










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
On-line version ISSN 2173-2345Print version ISSN 1889-836X
Rev Osteoporos Metab Miner vol.11 n.1 Madrid Jan./Mar. 2019
https://dx.doi.org/10.4321/s1889-836x2019000100006
Review
Free vitamin D: an increasing determination
1Unidad de Gestión Clínica de Endocrinología y Nutrición - Centro de Investigación Biomédica en Red de Fragilidad y Envejecimiento Saludable (CIBERFES) - Instituto Maimónides de Investigación Biomédica de Córdoba (IMIBIC) - Hospital Universitario Reina Sofía - Córdoba (España)
2DIAsource ImmunoAssays - Louvain-la-Neuve (Bélgica)
Vitamin D has long been a familiar concept for any professional working in clinical biology. Nowadays it is becoming known to a large sector of the population. The great research efforts developed over the past decade have led to an explosion in the number of determinations requested of the most qualified metabolite to express the body state of vitamin D, 25-OH vitamin D (25-OHD) free, represents the small fraction not bound to transporter proteins. According to the free hormone hypothesis, it should be considered the best representation of the body state of vitamin D. Unfortunately, limited attention has been paid to this determination since, until recently, the scientific community only had tedious, indirect methods to measure it. A few years ago, a direct measurement method of free 25-OHD was already available to carry out research studies with promising results.
Key words: colorectal cancer; aging; osteoporosis; pregnancy; infertility; 25-hydroxyvitamin D; 25 hydroxyvitamin D free; 1,25-dihydroxyvitamin D
INTRODUCTION
In recent decades, vitamin D has attracted growing interest, not only in the medical field, but also among the general population. Initially, the evaluation of vitamin D was part of bone metabolism assessment when, for example, rickets or osteomalacia were suspected, or in populations at risk of osteoporosis1. 25-hydroxyvitamin D (25-OHD) is the circulating metabolite of higher concentration and longer half-life, used to monitor the body status of vitamin D. Patients with chronic kidney disease and undergoing dialysis treatment are also controlled by measurements of the evaluation of this state2. In this case, in addition to 25-OHD, the active metabolite of vitamin D, 1,25-dihydroxyvitamin D (1,25- (OH) 2D), produced mainly in the cells of the proximal tubule of the nephron.
In the past, vitamin D measurements made by laboratories were limited and almost always for research purposes. For about ten years the situation has changed. The request for determinations has drastically increased and more than 4,500 articles on vitamin Dare currently published every year, and the general public has been sensitized. This is due to the knowledge of the involvement of vitamin D metabolites in multiple physiological processes4, its association with various diseases and the dissemination of clinical studies, as well as the dissemination of the concept of 'vitamin of the sun' for the general population.
Currently, about 90% of the determinations requested and carried out in the laboratory refer to the total 25-OHD form. A concentration below 20 ng/mL is accepted as a deficiency, and a concentration below 30 ng/mL is considered insufficient. The ideal levels are higher than 30 ng/mL, while the toxicity levels are above 100-150 ng/mL. This topic is currently the subject of debate, and real cases of intoxication have been described, mainly due to formulation errors and/or errors in the daily intake5,6. The remaining 10% of the requests for metabolites of vitamin D are from the active metabolite, 1,25- (OH) 2D, which are largely requested by mistake, due to confusion between both metabolites by the prescriber7. These test results, carried out to evaluate the vitamin D endocrine system in healthy and sick populations, remain controversial for numerous reasons8.
Several new trials have been developed to facilitate the work of researchers and clinicians. The C3 epimer, a stereo-isomer of 25-OHD, can now be easily measured by liquid chromatography-mass spectrometry (HPLC-MS/MS), although its clinical importance is not clearly understood9. 24,25-dihydroxyvitamin D (24,25(OH) 2D), which is a catabolite of 25-OHD, can also be measured by HPLC-MS/MS methods, and is useful in the diagnosis of idiopathic childhood hypercalcemia10. The measurement of bioavailable and free 25-OHD levels have also been incorporated as new markers of vitamin D status and, although the concept has been known since the 1980s, it has not been used regularly, due to the lack of an adequate method for its quantification11.
