










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkREC: Interventional Cardiology
On-line version ISSN 2604-7276Print version ISSN 2604-7306
REC Interv Cardiol ES vol.5 n.1 Madrid Jan./Mar. 2023 Epub Mar 18, 2024
https://dx.doi.org/10.24875/recic.m22000304
IMAGES IN CARDIOLOGY
Tratamiento de fístula arterial coronaria iatrogénica
Management of iatrogenic coronary artery fistula
Management of iatrogenic coronary artery fistula
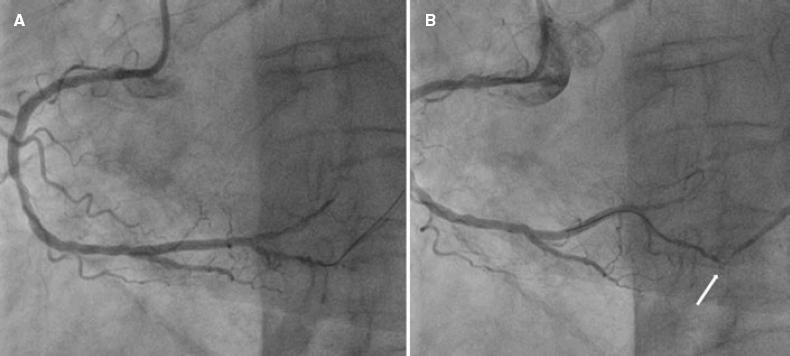
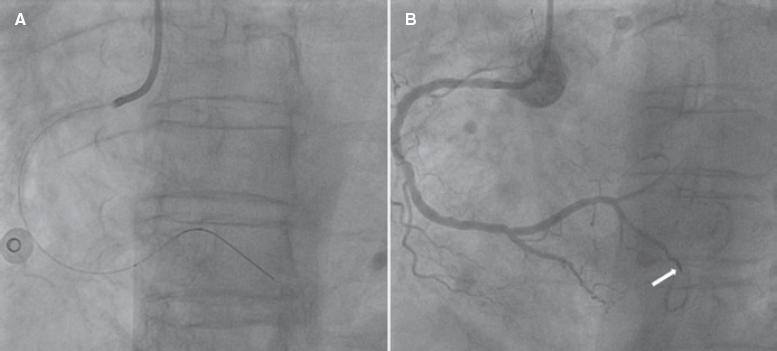
The authors describe the case of a 67-year-old woman who presented initially with an anterior ST-segment elevation myocardial infarction. Emergency coronary angiography revealed the presence of 95% stenosis in the middle segment of the left anterior descending coronary artery (LAD), and 90% stenosis in the middle segment of the right coronary artery (RCA). Primary percutaneous coronary intervention (PCI) of the mid LAD was performed. Two weeks later, elective PCI of the mid RCA was performed: we advanced a hydrophilic guidewire towards the distal RCA, predilated the lesion with a 2.25 mm × 15 mm balloon, implanted a 3.0 mm × 38 mm zotarolimus-eluting stent, and postdilated with 2.75 mm × 12 mm and 2.5 mm × 8.0 mm balloons. Although the angioplasty was successful, we observed contained contrast extravasation in a posterolateral artery branch (figure 1A,B; video 1 of the supplementary data). Echocardiography revealed no significant pericardial effusion. Coronary angiography reassessment performed 3 days later documented an Ellis type 3 coronary perforation with an evident fistulous tract to the venous system (figure 2; video 2 of the supplementary data). We advanced an Excelsior SL-10 microcatheter (Stryker, United States) towards the proximal end of the fistula (figure 3A) and delivered a 2 mm × 4 cm coil, which successfully occluded the vessel (figure 3B). There were no complications during hospitalization or at the follow-up.

Coronary artery perforation is a rare complication of PCI. Incidence rate is between 0.1% and 3.0%. Coronary perforations potentially result in severe complications like cardiac tamponade or arteriovenous fistula formation. Iatrogenic fistulae have a variable clinical course depending on the size and degree of left-to-right shunt. Treatment guidelines are not well established, and options reported include conservative, percutaneous or surgical management. Informed consent and authorization to publish these figures and videos were obtained from the patient.
Received: April 27, 2022; Accepted: May 17, 2022
 Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
