










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.23 n.73 Murcia Jan. 2024 Epub Feb 23, 2024
https://dx.doi.org/10.6018/eglobal.568371
Originals
Audiovisual Effectiveness of Independent Fetal Well-being Monitoring on Mother-Fetus Attachment and Birth Outcomes
1Nursing Studies Program, Faculty of Health Sciences, Universitas Aisyiyah, Yogyakarta, Indonesia
Introduction:
The mother-fetus bond plays an important role in pregnancy care, impacting birth outcomes. Monitoring fetal movement is a fundamental competence for pregnant women to do independently. Objective: to produce audiovisual monitoring of independent fetal movement and prove its effectiveness on maternal-fetal attachment and birth outcomes.
Methods:
Phase I, developing Audiovisual Fetal Well-being Monitoring, with literature study steps, developing scenarios, creating audiovisuals, testing the validity of experts. Stage 2 tested the effectiveness of audiovisual media on maternal-fetal attachment with the Prenatal Attachment Inventory instrument and birth outcomes from infant birth weight. Design of true experimental pretest-posttest control group approach. Samples of pregnant women with a history of antenatal care at the Kasihan II Health Center, Bantul, Yogyakarta, Indonesia with the following criteria: single pregnancy, normal, gestational age 28-36 weeks. Respondents of 60 subjects were divided into experimental and control groups. Normal data were tested by paired t test, independent t-test and MANOVA.
Results:
Content expert validity test score 81% very valid, media expert validity score 80.33%, valid. The audiovisual application showed the results of the paired t-test, both in the experimental and control groups there were differences in pretest and posttest, P <0.05. Independent sample t-test P < 0.05 and simultaneous MANOVA results showed maternal-fetal attachment score and birth outcome P < 0.05.
Conclusion:
Independent monitoring of fetal well-being using audiovisual media simultaneously affects the increase in maternal-fetal attachment scores and birth outcomes so it is recommended that second trimester pregnant women be taught techniques for counting fetal movements and practicing them routinely.
Keywords: Fetal Well-being; Maternal-Fetal Attachment; Birth outcomes
INTRODUCTION
Perinatal mortality is a world health problem, indicated by the infant mortality rate of 27.4/1000 live births and the highest is due to premature birth and low birth weight(1). Maternal health problems have become a target in the third target of the Sustainable Development Goals (SDGs), namely good health and well-being. The SDGs targets include reducing the infant mortality rate to less than 20 per 1000 live births(2). In Indonesia the infant mortality rate is 19.5 per 1000 live births, with the 2020-2024 National Medium Term Development Plan target of 16/1000 live births(3),(4). Efforts to achieve targets by the government include antenatal care services at least 4 visits, childbirth and postpartum, improving the referral system and mother class programs(5). Until now these efforts have not been able to achieve the expected target, so a strategy is needed to improve services since pregnancy.
Pregnancy adaptation is the basis for the mother to build a relationship with the fetus during pregnancy(6). The bond between mother and fetus plays an important role in the health of the mother and fetus and influences the mother's decision to behave healthily during pregnancy. The mother-fetus love relationship contributes to the protection provided by the mother to the fetus, reflected in the behavior of attention, love, affection, petting behavior, communication, responding to fetal movements, carrying out routine antenatal care and attending classes for pregnant women(7,8,9). The strong attachment between mother and fetus affects health practices during pregnancy which has an impact on the welfare of the fetus. Poor mother-fetal bonding affects fetal mood, fetal growth and worsens pregnancy outcomes, babies can be born prematurely or with low birth weight, fetal distress and fetal death(10). Study of 158 pregnant women in Denmark, there were 35 (22.1%) with low attachment, 18 of them resulted in premature birth and low birth weight(11). Studies in pregnant women in Africa show that strong maternal-fetal attachment is associated with good health practices and reduced adverse neonatal outcomes (prematurity and low birth weight), with an odds ratio: 0.91(12). The stronger the bond, the more the mother maintains the health of herself and her fetus and produces normal baby births(13).