PHYSIOLOGY OF FREE VITAMIN D
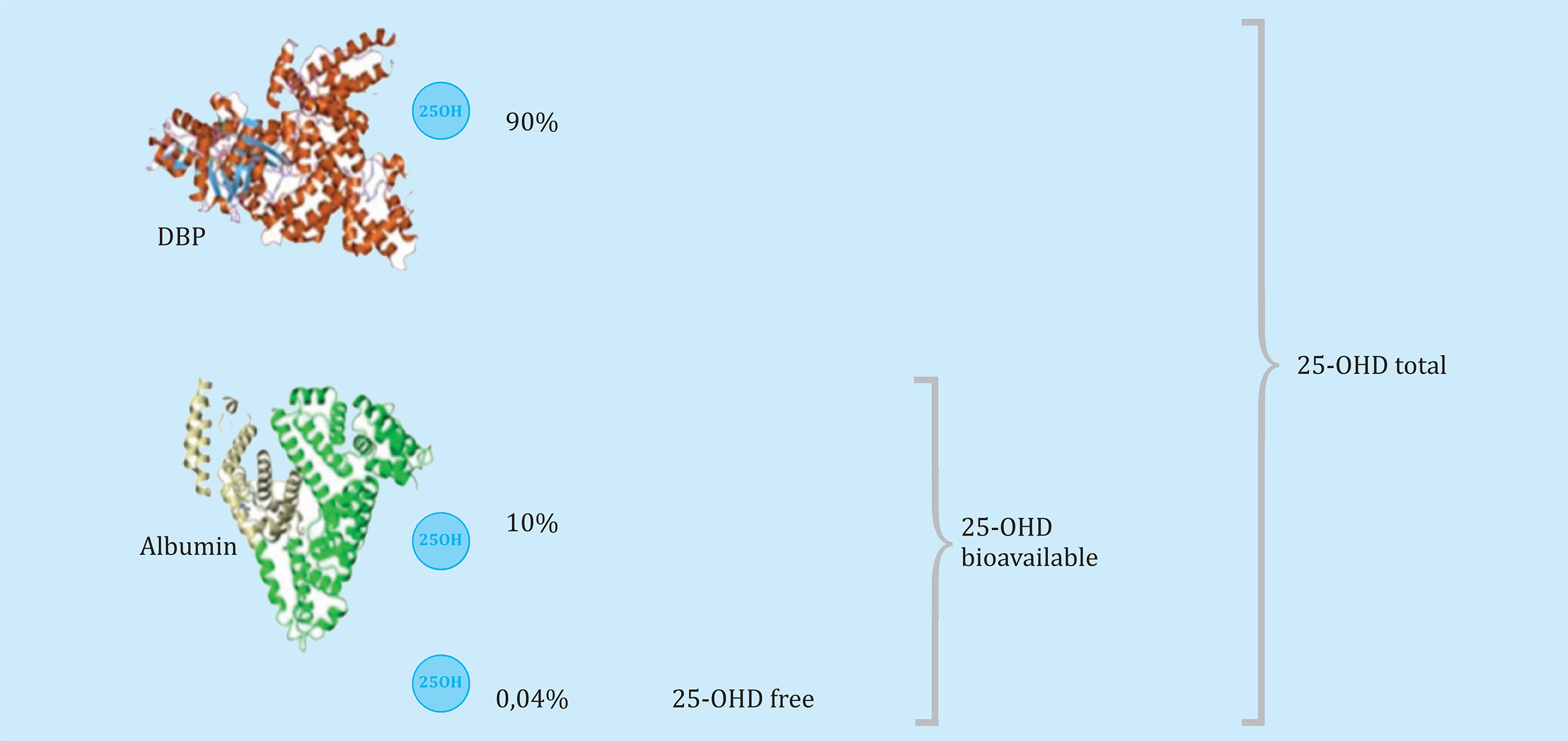
The free 25-hydroxyvitamin D (free 25-OHD) represents the fraction of 25-OHD that is not bound to vitamin D binding proteins. Due to its hydrophobic nature, the metabolites of vitamin D, especially 25-OHD, bind to transporter proteins. The main one is the vitamin D binding protein ((VDBP or DBP), also known as GC-globulin, which binds to all the metabolites of vitamin D but with greater affinity for 25-OHD, binding approximately 90% of its circulating concentration. Albumin, due to its high concentration in blood, although with a much lower affinity than VDBP for 25-OHD, binds the remaining 10%12. A small fraction, less than 0.1% of the total, circulates freely, and not bound13. The sum of free 25-OHD and the bound fraction to albumin is called bioavailable 25-OHD, since it is believed that the low-affinity albumin-25-OHD complex allows 25-OHD molecules to be readily available for produce their biological effects14. However, this concept tends to be abandoned in favor of the free hormone hypothesis (Figure 1).
