










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
On-line version ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 n.1 Jan./Feb. 2006
ORAL SURGERY
Compressive osteotomes for expansion and maxilla sinus floor lifting
José Luis Calvo Guirado 1, Rosario Saez Yuguero 2, Guillermo Pardo Zamora 3
(1) Lecturer and Director of Implant Dentistry Course
(2) Senior Lecturer and Director of Implant Dentistry Course
(3) Associate Professor of Implant Dentistry Course. School of Dentistry. University of Murcia.
ABSTRACT
Aim: The aim of this article is to assess the efficiency of the
technique for the posterior alveolar expansion and elevation of the upper
maxillary alveolar ridge through the use of compressive osteotomes (Quirurgical
Bontempi, España) which have been specifically designed for Osseotite NT and
Osseotite NT Certain of 3i implants (Implants Innovations, USA).
Materials and methods: 24 adult patients (16 female and 12 male), who
were selected according to Albrektssons inclusion and exclusion criteria,
took part in the study. All the patients presented bone deficiency in the width
and height of the upper maxilla. 48 Osseotite implants were performed (four
Osseotite Standard; six Osseotite NT; 38 NT Certain (3i, Implants Innovations,
CA, USA)). Implant diameters were 4 mm in 44 cases and 5 mm in 4 cases with
lengths varying between 11.5 (n = 4) and 13 mm (n = 44). The alveolar ridges of
the 24 patients had initial widths from 1.5 mm to 5 mm and heights between 5 and
13 mm.
Results: The data obtained were analysed using the SPSS 11.0 program. In
the 48 areas treated with immediate implants, an increase in bone height of 6.75
mm ± 1.25 mm was achieved. In the case of the alveolar expansion for the 48
implants, the average was 3.2 mm ± 0.15 mm.
Conclusions: The technique for alveolar expansion and elevation of the
upper maxilla with compressive osseotomes can lead to a 100% success rate after
a 9-month follow-up of the implants and insertion of prostheses. It is a highly
predictable surgical procedure which allows implants to be performed at the same
time as surgery, thus reducing the number of such interventions while recovering
aesthetic and functional losses in the patient.
Key words: Osteotomes, alveolar expansion, osseotite, atruamatic sinus elevation.
RESUMEN
Objetivo: El objetivo de este artículo es evaluar la eficacia de la
técnica del ensanchamiento alveolar posterior y elevación del reborde alveolar
del maxilar superior mediante el uso de los osteótomos compresivos (
Quirurgical Bontempi, España) especialmente diseñados para los implantes
Osseotite NT y Osseotite NT Certain de 3i ( Implants Innovations, USA).
Material y métodos: En el estudio se incluyeron 24 pacientes (16 mujeres
y 8 hombres) siguiendo los criterios de inclusión y exclusión de Albrektsson,
que presentaban un déficit óseo en anchura y altura del maxilar superior. Se
colocaron 48 implantes Osseotite ( cuatro Osseotite Standard, seis Ossoetite NT
y treinta y ocho NT Certain (3i, Implantes Innovations, CA, USA). El diámetro
de los implantes fueron 44 de 4 mm y 4 de 5 mm con longitudes que variaban entre
11.5 (n=4) y 13 mm (n= 44). La cresta alveolar inicial tenía una anchura que
variaba de 1.5mm a 5 mm y una altura que oscilaba entre 5 mm y 13 mm en los 24
pacientes.
Resultados: Los datos obtenidos fueron analizados con el programa SPSS
11.0. En los 48 sitios tratados donde se colocaron los implantes inmediatos se
obtuvo un aumento de altura ósea de 6.75 mm ± 1.25 mm. En el ensanchamiento
alveolar de los 48 sitios implantados la media fue de 3.2 mm ± 0.15 mm.
Conclusiones: La técnica de ensanchamiento y elevación alveolar del
maxilar superior con osteótomos compresivos permite obtener un porcentaje de
éxito de un 100 % a los 9 meses de seguimiento en los implantes y prótesis
colocadas. Es un procedimiento quirúrgico con alta predictibilidad y además
permite la colocación los implantes en el mismo acto quirúrgico reduciendo el
número de cirugías, devolviendo la estética y función del paciente perdidas.