Fetal well-being can be assessed from fetal movements. Poor attachment problems are triggered by maternal psychological problems that affect the sympathetic system, responding to the maturation and evolution of the fetal autonomic nervous system, fetal heart rate and decreased fetal movement(14),(15). Fetal movement can be measured independently by pregnant women as an indicator of fetal well-being and at the same time to arouse the behavior of mother's affection, care and concern for the fetus. Monitoring fetal movement is a competency that pregnant women must know and can practice in order to monitor the health of the fetus. Monitoring of fetal movement is an important thing to know and carry out by pregnant women independently to find out the condition of the fetus, determine the steps for treatment or the need for a health facility quickly when problems with fetal movement are found so as to prevent worsening of fetal growth and development and infant death. If this can be done properly it is hoped that the infant mortality rate can decrease(16). Independent fetal movement monitoring training is essential to increase the understanding and practice of monitoring fetal movement properly so that treatment can be immediately received if dangerous signs of pregnancy are found that start from a decrease in fetal movement, thus contributing to reducing maternal and infant morbidity and mortality(17).
The formulation of the problem found that there is no research on training in monitoring fetal movements in pregnant women. Likewise, in the government's standard education program for pregnant women, there is no specific training on techniques for monitoring fetal movements and interpreting the results, so it is important to conduct research to develop training in calculating fetal movements. Monitoring of fetal movement can be developed in a more innovative way, namely using audiovisual media, with material, time duration, and the use of appropriate language. Audio-visual aids media has been proven from previous research that audio-visual media is faster for participants to understand material. The material is delivered digitally using spoken words in the form of illustrations, photos, animations or videos(18). Audio-visual aids media is preferred because it is equipped with pictures or photos that look real, making it easier for respondents to understand(19). Until now there has not been found the results of previous studies that developed audiovisual media techniques for monitoring fetal movement independently. The aim of the study was to produce audiovisual media for independent fetal movement monitoring by pregnant women and to prove its effectiveness on maternal-fetal attachment levels and birth outcomes.
METHODS
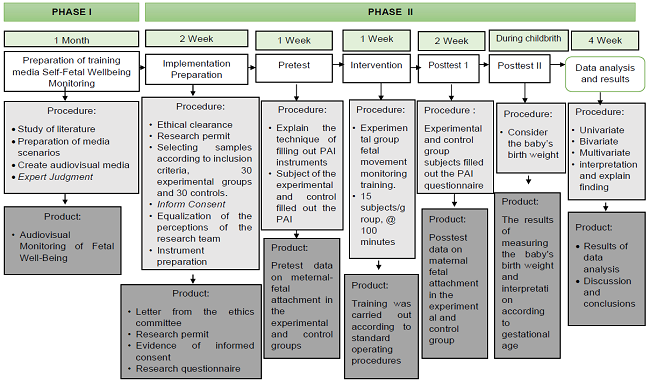
The research was conducted in two phases including developing audiovisual media for monitoring independent fetal movements by pregnant women and testing the effectiveness of its application on maternal-fetal bonding and birth outcomes (Picture 1). The first phase of research on the preparation of audiovisual media was carried out November 1 2022-January 15, 2023 and the second phase of research was carried out January 23 - April 2, 2023.
Stage 1. Audiovisual Fetal Welfare Monitoring
Activities carried out in stages include: literature study on the material of monitoring fetal well-being independently; prepare a scenario design for the development of audiovisual media; collaborate with information technology and health promotion experts in making audiovisuals. The audiovisual results were tested for validity by material experts and media experts. Testing with a score of 1-5 on each aspect that is evaluated. Score 1: not very suitable, 2: not suitable, 3: quite suitable, 4: suitable and 5: very suitable. The expert validity test consists of 4 aspects, with a score of 4-20 and the media validity test consists of 6 aspects, with a total score of 6-30. Validity categories include: 0-20%=very invalid; 21-40%=invalid; 41-60%=quite valid; 61-80%=valid and 81-100%=very valid. Revisions were made based on input and suggestions by experts.