FREE HORMONE HYPOTHESIS
The hypothesis of the free hormone states that a hormone´s biological activity is affected by its concentration not linked to protein (free) instead of the concentration bound to plasma proteins. In 1989, Mendel proposed that this hypothesis "is probably valid with respect to all tissues for thyroid hormones, cortisol and hydroxylated metabolites of vitamin D"15. Later, Chun et al.16 conjectured that "the binding of 25-OHD to VDBP hinders the delivery of 25-OHD to the target tissues, which ultimately prevents its metabolism to the active form, 1,25- (OH) 2D On the contrary, it is the unbound and free form that can pass through the cell membrane and, therefore, exercise the biological actions "(Figure 2).
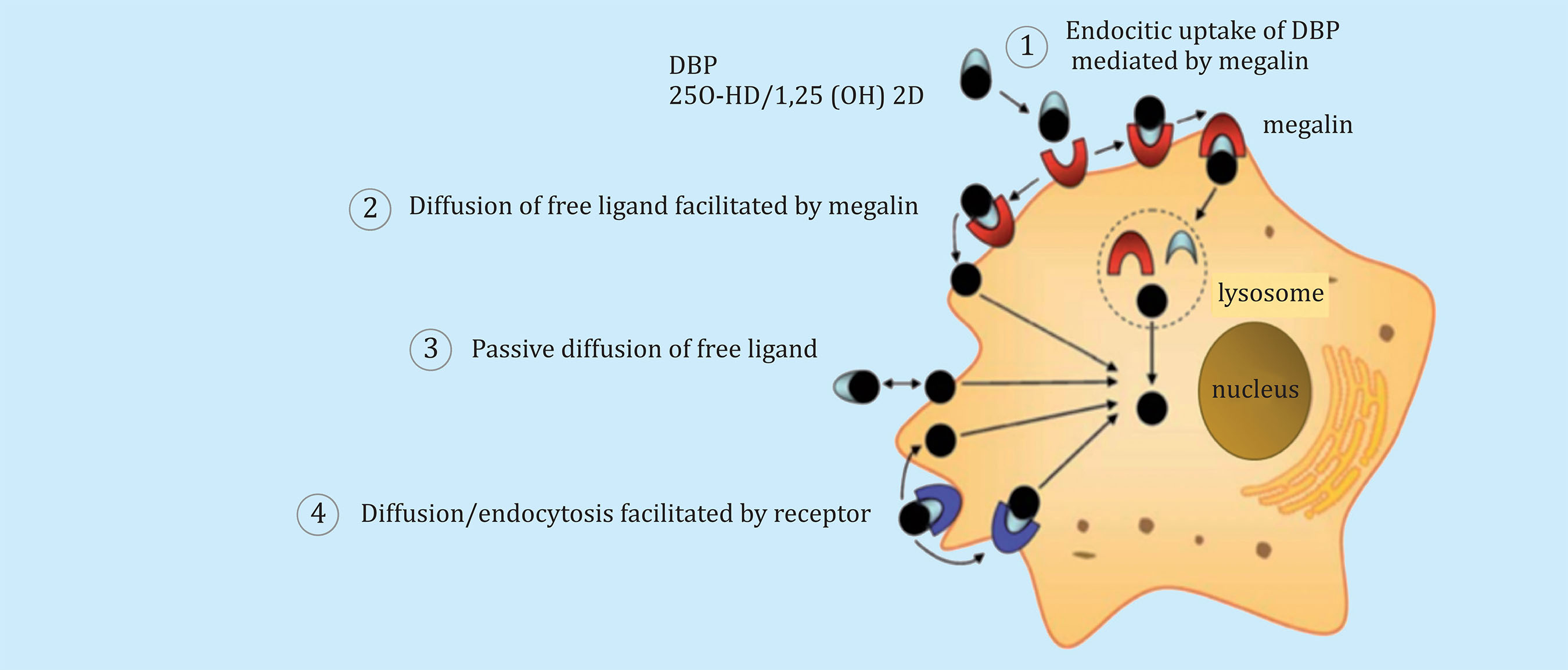
Figure 2. Transport mechanisms: Mechanisms mediated by membrane receptor and receptor-independent for the cellular uptake of vitamin D. Vitamin D metabolites bind to DBP in serum and extracellular fluid. The entrance to the cell of metabolites vitamin D can occur through one of the different mechanisms of the four described in the scheme
This free hormone hypothesis has been validated clinically for thyroid hormones, with the emergence of trials for free T3 and T4. These trials have replaced in practice most of the total T3 and T4 determinations that were previously made in clinical laboratories17. The story is similar, although to a lesser extent, for testosterone and cortisol18. For vitamin D, the situation is somewhat different, as the metabolite measured (25-OHD) is not the hormonally active form (it is 1,25- (OH) 2D). However, as Chun et al.16 previously reported, the conversion of 25-OHD to 1,25- (OH) 2D, and, consequently, the biological activity of vitamin D, is highly influenced by the concentration of 25-OHD free in the plasma.
