










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
The hernia is defined as an abnormal protrusion of an organ or tissue through a defect in its surrounding walls [1]. Interestingly, a hernia can occur at various sites in the body. These defects most commonly involve the abdominal wall, particularly the inguinal region. This clinical entity has remained a significant surgical burden to the General Surgeons worldwide, and especially in sub-Saharan Africa [1]. Indeed, hernias are known to be frequently responsible for morbidity and mortality in various parts of Africa [2, 3, 4, 5, 6, 7, 8].
Abdominal wall hernia repair is a highly prevalent surgical operation, which accounts for 15-18% of all surgical procedures at the typical surgical unit [1, 2, 3]. Similarly, an estimated 7 in 10 cases of all abdominal wall hernias occur in the groin, thus making inguinal hernias the most frequently occurring type of hernia [2, 3, 9, 10]. Therefore, the inguinal hernia has an incidence of 175 per 100,000. However, only a few fractions of these are repaired surgically [2, 11, 12].
Surprisingly, a significant body of knowledge has been acquired on the inguinal region anatomy from cadaver dissections in the nineteenth century. This development has enhanced tremendous progress in the surgery of inguinal hernias [13, 14]. Consequentially, the publications of surgeons such as Cooper, Franz Hasselbach, Antonio Scarpa, and Jules Germain Cloquet on the formation mechanisms and the management modality of inguinal hernia formed the basis of modern surgery [13, 14]. Most abdominal anterior wall hernias are inguinal hernias, followed by femoral and umbilical hernias, respectively [13, 14].
Various factors are contributing to the etiology of different types of hernia. These factors include, i) fundamental design weakness, ii) weakness due to structures entering and leaving the abdomen, iii) developmental failures, iv) genetic defect of collagen, v) sharp and blunt trauma, vi) weakness due to aging and pregnancy, vii) primary neurological and muscle diseases, and viii) excessive intra-abdominal pressure [15, 16]. The standard reasons for the repair of hernia include a) relief of symptoms, b) prevention of progression, and with further weakening of the anterior abdominal wall, c) preventions of complications such as acute incarceration and strangulation, d) addressing economic, employment, workers compensation issues, and e) treatment of incarceration and strangulation. Contraindications of repair of hernia include a) the presence of ascites, b) skin sepsis or other active infections, c) pregnancy, and d) reversible causes of increased intra-abdominal pressure—for example, prostatism, acute respiratory exacerbation and severe constipation [15, 16, 17].
Furthermore, the original description of inguinal hernia repair by Bassini was first published in 1887. The development has given rise to several other techniques for hernia repair, including Darning, Desarda, Modified Bassini, Shouldice, Lichtenstein mesh repair. Interestingly, laparoscopic repair is being advocated very lately in several works of literature [18, 19, 20, 21, 22, 23]. Besides, Laparoscopic and Lichtenstein mesh repair is both gaining popularity in recent times [23] mostly because of the benefit of a rapid return to normal activities, in addition to low recurrence rates [24]. Nonetheless, there have been concerns about the non-availability of mesh and laparoscopy in most centers in developing countries because of poor socioeconomic status and non-affordability by the patients. For these reasons, Laparoscopic and Lichtenstein mesh repair techniques for inguinal hernia are not accessible in the sub-Saharan African countries. Therefore, the traditional suturing techniques such as Shouldice, Darning, Desarda, and Modified Bassini are still practiced widely in this part of the world [25, 26].
Moreover, several challenges have been identified in the surgical management of groin hernias in our developing countries [2, 27, 28]. These limitations include i) delayed clinical presentation of patients, and ii) very inadequate privately-funded health care financing. The overall goal, therefore, is to maintain a balance between expensive cutting-edge techniques and an affordable surgical practice [2, 27, 28]. Subsequently, it is expedient to ensure adequate training for surgical trainees. The ultimate aim of any repair is a low perioperative complication profile that guarantees the largely predominant male population early return to a healthy lifestyle and work [2, 29]. There is no existing publication on abdominal wall hernias in our settings in particular. This study was therefore undertaken to describe the pattern, outcome, and our experience in the surgical management of anterior abdominal wall hernias in Shisong, Cameroon.