Stage 2. Testing the effectiveness of audiovisual media monitoring fetal well-being on mother-fetal bonding and birth outcomes
Research with a true experimental design with a pretest-posttest control group design approach. The population is all pregnant women in the Working Area of the Kasihan Bantul Health Center, Yogyakarta. The sample was all pregnant women who checked their pregnancies at the Kasihan II Health Center, Bantul, Yogyakarta, Indonesia with the following criteria: single and normal pregnancies, gestational age 28-34 weeks. The sample size was calculated by estimating the sample size of 2 paired groups, Lemeshow. The method used simple random sampling, resulting in 60 samples which were divided into the experimental group and the control group. In the intervention group, a pretest was carried out before being given training in counting fetal movements with audiovisual media. Respondents were asked to carry out at home 2 times a week and document it on the observation sheet. At 3 weeks after training, posttest maternal-fetal attachment. Data processing with editing, coding, data entry and data cleaning. Univariate analysis of mean, minimum and maximum values, and 95% confidence interval on the dependent variable, namely maternal-fetal attachment levels and birth outcomes, as well as sociodemographic characteristics including: gestational age, gestational age, gravid status and employment status. Bivariate analysis, an equivalence analysis test was carried out with data normality in the intervention group and the control group. For normal data results, a paired t-test and an independent t-test were performed, then a multivariate test was performed, using the multivariate analysis of variance (MANOVA) test. and 95% confidence interval on the dependent variable, namely the level of maternal-fetal attachment and birth outcomes, as well as sociodemographic characteristics including: maternal age, gestational age, gravida status and employment status. Bivariate analysis, an equivalence analysis test was carried out with data normality in the intervention group and the control group. For normal data results, a paired t-test and an independent t-test were performed, then a multivariate test was performed, using the multivariate analysis of variance (MANOVA) test. and 95% confidence interval on the dependent variable, namely the level of maternal-fetal attachment and birth outcomes, as well as sociodemographic characteristics including: maternal age, gestational age, gravida status and employment status. Bivariate analysis, an equivalence analysis test was carried out with data normality in the intervention group and the control group. For normal data results, a paired t-test and an independent t-test were performed, then a multivariate test was performed, using the multivariate analysis of variance (MANOVA) test.
This study has been declared to have passed an ethical review from the Ethics Committee of the Universitas Aisyiyah Yogyakarta Indonesia, with Number 2531/KEP-UNISA/I/2023. The study has applied the basic ethical principles of respecting the dignity of others, not harming and the principle of justice. Consent to be a research respondent was given voluntarily by the research subject, indicated by signing proof of consent on the consent form. All data is kept confidential and only used for study purposes.
RESULTS
Stage I. Development of Audiovisual Fetal Welfare Monitoring
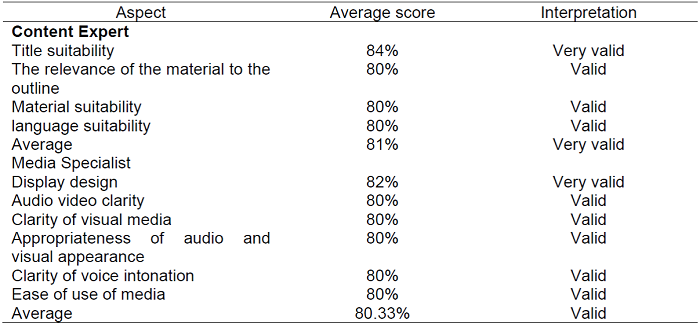
The development begins with a literature study on fetal well-being monitoring, including: definition, objectives, benefits, monitoring techniques, interpretation of results and conclusions. Followed by a storyboard that facilitates the preparation of audiovisual media. Story board equipped with pictures, moving and still animations and instrumental music that supports relaxation. The voice in the form of words to clarify the video display is carried out by a model with a soft and attractive intonation. All components are assembled into one media unit in accordance with the storyboard and flowchart. Audiovisual generated with a duration of time: 4 minutes 13 seconds. The validity test was carried out by 2 content experts in the field of maternal and child health and 2 media experts from the science of communication and graphic design. Table 1 shows the results of the validity of the content expert with a score of 81% very valid interpretation. Revisions have been made to the use of language and the sequence of materials. Media validity test results with a score of 80.33%, a valid interpretation.
