérrez-Provecho Lourdes. Cómo realizar e interpretar un análisis factorial exploratorio utilizando SPSS. Rev Inov Educ, 2019; 12(2): 1-14. Disponible en http://doi.org/10.1344/reire2019.12.227057 [ Links ]
Received: November 13, 2022; Accepted: February 03, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
