










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Chronic heart failure (CHF) is a condition which leads to frequent hospitalizations, quality of life deterioration and high rates of mortality. Pharmacological treatment in CHF focuses on relieving symptoms (such as dyspnea or fluid retention), preventing readmissions and improving survival1.
The recommended CHF treatment combines renin-angiotensin-aldosterone system inhibitors, such as angiotensin-converting enzyme inhibitor (ACEI) or angiotensin-II receptor blockers (ARB), and beta-blockers. In refractory cases, the addition of aldosterone antagonists, such as spironolactone, is proposed. To relieve congestive symptoms, diuretics are used. This is reflected in the treatment algorithms of European1 and American Cardiology Societies2 .
Sacubitril/valsartan is a new drug for CHF treatment which inhibits neprilysin and blocks angiotensin-II type-I receptor. The Spanish Agency of Medicines and Health Products (AEMPs) published an assessment report (therapeutic positioning report) for sacubitril/valsartan3 on the basis of which, the Commission for the Rational Use of Medicines of the South of Seville Health Management Area (HMA) stablished some criteria for prescribing this drug. These criteria are: left ventricular ejection fraction (LVEF) <35%, New York Heart Association (NYHA) class II-III, and finally ACEI or ARB treatment during the last 4 weeks before starting sacubitril/valsartan without achieving adequate control of CHF symptoms.
The pivotal clinical trial (RCT)4 was a randomized, controlled and double-blind, multicenter trial comparing sacubitril/valsartan and enalapril. It included 8,442 patients with CHF with NYHA class II-IV and LVEF ≤40% (subsequently modified to ≤35%) on previous treatment with ACEI or ARB. The main combined variable was death and/or hospitalization due to CHF. The trial was stopped early (at 27 months of follow-up) because sacubitril/valsartan achieved a reduction of 4.7% for the combined end of death and/or hospitalization, reaching statistical significance (HR 0.8, 95% CI 0.73-0.87, p<0.001), as well as a significantly reduction of crude mortality (HR 0.84; 95% confidence interval 0.76-0.93, p<0.001).
However, this RCT presents some limitations of internal validity (unbalanced baseline characteristics between arms) and applicability (sacubitril/valsartan dose poorly tolerated in clinical practice and tolerant population selected by a run-in phase) which introduce a reasonable uncertainty about its reproducibility in real populations5. In addition, the economic impact of this treatment is high. Because of that, it is necessary to identify patients with the most favorable benefit/risk balance6.
The objective of this study is to evaluate the effectiveness and safety of sacubitril/valsartan for CHF treatment, as well as the adequation to the criteria of use recommended in the South of Seville HMA.
METHODS
This is an observational, retrospective study conducted in an HMA covering aproximately to 406,768 inhabitants. All patients older than 18 years with a diagnosis of CHF and undergoing treatment with sacubitril/valsartan between January-December 2017 were included. As exclusion criteria, previous or current participation in RCTs were considered.
Demographic (sex and age) and diagnostic variables (prescription physician, NYHA class and LVEF at the beginning of sacubitril/valsartan treatment and ACEI/ARB previous treatment) were recorded.
Mortality and/or hospitalization due to CHF at 12 months was stablished as main effectiveness variable. Some secondary variables were also defined: blood pressure (BP) control, symptomatic improvement of CHF at 12 months and NYHA class variation at 12 months.
To assess safety, adverse events (AE) and dose adjustment and/or treatment withdrawal during the study period was considered.
Overall adequation rate for sacubitril/valsartan treatment was evaluated by the percentage of compliance with these three items: LVEF ≤35%, NYHA class I-II and previous ACEI/ARB treatment.
Patients with an active sacubitril/valsartan prescription were obtained from the electronic prescription application available in the Andalusian Health Service. Data were collected from digital medical records. SPSS.v.21® was used for statistical analysis.
This study was approved by the Ethics Committee of the South of Seville HMA.