Stage 2. Testing the effectiveness of audiovisual monitoring of fetal well-being on maternal-fetal bonding and birth outcomes
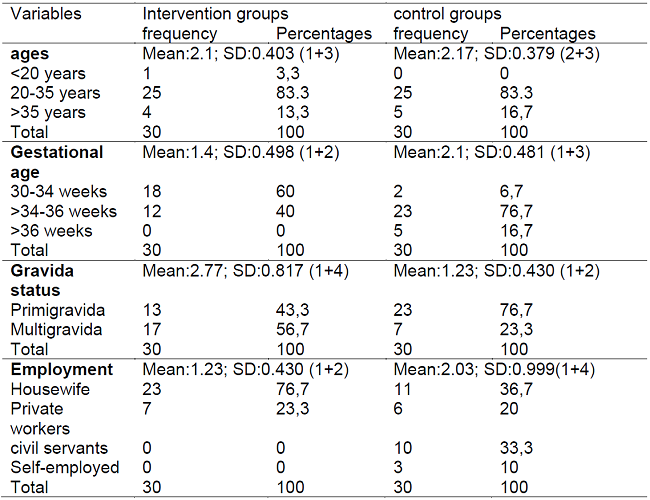
Table 2 shows the sociodemographic characteristics of the respondents. Of the 30 respondents in the intervention group and 30 respondents in the control group, most were 20-35 years old, 25 (83.3%) each. The most gestational age in the intervention group was 30-34 weeks, namely 18 (60%), the control group > 34-36 weeks, namely 23 (76.7%). The majority of the intervention group was multigravida, 17 (56.7%) and the primigravida control group was 23 (76.7%). The occupational status of the intervention and control groups was mostly as housewives, 23 (76.7%) and 11 (36.7%).
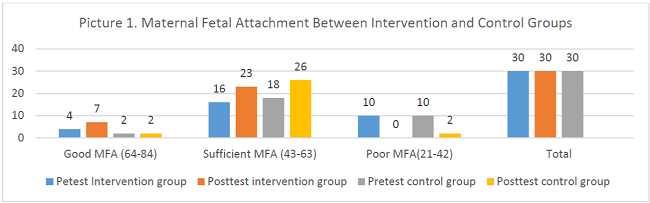
Picture 2 shows the results of the Maternal-Fetal Attachment level. Most of the intervention and control groups had moderate MFA levels. The results of the intervention group pretest 16 (53.33%) and posttest increased to 23 (76.66%), while the control group, pretest 18 (60%) and posttest increased to 26 (86.66%).
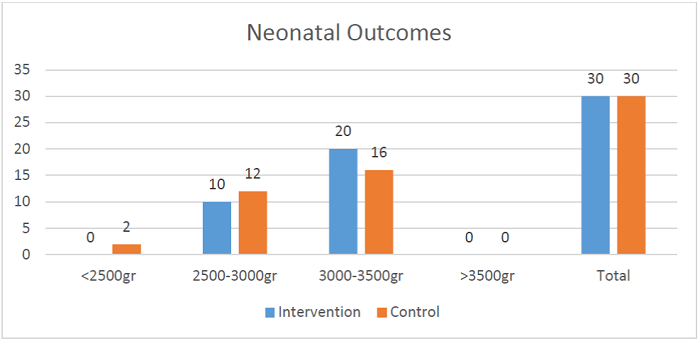
Picture 3 is the results of births, which shows the results of the majority with babies born weighing 3000-3500 grams, in the intervention group as many as 20 (66.67%) babies were born and in the control group as many as 16 (53.33%) babies were born. In the control group there were 2 (6.67%) babies born with birth weight less than 2500 grams.
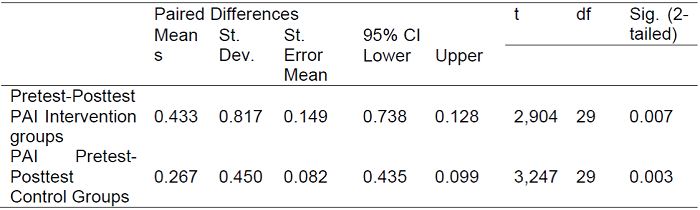
The results of the paired t-test are shown in table 3, with the results of the intervention group calculating P = 0.433 with a significance of 0.007 <0.05. Control group P count = 0.267 with a significance of 0.003 <0.05.