Palabras clave: Osteotomos, ensanchamiento alveolar, osseotite, elevación seno atraumática.
Introduction
In patients suffering partial or total tooth loss, the maxilla may present bone deficiency in both width and height for realisation of implants. Thus, a case-by-case study will not merely be limited to a real surgical possibility of performing an implant using the available bone, but rather to the creation of the alveolar ridge through bone grafts, guided tissue regeneration or bone enlargement procedures (1-10).
Another problem that we may encounter is that of the quality of the bone in the posterior upper maxilla area. This may be less dense, more medullar and thinner than in the jaw. A surgical procedure to overcome this inconvenience is that developed by Summers in 1994 (11, 12) which uses compression and compaction of the spongy bone of the upper maxilla.
Such defects are predominantly located along the upper maxillary ridge, although most commonly in the posterior toothless areas. Such cases involve patients with insufficient bone height and width (5 8 mm.), who, moreover, present a deficit of bone width of between 1.5 and 2.5 mm. Alveolar expansion using a 2mm diameter drill and compressive osteotomes of different heights (Quirurgical Bontempi, España, SL), enables separation of the vestibular and lingual or palatal corticals for the insertion of implants in order to achieve the 4-5 mm. width required. We can also achieve an important height up to 13 mm. In the majority of these cases, the implant surgery is performed at the same time as the ridge widening (13, 14).
Ridge widening with osteotomes aims to increase width and thus allow implants during expansion/enlargement surgery. Both when implants are immediate in a single surgical intervention and when they are deferred, the soft tissues can be manipulated to give a better emergency profile.
Materials and Methods
MATERIALS
Patients were rehabilitated using fixed single implant-supported caps or three piece bridges. 24 adult patients (16 female, 8 male) between 18 and 73 years were selected. 48 Osseotite implants were performed ( NT Certain = 38, NT = 6, Osseotite Standard = 4). All patients were in good health and were informed as to the risks and benefits the surgery entailed. Risks involved infection, pain and loss of bone, and implants. All the patients signed forms of consent. Smokers on over 10 cigarettes a day, those presenting uncontrolled diabetes and patients with bruxism habits were excluded from the study. All accepted 6-monthly checks and follow-up x-rays. All statistical data were processed using the program SPSS 11.0 for Windows. The diameter of the most used implants was 4 mm (n = 44), followed by 5 mm (n = 4), and length used was 11.5 mm (n = 4) and 13 mm (n = 44). Initial bone height ranged from 5 mm. to 13 mm. An initial bone width of 1.5 mm was found in 20 of the 24 subjects with 4 presenting 4.5 mm bone width. The teeth most replaced were the first upper molars and the second upper premolars. 17 immediate provisional caps were put in.
METHODS
SURGICAL TECHNIQUE WITH COMPRESSIVE OSTEOTOMES
Contemporary treatment of maxillary sinus elevation depends heavily on the height of the residual bone, the alveolar ridge and the height of the maxillary sinus floor.
We bring together the Bontempi Osteotones technique and the Misch Classification of maxillary sinus elevation (SA-1 to SA-4) with immediate insertion of the Osseotite NT and NT certain of 3i (Implants Innovations, Ibérica, CA, USA).
Treatment starts with an incision in the alveolar ridge in the centre of the bone crest using a cylindrical, handheld bur (num. 700) with external irrigation. A 1.5 mm bobe chanel is opened. The bur penetrates between the corticals until it reaches the spongy bone, at a depth of approximately 5 8 mm. It is important to reach the trabecular bone in order to avoid as far as possible any fracture of the buccal plate when beginning the technique with the osteotomes.
Initially a 2 mm bur is used. This penetrates to a depth of 2.5 mm in the spongy alveolar and allows insertion of the first, 4 mm high, osteotome, with a concave head.