METHODS
The descriptive retrospective study was conducted at St. Elizabeth Catholic General Hospital, Shisong. The facility is a tertiary health institution situated in the Northwestern region of Cameroon. The various cases of various abdominal wall hernias performed in the hospital during the study period of three (3) years covering January 2017 to December 2019 by the surgical teams were included. We retrieved the case folders of all the adult patients with the clinical diagnosis of an external abdominal wall hernia seen in our surgical services during the study period. Relevant data, including the patients' sociodemographic information, clinical presentation, anesthetic, and surgical treatments, along with outcomes, were retrieved from the case files in addition to the detailed follow-up. The data were analyzed using SPSS Version 22.0. The findings were presented with descriptive statistics utilizing frequency distribution, percentages, range, mean, tables, and charts as appropriate. Continuous variables were compared by student t-test while proportions or specific parameters by chi-square test or two tail fisher's exact test as necessary. A P-value of ≤ 0.05 was considered statistically significant. The relationship between any two variables was, therefore, determined by Pearson's correlation coefficient.
RESULTS
During the study period of three (3) years covering January 2017 to December 2019, a total of 553 cases were operated for various abdominal wall hernias. Out of these, 88 cases were excluded as the records could not be retrieved for 28 cases, and the rest 60 cases comprised of congenital hydrocele for which herniotomy had been performed. Thus 465 cases of various abdominal wall hernias were included in this study. There were 82.4% males and 17.6% females.
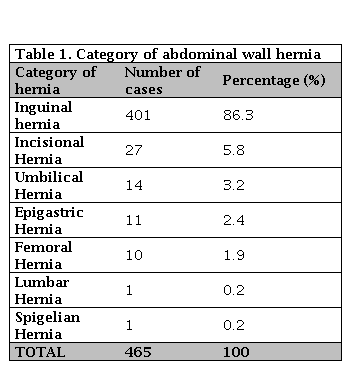
Inguinal hernia (86.3%) consisted of a majority of the series followed by incisional hernia (5.8%), umbilical (3.2%), epigastric (2.4%), femoral (1.9%) and lumbar and Spigelian (0.2% each) (Table 1).
The distribution of the groin hernias includes bubonocele, funicular, and complete inguinoscrotal hernia types were seen in 80 (32%), 60 (24%), and 95 (38%) patients respectively. In 15 patients (6%), the extent of groin hernia was not stated.
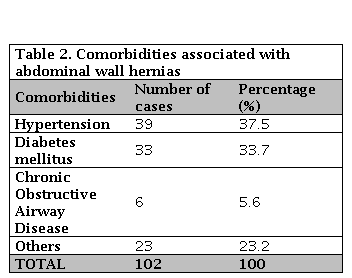
The range of common comorbidities associated with the study cohort includes Hypertension (37.5%), Diabetes mellitus (33.7%), and Chronic Obstructive Airway Disease (5.6%) based on Table 2.
Regarding the occupational status of the participants, most of the patients (64%) were artisans and farmers; therefore, they did not have any formal education.
The sub-arachnoid block was done in 352 (75.8%) patients, and this was the most prevalent form of anesthesia. Others were general anesthesia in 88 (18.8%) patients, total intravenous anesthesia in 2 (0.4%) patients, and local infiltration in 23 (5%) patients.
In this series, the various surgical procedures performed are outlined in Table 3, including herniotomy (8.7%), hernioplasty (38.7%), and herniorrhaphy (28.6%), which were done for various inguinal hernias. In contrast, only mesh repair (9%) was performed for epigastric, lumbar, umbilical, Spigelian, and incisional hernia.