Table 3. Paired T-Test Prenatal Attachment Inventory Scores Pre-test and Posttest in the Intervention and Control Group (N=60).
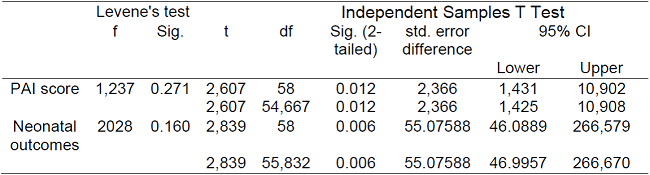
The results of the independent sample t-test in table 4 show that the score of the Prenatal Attachment Inventory (PAI) shows the difference in the level of maternal-fetal attachment between the intervention and control groups with the result t count = 2.607 with a significance of 0.012. While the neonatal results showed a t value of 0.160 with a significance of 0.006.
Table 4. Independent Samples T Test Prenatal Attachment Inventory Scores and Birth Outcomes Intervention and Control Group (N=60).
In the final stage of the manova multivariate test, which tested the independent variable providing fetal movement monitoring training to the two dependent variables including the level of maternal-fetal attachment and birth outcomes, each calculated result showed a significance level of 0.013 and 0.006 <0.05. This proves that the provision of independent fetal movement monitoring training using audiovisual simultaneously has an effect on increasing maternal-fetal attachment and normal birth outcomes.
DISCUSSION
The results of the study showed that there was an effect of providing independent fetal well-being monitoring training through audiovisuals on maternal-fetal attachment. This is evidenced by changes in maternal-fetal attachment scores from the pretest and posttest of the intervention group. there was a change in the maternal-fetal attachment score on the posttest which was better than the pretest after being given training on independent fetal well-being monitoring using audiovisual. The group that received the intervention of independent fetal well-being monitoring training using audiovisual produced a better prenatal attachment inventory score, meaning that maternal-fetal attachment was better than the control group who did not receive training.
The results of relevant studies explain that audiovisual is an interesting medium, in the form of a moving image simulation of an object. This media is suitable for pregnant women to give a real picture, provide memory retention, involve hearing and sight with sound and images so that it is easy to remember, follow and practice again(20). Another study stated that audiovisual displays objects or events that are close to their actual state (overcoming the limitations of space and time) which can clarify information with manipulation techniques, both size, color, and speed. Audiovisual is able to clarify information by means of repeated viewing, the displayed image can be stopped to be observed for a moment carefully, making it easier for pregnant women to practice the training again to apply it independently(21).
Training on fetal movement monitoring through audiovisual media can be more easily understood and re-practiced independently by respondents. The activity of counting fetal movements causes pregnant women to feel the fetus moving and triggers them to feel the protruding parts of the fetus. This activity evokes a mother's sense of affection, care and concern for the fetus. The mother-fetus love relationship contributes to the protection provided by the mother to the fetus, attention, love, affection, caring for the fetus better. A fetus that is well cared for, a good mother's psychology triggers optimal fetal growth and development, the fetus is healthy and born normally. The results of this study are corroborated by previous studies which state that pregnant women need health promotion about their pregnancy so that it encourages mother-fetus attachment and pregnancy care practices(13).
In the control group, those who were not given training in monitoring fetal well-being also showed higher posttest results than pretest. The majority of respondents in the control group were primigravida obstetrics, namely pregnant women for the first time. The first experience of pregnancy so that the lack of knowledge and understanding of the changes in pregnancy can further trigger anxiety, exacerbate the psychological condition of the mother and the action of mother-fetus attachment(22). Lack of knowledge and experience triggers primigravida mothers to seek information about changes during pregnancy and pregnancy care. Information can be obtained through electronic and non-electronic mass media. In line with this, after obtaining information about pregnancy development and care, mothers are calmer, enjoy pregnancy and pay more attention to pregnancy care, feel healthier during pregnancy(23).