RESULTS
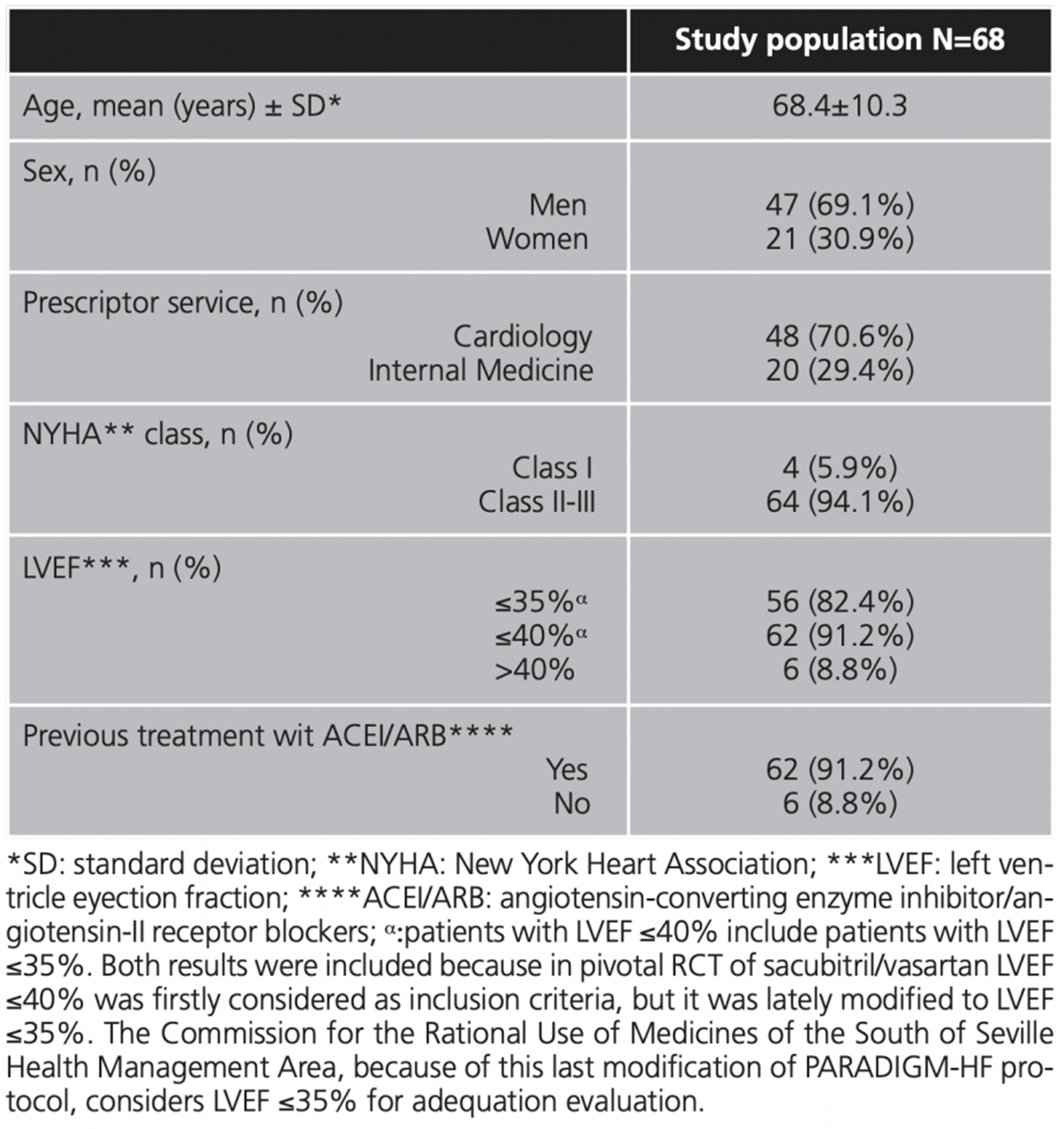
A total of 68 patients who met the inclusion criteria were recruited, whit a mean age of 68.4 years. Of them, 69.1% were men, mainly receiving therapy prescribed by cardiology department (70.6%). The rest of baseline features are shown in table 1.