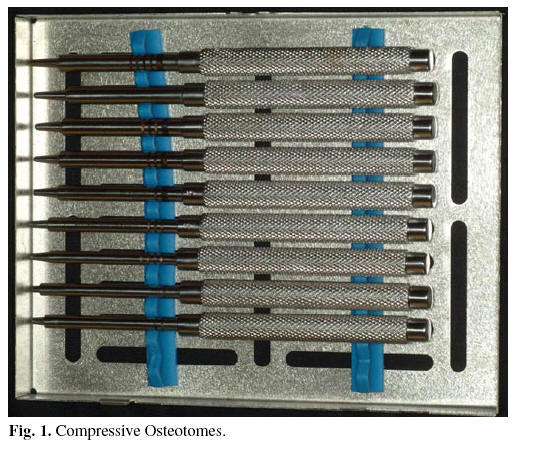
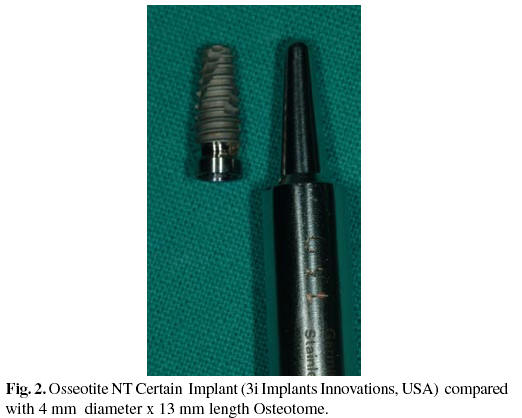
There are nine Bontempi osteotones, ranging from 4 mm to 13 mm in height, and can be convex or concave (Fig.1). The second osteotome to be inserted is a 5.5 mm convex one; the third is a 7 mm concave one; the fourth an 8.5 mm concave one; the fifth a 10 mm concave one: the sixth is a 10 mm convex one; the seventh an 11.5 mm concave one; the eighth is 11.5 mm and convex; the ninth a 13 mm concave one; finally, the tenth is osteotome is 13 mm and convex, which is similar to the 4 mm by 13 mm long Osseotite NT Certain of 3 i implant (Implants Innovations Ibérica, Palm Beach, CA, USA) (Fig. 2). Bone deficiencies must be filled with autologous bone from the patient or, in its absence, with biomaterial, in order to keep the bone corticals apart and to serve as scaffolding for the bone neoformation.
Cicatrization of the bone is controlled along with the taking of the graft and the implants by six-monthly x-rays (Fig. 3).
Six to seven months are allowed to pass for the complete osteointegration of the implant, and then the permanent prosthesis is put in.
Results
After clinical and x-ray control of the 24 patients the results were as follows. Of the 48 implants with sinus elevation with osteotones, 8 had an initial bone height of 5 mm. A final bone height of 11.5 mm was achieved, thus raising the maxillary sinus floor by 6.5 mm ± 0.16 mm. In the remaining 36 elevations the achieved bone height was 13 mm with an initial posterior alveolar ridge height of between 6 mm and 12 mm the average increase in the alveolar ridge height was 6.75 mm ± 1.25 mm.
As regards the width of the alveolar ridge, the minimum was 1.5 mm in 5 of the implant areas, 2 mm in 6 areas, 3 mm in 9 areas, 3.7 mm in 7 areas, 4 mm in 10 areas, 4.1 mm in 5 areas and the maximum 5 mm in 6 areas of implants. The widening of hte alveolar ridge in the 48 areas implanted was on average 3.2 mm ± 0.15 mm. All implants were rehabilitated with porcelaincrowns.
Discussion
Patients with partial tooth loss often offer stern challenges and severe limitations for restoration with maxillary implants. This is due mainly to the bone quality in that area. There is often low bone density. This was first classified by Albrektsson and Zarb, and later by Misch in 1989 (15, 16) who reported that the posterior area of the maxilla has a very thin cortical with thin trabecular bone. Jaffin and Berman reported a 35% greater loss of Branemark fixtures in Type D4 bone (17). In 1994, Scriponi et al. studied patients over a 5-year period following use of this technique of simultaneous Tübingen and IMZ implant placements. The results were 85.5% successrate in the former and 99% in the latter (18). Simion et al. (1992) reported five cases for five patients who underwent this treatment with guided bone regeneration (19). In 2000, Sehti A. and Kaus T. published a medium-term clinical study on osteotome technique and the placement of implants. There was a total of 449 implants and a ¡n average follow-up period of 27 months. Success rate was 97% (20). The frequent loss of bone in widening the upper alveolar ridge should be noted. In the study by Hallman, 41 subjects were assessed, of which 31 were edentulous, with resorption of the upper alveolar ridg. Hallman placed 182 implants with lengths between 8 and 12 mm, finding 4 periimplantitis and a mean resorption of between 0.35 mm. and 1.05 mm in the first year (21). Several authors have published on this subject, some with medium to long term studies in atraumatic sinus elevation, and with good aesthetic and functional results between 97 and 99% success rate, in line with those of Lange and Palti (22 30).