Birth outcome data in the intervention group were better than the control group. These results prove that strong maternal-fetal attachment is associated with good health practices thereby reducing adverse neonatal outcomes.Good maternal-fetal attachment is psychologically beneficial in adapting to pregnancy and carrying out the role of mother. In line with studies on pregnant women in Iran, strong maternal-fetal attachment stimulates mothers to take better care of their health, willingness to care for pregnancy and awareness in avoiding things that endanger pregnancy such as smoking, alcohol and consumption of unhealthy foods.The results of maternal fetal attachment, better health care practices and resulting in an average birth weight of 3052.38 grams(13). Another study added that the quality of good maternal-fetal attachment has a significant impact on the growth and development of infants after birth until they are 3 months old with good growth and development results(9).
These results were also influenced by the sociodemographic characteristics of the respondents which included the majority of respondents in the intervention group aged 20-35 years, gestational age 30-34 weeks and the mother's occupation as a housewife. Age 20-35 years is a mature age that contributes to a better understanding of the process of pregnancy. Mothers are also able to adapt more quickly to conditions of pregnancy, the tendency to care for pregnancy will be better and can more quickly improve the bond between mother and fetus, thereby reducing the risk of premature birth and low birth weight. Mother-infant attachment response is faster in mothers with more mature age(24).The results of previous studies stated that the tendency for premature and low birth weight births was smaller for mothers who gave birth at the age of 20-35 years with an odds ratio of 1.064. Mothers with a healthy reproductive age, namely 20-35 years, the development and function of the reproductive system are more mature so that it is easy and fast to overcome the critical phase, the transitional period in pregnancy compared to those of reproductive age at risk (ages less than 20 years or more than 35 years)(25,26).
The results of this study are also supported by the sociodemographic employment status of the majority of pregnant women as housewives. Housewives have more flexible time to rest, caress the fetus, talk to the fetus in a relaxed situation. Mothers become more regular in their pregnancy care, can manage time more freely to practice counting fetal movements when they are relaxed(27). Another contributing factor is the gestational age of the majority aged 30-34 weeks. This gestational age is called the third trimester, at this time the fetus has grown large, the organs are complete and the pressure of the enlarged fetus is getting closer to the skin of the mother's abdomen. The hearing function of the fetus is getting better, being able to hear the sound of breathing, heart rate, intestinal peristalsis, as well as the mother's voice and sounds outside the mother's body that are in a place close to the mother. The more sounds heard and the stimulation of touch to the fetus will trigger the fetus to move. The movement of the fetus that is felt stimulates the mother to talk to and caress the fetus with great affection so that the emotional bond between the mother and the fetus becomes stronger(28). Relevant research on 213 pregnant women, pregnant women by feeling and counting fetal movements will further increase mother-fetus attachment. Pregnant women with a high level of attachment feel more frequent fetal movements(29).The results of the study prove that counting fetal movements has a positive effect on stronger maternal-fetal attachment(15). Counting fetal movements means that the mother feels the fetus when it moves and touches the abdomen where there is fetal movement. The activity of feeling the movement of the fetus shows the behavior of emotional attachment to the fetus. Mother's touch when the fetus moves, communicating with the fetus causes the fetus to respond with subsequent movements(14),(15).
Factors that supported the implementation of the research included the support of the coordinator of midwives at the Maternal and Child Health Service Unit who had collaborated in preparing respondents according to the criteria and no dropouts occurred. Respondents of pregnant women in the experimental group were enthusiastic about participating in the training, enthusiastically asked questions and followed the training instructions to carry out monitoring of fetal movements independently as evidenced by the results of the documentation of fetal well-being monitoring sheets that were filled in coherently. The limitations that occurred in this study, there were pregnant women according to the criteria who could not take part in the training due to work so that they needed additional time to find replacement respondents. Data on birth outcomes were obtained with a relatively long time lag because they had to wait for all respondents to give birth.