METHODS FOR THE MEASUREMENT OF FREE 25-OHD
Historically, free 25-OHD and 1,25- (OH) 2D metabolites were measured by centrifugal ultrafiltration and equilibrium dialysis using the tritiated metabolite, which constitutes the classical immunoassay for the measuring total concentrations. Simple equations have been used to calculate the free hormone concentration19 and, although these methods provide reliable results, they are extremely complicated to assemble. They require considerable time and a large sample volume, in addition to involving the handling of material marked with tritium and/or carbon-14. Therefore, other methods of quantification have been developed over time, based on the measurement of the total metabolite of vitamin D and the binding protein concentrations, using the related affinity constants20. While in clinical laboratories the quantification of albumin and total 25-OHD are part of the routine analysis, the quantification of VDBP is based on kits for use only in research (Research Use Only, RUO), usually not validated. Trials using monoclonal antibodies have proved unreliable, since they do not measure the different polymorphisms of VDBP equally.
However, trials and techniques that employ radial immunodiffusion using polyclonal antibodies produce excellent results20. As different VDBP forms are found in the different serum samples to be evaluated, and although this is still a matter of debate since these different forms have different binding coefficients for 25-OHD, the calculation of each sample should ideally include the genotyping of the patient to use the appropriate coefficient21. In clinical practice, this is done very exceptionally (Figure 3).

Figure 3. Calculation of 25-OH of free vitamin D. BC: binding coefficient. DBP: vitamin D transporter protein
In 2017, a new direct method was developed and made available to the scientific community. The amount of free 25-OHD is measured by the enzyme-linked immunosorbent assay (Enzyme-Linked ImmunoSorbent Assay). The separation of the free and bound forms, as well as the capture of the former, is achieved through the use of a monoclonal antibody (anti-25-OHD), altering as little as possible the balance between both forms22, having validated the precision, sensitivity, accuracy and specificity of the assay.
On the other hand, this methodology generates results similar to those obtained by centrifugal ultrafiltration and has been used successfully in many clinical studies. The test obtained the European Union (CE) European Union mark of conformity in 2018, which allows its use in in-vitro diagnostic laboratories (IVD).
25-OHD FREE IN CLINICAL STUDIES
Recently, Tsuprykov et al.23 published a direct measurement method for free and total 25-OHD in a cohort of 297 healthy pregnant Caucasian women (gestational age ranged from the fourth week to the fortieth week), along with the 25- Total OHD, and other parameters (Table 1). Free 25-OHD correlated better than the total with various parameters, so it was concluded that optimal monitoring of vitamin D status in pregnant women should consist of free 25-OHD measurements at the beginning and end of pregnancy.