Conclusions
1. Bone widening with compressive osteotones (Quirurgical Bontempi, España) can increase the thickness of the ridge of atrophic maxillas by 4 to 6 mm with residual ridges of 1.5 to 2 mm.
2. Compressive progressive osteotomes are an ideal tool for the elevation of the atraumatic floor, with heights of up to 13 mm. being achieved in posterior upper areas in ridges with 5 to 8 mm. residual bone heights.
3. Filling of the space between the vestibular and palatal corticals should be performed with autologous bone or, in its absence, with some biomaterial which can be resorbed in at least 5 or 6 months, and which serves as scaffolding for the bone neoformation and prevents collapse of the alveolar tables.
4. The technique for alveolar widening and maxilla sinus floor elevation with compressive progressive osteotones is recommendable for the treatment of patients suffering partial or total tooth loss, and offers a high level of predictability. Success rates with the technique stand at 97 to 100%
![]() Correspondence
Correspondence
Prof. Dr. José Luis Calvo Guirado
Calle Mozart nº 1 , 1º esc. 1º G
CP. 30002. Murcia
E-mail: josecalvog@ono.com
joseluis.calvo@um.es
Received: 10-10-2004
Accepted: 2-11-2005
References
1. Adell R, Lekholm U, Gröndahl K, Brånemark P-I, Lindström J, Jacobsson M. Reconstruction of severely resorbed edentulous maxillae using osseointegrated fixtures in immediate autogenous bone grafts. Int J Oral Maxillofac Implants 1990;5:233–46. [ Links ]
2. Collins T. Onlay bone grafting in combination with Brånemark implants. Oral Maxillofac Surg Clin North Am 1991;3:893–902 [ Links ]
3. Nyström E, Kahnberg K-E, Gunne J. Bone grafts and Brånemark implants in the treatment of the severely resorbed maxilla: A 2-year longitudinal study. Int J Oral Maxillofac Implants 1993;8:45–53. [ Links ]
4. Buser D, Brägger U, Lang S. Regeneration and enlargement of jaw bone using guided tissue regeneration. Clin Oral Implants Res 1990;1: 22–32. [ Links ]
5. Nevins M, Mellonig JT. Enhancement of the damaged edentulous ridge to receive dental implants: A combination of allograft and Gore-Tex Membrane. Int J Periodont Rest Dent 1992;12:97–111. [ Links ]
6. Dahlin C, Lekholm U, Becker W, Becker B, Higuchi K, Callens A, et al. Treatment of fenestration and dehiscence bone defects around oral implants using the guided tissue regeneration technique: A prospective multicenter study. Int J Oral Maxillofac Implants 1995;10:312–8. [ Links ]
7. Augthun M, Yildirim M, Spiekermann H, Biesterfeld S. Healing of bone defects in combination with immediate implants using the membrane technique. Int J Oral Maxillofac Implants 1995;10:421–8. [ Links ]
8. Massimo S, Baldoni M, Zaffe D. Jawbone enlargement using immediate implant placement associated with a split-crest technique and guided tissue regeneration. Int J Periodont Rest Dent 1992;12:463–73. [ Links ]
9. Wilson DJ. Ridge mapping for determination of alveolar ridge width. Int J Oral Maxillofac Implants 1989;4:42–3. [ Links ]
10. Arx T, Cochran D, Hermann J, Schenk R, Buser D. Lateral ridge augmentation using different bone fillers and barrier membrane applícation. Clinical Oral Implants Research 2001;12:260-9. [ Links ]
11. Summers R. The ridge expansion osteotomy (REO). Compend Contin Educ Dent 1994;15:422–36. [ Links ]