CONCLUSIONS
Generated audiovisual media independent monitoring of fetal well-being in pregnant women. The media is applied to pregnant women by providing training in monitoring fetal well-being so they can carry out monitoring of fetal well-being independently at home. In pregnant women who carry out independent monitoring of fetal well-being it is proven to simultaneously improve maternal-fetal attachment and birth outcomes with relatively normal fetal weight. The implications of this study corroborate previous findings that good maternal-fetal attachment improves health care practice and reduces the risk of adverse neonatal outcomes. All pregnant women need to be trained to carry out counting fetal movements to find out danger signs in the fetus, which also has a positive impact on increasing maternal-fetal attachment and birth outcomes.
REFERENCIAS
1. World Health Organization. Monitoring Health For The Sustainable Development Goals. Vol. 8, WHO. 2019. p. 55. [ Links ]
2. United Nations Development Programme. Sustainable Development Goals. 2020. p. 68-70. [ Links ]
3. Kemenkes RI. Rencana Aksi Kegiatan Direktorat Kesehatan Keluarga. 2020. [ Links ]
4. Kemenkes RI. Pedoman pelayanan antenatal, persalinan, nifas, dan bayi baru lahir. Direktorat Kesehatan Keluarga, Direktorat Jenderal Kesehatan Masyarakat Kemenkes RI; 2020. [ Links ]
5. Permenkes. Standart Teknis Pemenuhan Mutu Pelayanan Dasar Pada Standar Pelayanan Minimal Bidang kesehatan. In: Permenkes RI. 2019. p. 1-5. [ Links ]
6. Anjarwati A, Suryaningsih EK. The relationship between pregnancy-related anxiety and maternal-fetal attachment among primigravida. Open Access Maced J Med Sci [Internet]. 2021 May 11 [cited 2022 Dec 9];9:47-51. doi: 10.3889/oamjms.2021.6586 [ Links ]
7. Baltaci N, Baser M. Maternal-Fetal Attachment During Pregnancy and Nursing. In: Health Sciences Research in the Globalizing World [Internet]. 2018. p. 123-31. Available from: https://www.researchgate.net/publication/329885554 [ Links ]
8. Khalili Z, Navaee M, Shakiba M, Navidian A. The effect of a supportive-educational intervention on maternal-fetal attachment of pregnant women facing domestic violence: A randomized controlled trial. Iran J Psychiatry Behav Sci [Internet]. 2020;14(1). DOI 10.5812/ijpbs.92070 [ Links ]
9. Dokuhaki S, Heidary M, Akbarzadeh M. Investigation of the effect of training attachment behaviors to pregnant mothers on some physical indicators of their infants from birth to three months based on the separation of male and female infants. Pediatr Neonatol [Internet]. 2019;60(3):324-31. https://doi.org/10.1016/j.pedneo.2018.08.002 [ Links ]
10. Wada FH, Prabandari YS, Hapsari ED. Bonding and Attachment Experience among Postnatal Mothers with Spontaneous Childbirth. Belitung Nurs J [Internet]. 2020;6(1):14-20. doi: 10.33546/BNJ.779 [ Links ]
11. Røhder K, Væver MS, Aarestrup AK, Jacobsen RK, Smith-Nielsen J, Schiøtz ML. Maternal-fetal bonding among pregnant women at psychosocial risk: The roles of adult attachment style, prenatal parental reflective functioning, and depressive symptoms. PLoS One. 2020 Sep 1;15(9 September 2020):1-19. [ Links ]
12. Alhusen JL, Hayat MJ, Gross D. A longitudinal study of maternal attachment and infant developmental outcomes. Arch Womens Ment Health. 2013;16(6):521-9. [ Links ]
13. Maddahi MS, Dolatian M, Talebi A. Correlation of maternal-fetal atachment and health service during pregnancy with neonatal outcomes. Electron Physician [Internet]. 2016;8(7):2639-44. doi: http://dx.doi.org/10.19082/2639 [ Links ]