Table 1. Metabolites of vitamin D 25-OH total vitamin D, 25-OH free vitamin D and 1,25 (OH) 2 vitamin D with pregnancy parameters and other biochemical parameters. In bold, the results are statistically significant

The same year, Franasiak et al. studied free 25-OHD in a small group of infertile patients24. Free 25-OHD was calculated using the DBP data obtained with an antibody-based assay, and showed statistically significant differences between the groups of infertile and control (6.3±2.9 pg/mL vs. 4.3±1.8 pg/mL), differences that were not observed for total 25-OHD (30.3±9.8 ng/mL vs. 28.9±8.7 ng/mL). These results are explained by the lower concentration of DBP in the infertile group, which influences the balance between the free and bound forms of 25-OHD. Although these data only represented a pilot study, they concluded that the quantification of total 25-OHD can be misleading when assessing the status of vitamin D in situations of infertility.
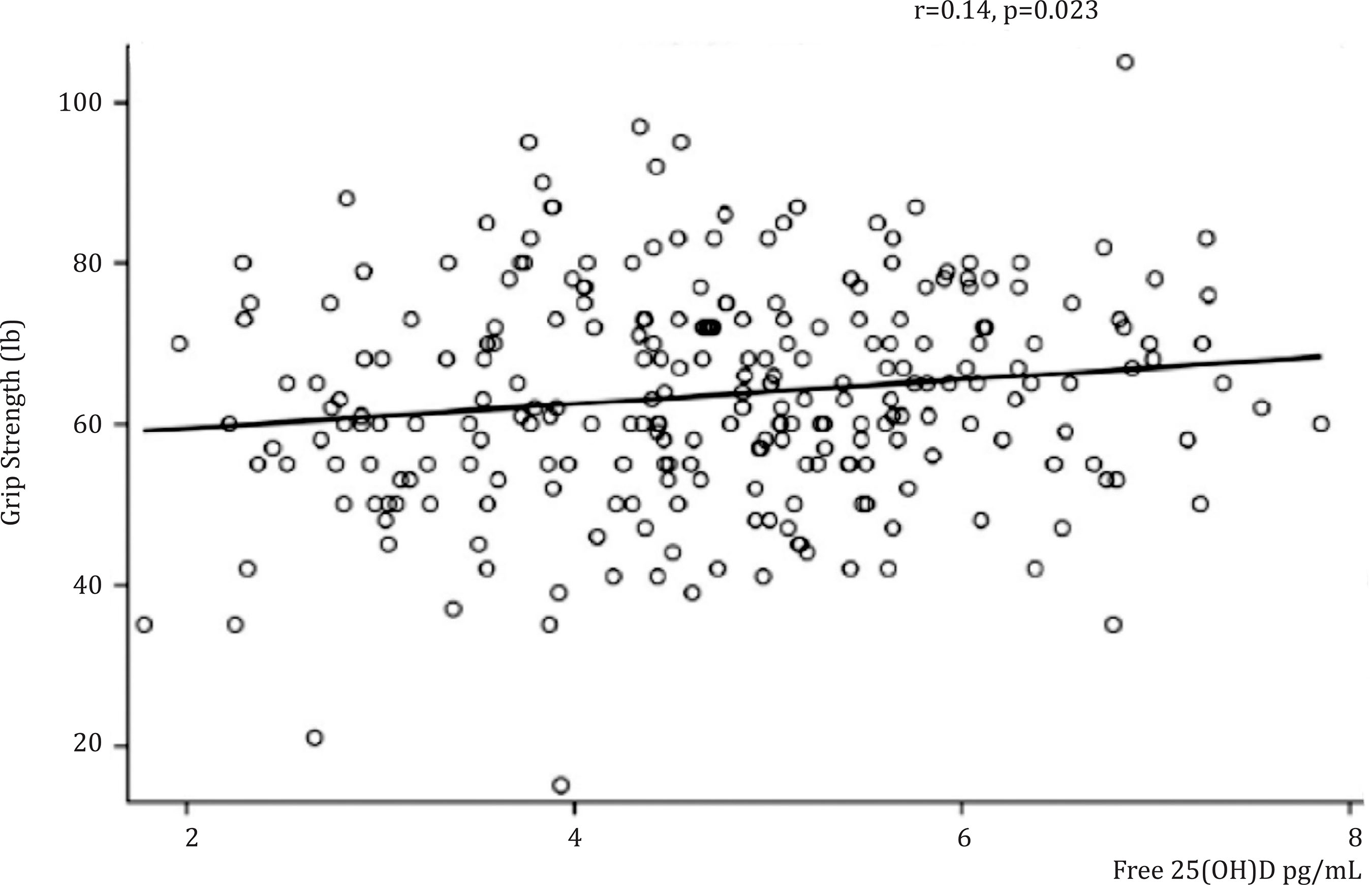
Free 25-OHD has also been studied in elderly healthy African-American women over 60 years of age25, analyzing the relationship between physical performance and osteoporosis prevention with vitamin D in this population. This is a 3-year, randomized, double-blind, placebocontrolled study that examined the effect of vitamin D on physical performance and bone loss in 260 women. Free 25-OHD significantly predicted the grip strength in a linear regression model (R2=0.02, F=5.22, regression coefficient [β]=1.52, p=0.023), suggesting that for each an increase of 1 pg/mL of free 25-OHD produced an increase in the grip strength of 1.52 lb, this association not being found for the total 25-OHD. These results suggest the usefulness of free 25-OHD as a predictor of physical performance with the aging of African-American women. The association of free 25-OHD with performance measures of the upper and lower extremities supports further examination of the role of serum-free 25-OHD in physical performance to prevent frailty and fractures in older adults (Figure 4).