12. Fugazzotto PA. Predictable restoration of the atrophic posterior maxilla. J Mass Dent Soc 2002;51:28-35-53. [ Links ]
13. Duncan JM, Westwood RM. Ridge Widening for the thin Maxilla: A clinical report Int J Oral Maxillofac Implants 1997;12:224-7. [ Links ]
14. Summers RB. The osteotome technique: Part 2 - The ridge expansion osteotomy (REO) procedure. Compend Contin Educ Dent1994;15:422-34. [ Links ]
15. Lekholm U, Zarb GA. Patient selection. In: Branemark P-I, Zarb G, AIbrektsson T, eds. Tissue-Integrated Prostheses: Osseointegration in Clínical Dentistry. Chicago: Quintessence Publishing 1985:199-209. [ Links ]
16. Misch C. Bone classification, training keys to implant success. Dent Today 1989 ;8:39-44. [ Links ]
17. Jaffin RA, Berman CL. The excessive loss of Branemark fixtures in type IV bone: A 5-year analysis. J Periodontol 1991;62:2-4. [ Links ]
18. Scipioni A, Bruschi GB, Calesini G. The edentulous ridge expansion technique : A 5 year study. Int J Periodontics Restorative Dent 1994;14:451-9 [ Links ]
19. Simion M, DaWin C, Blair K, Schenk R. Effect of different microstructure of ePTFE membranes on bone regeneration and soft tissue response: a histologic study in canine mandible. Clin Oral Implants Res1999;10:73-84. [ Links ]
20. Sethi A, Kaus T. Maxillary Ridge Expansion with simultaneous implant placement : 5- Year Results of an Ongoing Clínical Study. Int J Oral Maxillofac Implants 2000;15:491-9. [ Links ]
21. Hallman M. A prospective study of treatment of severely resorbed maxillae with narrow nonsubmerged implants: results after 1 year of loading. Int J Oral Maxillofac Implants 2001;16:731-6 [ Links ]
22. El Chaar E.Ridge augmentation for improved implant placement. Compend Contin Educ Dent. 1998 Dec 19;12:1193-8 [ Links ]
23. Coatoam GW, Mariotti A. The segmental ridge-split procedure. J Periodontol 2003;74:757-70. [ Links ]
24. Oikarinen KS, Sandor GK, Kainulainen VT, Salonen-Kemppi M. Augmentation of the narrow traumatized anterior alveolar ridge to facilitate dental implant placement. Dent Traumatol 2003;19:19-29. [ Links ]
25. Ataoglu H, Kucukkolbasi H, Ataoglu T. Posterior segmental osteotomy of maxillary edentulous ridge: an alternative to vertical reduction. Int J Oral Maxillofac Surg 2002;31:558-9. [ Links ]
26. Raghoebar GM, Batenburg RH, Reintsema H. Augmentation of the maxillary sinus floor and alveolar ridge for placement of endosseous implants in the edentulous maxilla. Ned Tijdschr Tandheelkd 1997;104:269-70 [ Links ]
27. de Lange GL, Kuiper L, Blijdorp PA, Hutter W, Mulder WF. Five-year evaluation of implants in the resorbed maxilla. Ned Tijdschr Tandheelkd 1997;104:274-6. [ Links ]
28. Bernhart T, Weber R, Mailath G, Ulm C, Dortbudak O, Watzek G. Use of crestal bone for augmentation of extremely knife-edged alveolar ridges prior to implant placement: report of 3 cases. Int J Oral Maxillofac Implants 1999;14:424-7. [ Links ]
29. Horowitz RA. The use of osteotomes for sinus augmentation at the time of implant placement. Compend Contin Educ Dent 1997;18:441-7,450-2; quiz 454. [ Links ]
30. Palti A, Steigmann M. Long term success with sinus elevation-criteria and parameters. Int Magazine of Oral Implantology 2004;4:20-4. [ Links ]