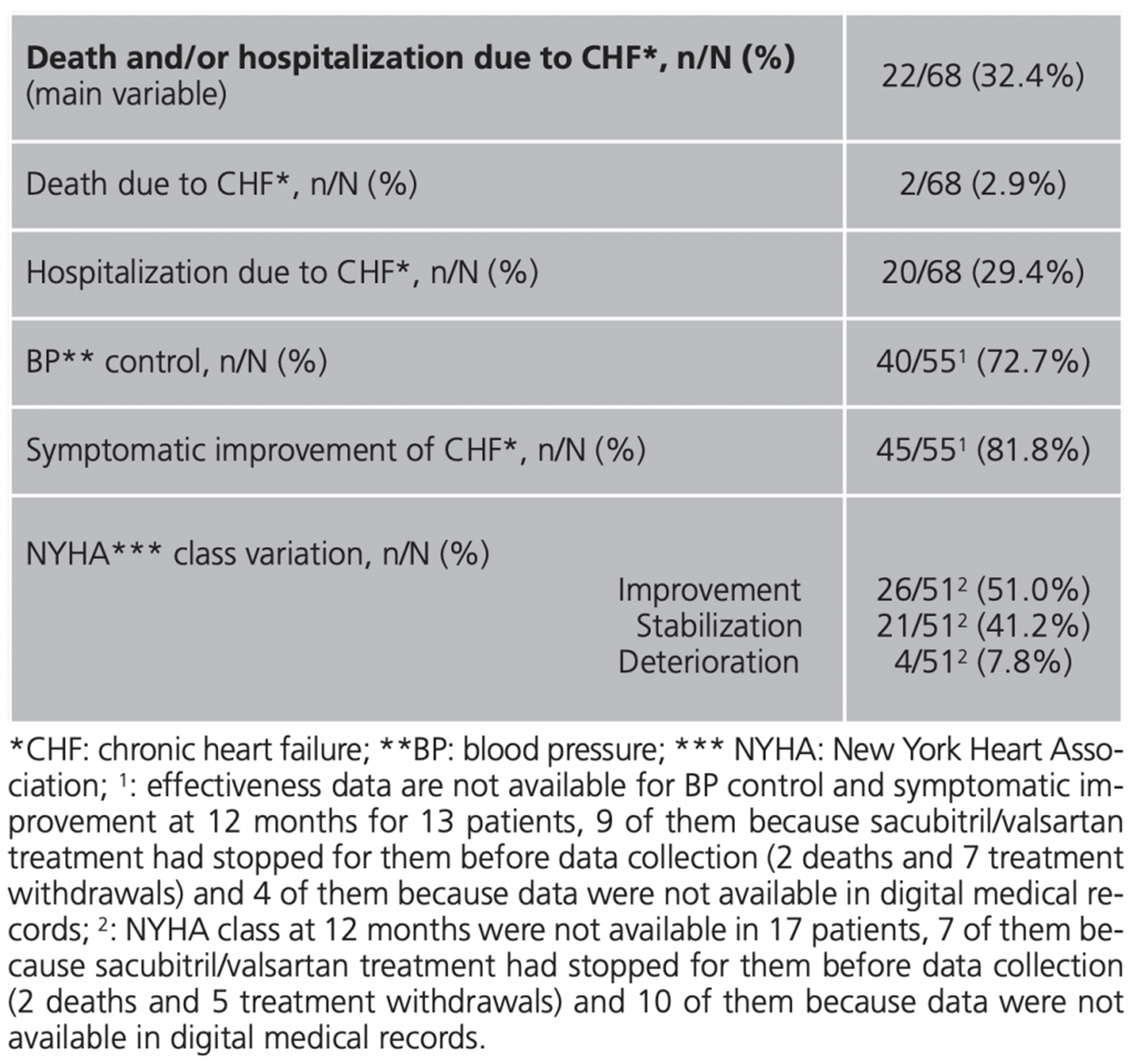
After 12 months of treatment, 22 patients (32.4%) had died and/or had been hospitalized due to CHF. All the effectiveness results at 12 months are shown in table 2.
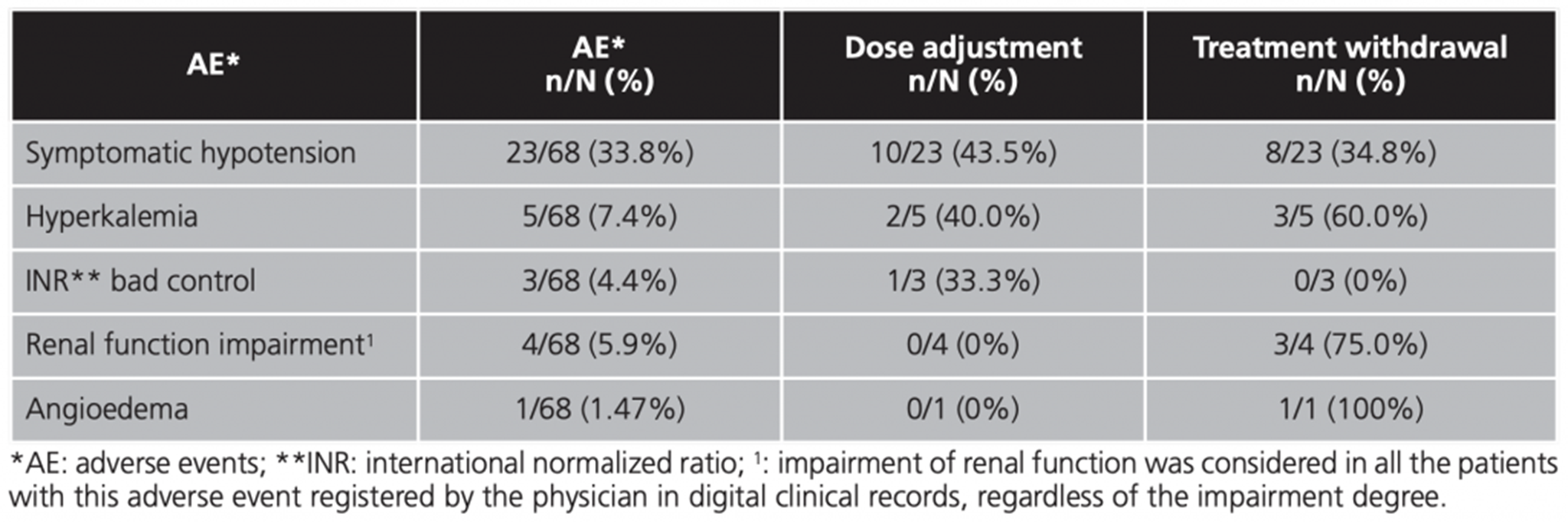
Adverse events observed during first 12 months of treatment, as well as need for dose adjustment and/or treatment withdrawal rates are shown in table 3. Hypotension was the most frequent AE (33.8% of patients, n=23).