Another application, in oncology, was proposed by the Yang group26. The aim of this study was to exhaustively evaluate the prognostic value of VDBP, total and free 25-OHD and its bioavailability in patients with colorectal cancer in stages I-III. The results showed that the elevation of free 25-OHD and its bioavailability was significantly associated with a better survival at 5 years, after carrying out a univariate statistical analysis. Upon completion of the study using a multivariate Cox analysis, they also found that high levels of free 25-OHD (HR=0.442, 95% CI=0.238-0.819, p<0.010) could be identified as an independent factor to predict better survival. In conclusion, the study suggested that higher levels of free and bioavailable 25-OHD were associated with greater survival in patients with colorectal cancer in stages I-III. In addition, free 25-OHD could be considered as an independent prognostic biomarker for survival. More recently, many other articles have been published, including reviews and clinical studies, which highlight the importance of free 25-OHD27.
CONCLUSION
Although the concept of free hormone and its physiological and clinical importance has been known for a long time, the free 25-OHD metabolite is still a relatively new subject of research. The absence of a direct measurement procedure has probably been one of the reasons for explaining this situation. With the direct immunoassay now available, the number of studies is growing rapidly and possible clinical applications are appearing in the literature. The true potential of this parameter has yet to be established in routine clinical practice, through broader clinical studies in relevant areas, mainly in pregnancy, fertility, renal and hepatic diseases, as well as in critical patients.
Bibliografía
1 Lips P, van Schoor NM. The effect of vitamin D on bone and osteoporosis. Best Pract Res Clin Endocrinol Metab. 2011;25:585-91. [ Links ]
2 Al-Badr W, Martin KJ. Vitamin D and kidney disease. Clin J Am Soc Nephrol. 2008;3:1555-60. [ Links ]
4 Feldman D, Pike JW, Bouillon R. Giovannucci E, Goltzman D, Hewison M (eds.). Vitamin D. Volume 1: Biochemistry, Physiology and Diagnostics. London; Elsevier Academic Press: 2018. [ Links ]
5 Benhamou CL, Souberbielle JC, Cortet B, Fardellone P, Gauvain JB, Thomas T, et al. La vitamine D chez l´adulte: recommandations du GRIO. Presse Med. 2011;40:673-82. [ Links ]
6 Lee JP, Tansey M, Jetton JG, Krasowski MD. Vitamin D toxicity: a 16-year retrospective study at an Academic Medical Center. Lab Med. 2018;49:123-9. [ Links ]
7 Dale JC. Common Test-Ordering Errors Part 1: Misordered Tests, http://www.mayomedicallaboratories.com/articles/hottopics/2010-04borderingtestspt1.html, consultada el 26 de abril de 2017. [ Links ]
8 Lucas RM, Gorman S, Black L, Neale RE. Clinical, research, and public health implications of poor measurement of vitamin D status. J AOAC Int. 2017; 100:1225-9. [ Links ]
9 Bailey D, Veljkovic K, Yazdanpanah M, Adeli K. Analytical measurement and clinical relevance of vitamin D(3) C3epimer. Clin Biochem. 2013;46:190-6. [ Links ]
10 Kaufmann M, Morse N, Molloy BJ, Cooper DP, Schlingmann KP, Molin A, et al. Improved screening test for idiopathic infantile hypercalcemia confirms residual levels of serum 24,25-(OH)2 D3 in affected patients. J Bone Miner Res. 2017;32:1589-96. [ Links ]