14. Malm MC, Hildingsson I, Rubertsson C, Rådestad I, Lindgren H. Prenatal attachment and its association with foetal movement during pregnancy - A population based survey. Women and Birth [Internet]. 2016;29(6):482-6. Available from: https://doi.org/10.1016/j.srhc.2021.100674 [ Links ]
15. Güney E, Uçar T. Effect of the fetal movement count on maternal-fetal attachment. Japan J Nurs Sci. 2019;16(1):71-9. [ Links ]
16. Hatini EE. Pendampingan Pengkajian Kesejahteraan Janin Pada Ibu Hamil Trimester III di Kelurahan Kereng Bangkirai. J Poltekkes Kemenkes Palangka Raya. 2018;8(4):152-7. [ Links ]
17. Memchoubi K, Ray S. Exploring The Experiences of Maternal Fetal Attachment Among Primigravida Women. In 2021. [ Links ]
18. Sudarmi. Efektifitas Media Audio-Visual pada Kelas Ibu Hamil Terhadap Pengetahuan dan Sikap Ibu dalam Pencegahan Komplikasi Kehamilan dan Persalinan. JKM Sai Wawai [Internet]. 2021;14(1):19-29. Available from: https://ejurnal.poltekkes-tjk.ac.id/index.php/JKM [ Links ]
19. Kristianti S, Suwoyo S, Pratiwi IY. Pengaruh Pendidikan Kesehatan Melalui Media Video Terhadap Kecemasan Persalinan Pada Primigravida Trimester III. J Midwifery Updat. 2020;2(2):84. [ Links ]
20. Parent S, Barrios R, Nosyk B, Ye M, Bacani N, Panagiotoglou D, et al. Impact of Patient-Provider Attachment on Hospital Readmissions Among People Living With HIV: A Population-Based Study. J Acquir Immune Defic Syndr [Internet]. 2018 Dec;79(5):551-8. DOI 10.1097/QAI.0000000000001857 [ Links ]
21. Dantas, Daniella Canejo; Fernada, Garcia, Bezerra Goes; Andressa, Silva Torres dos Santos; Aline, Cerqueira Santos Santana da Silva; Maria da ASLF da S. Production and Validation of Educational Video to Encourage Breastfeeding. Rev Gauch Enferm [Internet]. 2022;43:1-13. https://doi.org/10.1590/1983-1447.2022.202110247.en [ Links ]
22. Mariani M, Wahyusari S, Hikmawati N. Edukasi Prenatal Attachment Dapat Meningkatkan Kelekatan Ibu Dan Janin Pada Ibu Hamil Risiko Tinggi. J Ilm Perawat Manad. 2020;8(01):44-61. [ Links ]
23. Mohapatra S, Gomathi B, Nayak D. Effect of Fetal Movement Count Training (FMCT) on Prenatal Bonding and Maternal Anxiety among Primigravida Women. Int J Nurs Educ. 2021;13(3):119-25. [ Links ]
24. Castañeda J, SantaCruz H. Factores de riesgo asociados al embarazo en adolescentes. Enfermería Glob [Internet]. 2021;20(2):109-28. Available from: https://scielo.isciii.es/pdf/eg/v20n62/1695-6141-eg-20-62-109.pdf [ Links ]
25. Perry, SE; Lowdermilk DL; Hockenberry MJ; Wilson, D; Rodgers, K. Maternal Child Nursing care. Vol. Six Editio, Elseiver. 2018. 1-5018 p. [ Links ]
26. Qouta SR, Vänskä M, Diab SY, Punamäki R-L. War trauma and infant motor, cognitive, and socioemotional development: Maternal mental health and dyadic interaction as explanatory processes. Infant Behav Dev. 2021;63:101532. Available from: https://www.sciencedirect.com/science/article/pii/S0163638321000072 [ Links ]
27. Nakamura Y, Tsuno YS, Wada A, Nagasaka K, Kawajiri M, Takeishi Y. Occupational stress is associated with job performance among pregnant women in Japan : comparison with similar age group of women. BMC Pregnancy Childbirth [Internet]. 2022;3:1-8. https://doi.org/10.1186/s12884-022-05082-3%0A(2022) [ Links ]
28. Aprilia W. Perkembangan pada masa pranatal dan kelahiran. Yaa Bunayya. 2020;4(1). [ Links ]
29. Baltaci N, Baser M. Maternal-Fetal Attachment During Pregnancy and Nursing. In: Health Sciences Research in the Globalizing World. 2018. p. 123-31. [ Links ]
Received: April 29, 2023; Accepted: May 20, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