Overall adequation rate was achieved in 46 patients (67.6%). Moreover, adequation for each individual item was as follow: LVEF ≤35% in 56 patients (82.4%), New York Heart Association (NYHA) II-III in 64 (94.1%) and 62 with previous angiotensin-converting enzyme inhibitor/angiotensin-II receptor blockers (ACEI/ARB) treatment (91.2%).
Since the RCT PARADIGM-HF presents several limitations5 and sacubitril/valsartan has an important economic impact in health services6, it is important to evaluate these real-life results. So far, this work is the first study which evaluates effectiveness and safety of sacubitril/valsartan based on the same variables which were stablished in the pivotal RCT4.
In our study, patients had a mean age higher than PARADIGM-HF patients (68.4 years vs. 63.8) and a proportion of men lower (69.1% vs. 78.2). The European Public Assessment Report of sacubitril/valsartan shows a value for the combined variable of death and/or hospitalization due to CHF at 12 months lower than 12%7 (extracted from PARADIGM-HF data), which is lower than ours (32.4%). This difference could be due to the differences in demographic patient's characteristics.
Higher prevalence of hypotension in real life is remarkable (33.8% after 12 months vs. 17.6 at month 27), and it is probably due to the run-in phase performed in the pivotal RCT4. Hypotension could be an important limitation in clinical practice. Thus, the rate of treatment withdrawal because of hypotension was 11.7% in our study vs. 0-9% in PARADIGM-HF4. Other treatments withdrawal rates in our population (compared to pivotal RCT results)4 were: 4.4% vs. 0.7 for acute renal failure and 4.4% vs. 0.3 for hyperkalemia.
Overall treatment adequation rate was acceptable (67.6%). The main reason for non-adequacy was a LVEF >35% in 17.6% of patients, but only an 8.8% of patients had a LVEF >40%.
In 2017, the Catalan Health Service published a retrospective study, including 2,179 patients and describing sacubitril/valsartan use. The 75% of patients were men (compared to 69.1% in our study) and the mean age of patients was similar than ours (69.8 vs. 68.4 years). All patients, except one, had previously received ACEI/ARB treatment and, in most cases, the lowest dose of sacubitril/valsartan was prescribed, probably due to concerns about hypotension in elderly population8. Moreover, a recent cohort study from the German IMS® prescription database showed that 2/3 of patients with sacubitril/valsartan was receiving low doses (50 mg/12 hours) and only 41% of patients were able to be dose-escalated9. This trend to maintain low doses could be an indicator of higher incidence of hypotension in real clinical practice.
Another recent observational study10 included 201 patients with the same inclusion criteria (NYHA ≥II, LVEF ≤35%, previous ACEI/ARB) which were followed during a mean (±SD) of 221±11.4 days. The proportion of men was higher than ours (82.0% vs. 69.1), while the mean age is similar (67.7 vs. 68.4 years). Regarding the variation in NYHA class at the end of the follow-up period (compared to our study), 32% vs. 51.0 of patients had improved, 64% vs. 41.2 remained stable and 4% vs. 7.8 had worsened.
The main limitation of this study is the inclusion of a local population; thus, results might not be representative of other different populations. Furthermore, its retrospective design and the limited follow-up period are also limitations. However, these results could be useful for demonstrating the effectiveness and safety of sacubitril/valsartan in real life clinical practice, considering the same variables as pivotal RCT.
CONCLUSION
In our study, the percentage of mortality and/or hospitalization due to CHF during the first year of sacubitril/valsartan treatment is high. In addition, hypotension is a frequent adverse event, hypotension is a frequent adverse event, which forces extreme precautions in its use and even to withdraw it occasionally. The adequation of sacubitril/valsartan prescription in the South of Seville HMA is acceptable.
Funding: The present investigation has not received specific aid from agencies from the public sector, commercial sector or non-profit entities.
Conflicts of interest: The authors declare no conflicts of interest.