11 Chun RF, Nielson CM. Free Vitamin D: concepts, assays, outcomes, and prospects. In: Feldman D, Pike JW, Bouillon R, Giovannucci E, Goltzman D, Hewison M (eds.). Vitamin D. Volume 1: Biochemistry, Physiology and Diagnostics. London: Elsevier Academic Press; 2018. p. 925-37. [ Links ]
12 Pop LC, Shapses SA, Chang B, Sun W, Wang X. Vitamin D-Binding Protein in healthy pre- and postmenopausal women: relationship with estradiol concentrations. Endocr Pract. 2015; 21:936-42. [ Links ]
13 Bikle D, Bouillon R, Thadhani R, Schoenmakers I. Vitamin D metabolites in captivity? Should we measure free or total 25(OH)D to assess vitamin D status? J Steroid Biochem Mol Biol. 2017; 173:105-16. [ Links ]
14 Hewison M. Ligand regulation and nuclear receptor action. In: Bunce CM, Campbell MJ (eds). Nuclear Receptors. Current Concepts and Future Challenges. Dordrecht: Springer Netherlands; 2010. p. 381-417. [ Links ]
15 Mendel CM. The free hormone hypothesis: a physiologically based mathematical model. Endocr Rev. 1989;10: 232-74. [ Links ]
16 Chun RF, Peercy BE, Orwoll ES, Nielson CM, Adams JS, Hewison M. Vitamin D and DBP: the free hormone hypothesis revisited. J Steroid Biochem Mol Biol. 2014;144:132-7. [ Links ]
17 Shepherd HG. Practical clinical laboratory assessment of thyroid function today. Lab Med. 1974;5:9-12. [ Links ]
18 Faix JD. Principles and pitfalls of free hormone measurements. Best Pract Res Clin Endocrinol Metab. 2013;27: 631-45. [ Links ]
19 Bikle DD, Halloran BP, Gee E, Ryzen E, Haddad JG. Free 25-hydroxyvitamin D levels are normal in subjects with liver disease and reduced total 25-hydroxyvitamin D levels. J Clin Invest. 1986; 78:748-52. [ Links ]
20 Nielson CM, Jones KS, Bouillon R, Chun RF, Jacobs J, Wang Y, et al. Role of assay type in determining free 25-hydroxyvitamin D levels in diverse populations. N Engl J Med. 2016;374:1695-6. [ Links ]
21 Johnsen MS, Grimnes G, Figenschau Y, Torjesen PA, Almås B, Jorde R. Serum free and bio-available 25-hydroxyvitamin D correlate better with bone density than serum total 25-hydroxyvitamin D. Scand J Clin Lab Invest. 2014;74:177-83. [ Links ]
22 Heureux N, Lindhout E, Swinkels L. A direct assay for measuring free 25hydroxyvitamin D. J AOAC Int. 2017; 100:1318-22. [ Links ]
23 Tsuprykov O, Buse C, Skoblo R, Haq A, Hocher B. Reference intervals for measured and calculated free 25-hydroxyvitamin D in normal pregnancy. J Steroid Biochem Mol Biol. 2018;181:80-7. [ Links ]
24 Franasiak J, Shapses S, Sun W, Scott R, Wang X. Vitamin D binding protein is lower in infertile patients compared to fertile controls: a case control study. Fertil Res Pract. 2017;3:14. [ Links ]
25 Dhaliwal R, Mikhail M, Usera G, Stolberg A, Islam S, Ragolia L, et al. The relationship of Physical performance and Osteoporosis prevention with vitamin D in older African Americans (PODA). Contemp Clin Trials. 2018;65:39-45. [ Links ]
26 Yang L, Chen H, Zhao M, Peng P. Prognostic value of circulating vitamin D binding protein, total, free and bioavailable 25-hydroxy vitamin D in patients with colorectal cancer. Oncotarget. 2017;8:40214-21. [ Links ]
27 Heureux N. Vitamin D testing-where are we and what is on the horizon? Adv Clin Chem. 2017;78:59-101. [ Links ]
 Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