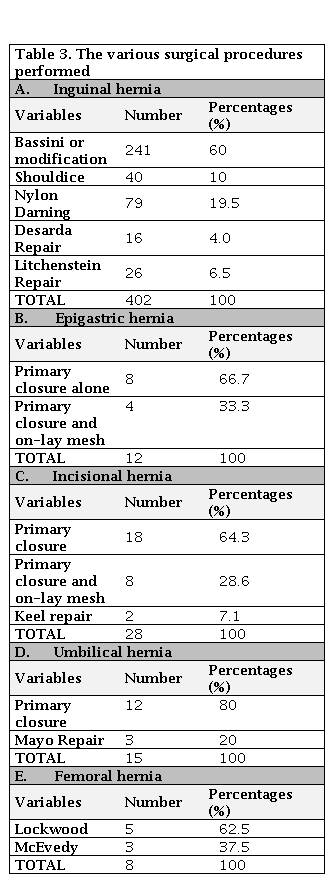
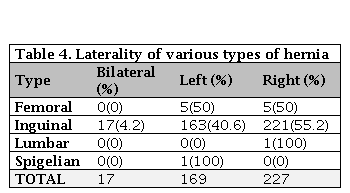
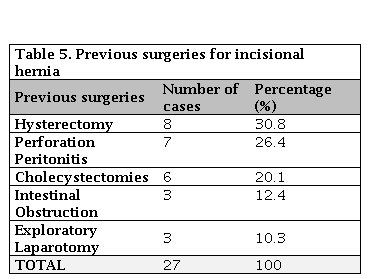
For the eight (8) cases of femoral hernia in our series, five (5) cases were approached via Lockwood inferior technique, and the rest 3 cases had McEvedy approach. Overall, the recurrence rate was nine (9) patients (1.9%) in our series, essentially were inguinal hernias. The bulk of inguinal hernia in our series was indirect inguinal hernia (217, 90.2%). Out of the 241 cases of inguinal hernia, 20 (8.4%) presented with strangulation, and 14 (5.8%) filed with features of obstruction and were thus tackled as an emergency. Amongst the inguinal hernias, 55.2% were right-sided, 40.6% were left-sided, and 4.2% were bilateral, whereas 50% each of femoral hernia was left and right-sided. in our series The only Spigelian hernia in the cohort was left-sided based on Table 4. Amongst the incisional hernias, 30.8% had a previous history of hysterectomy, 20.1% had cholecystectomies, 12.4% had intestinal obstruction, and 10.3% had exploratory laparotomy for various other reasons, and 26.4% had a history of perforation peritonitis in the past (Table 5).
DISCUSION
In this series, the plethora of clinical profile of external abdominal wall hernia is similar to what obtain in other previous studies [30, 31, 32]. Essentially, abdominal wall hernia repair constitutes a significant proportion of surgical workload in many centers in Africa [31, 32, 33, 34, 35].
Furthermore, from our study, we found a male preponderance concerning hernia presentations, whereby the male to female ratio is 4.6: 1 (82% to 12%). In another study, Gupta et al. [15, 36] reported 96% of male incidence. In contrast, Charles et al. [15, 37], in a study from Nepal, reported 93.2% of male preponderance in their education, which is similar to our findings. These reports concurred with the available body of evidence, which showed that more male is readily affected by external abdominal wall hernia in general. Because of several reasons including i) the anatomical difference in the pelvis between male and female demonstrating significant variation in the musculo-facial structure of the lower abdomen, coupled with ii) the varied descent of the gonads from their original embryonic retroperitoneal location [15, 38]. Besides, the male group usually engages in very strenuous activities, predisposing them to develop hernias, especially the inguinal type compare to their female counterparts [15, 38]. The later descent of the right testes and a higher incidence of failure of closure of processus vaginalis are factors usually described as responsible for the preponderance of the disease on the right [31, 39].
In a related development, our result showed that inguinal hernias comprised 86.3% of all abdominal wall hernias, which is similar to the 75% and 76.1% reported by Garba [10, 30] and Mabula et al. [3, 30] from Zaria (in Nigeria) and Tanzania, respectively. Meanwhile, inguinal hernia repair is one of the most frequently done procedures and contributes significantly to the surgical workload in many centers [4, 10, 30].
Some authors submitted that there is a robust association of inguinal hernia and low socioeconomic status. The opinion is based on the fact that inguinal hernia has been reported to be more prevalent in people of low socioeconomic class [30, 39]. The majority of our patients were artisans and farmers with no formal education confirming this submission. Other works of literature have reported a similar observation previously [30, 37, 38, 39, 40]. A compelling implication of the preceding is that consequent to financial constraint and a lack of awareness, most of our patients tend to present late with a giant inguinoscrotal hernia in our developing country settings [30, 40, 41, 42, 43].
In this study, most of our patients presented late after the onset of their symptoms resulting in complicated inguinoscrotal hernia similar to what was earlier described by other authors [7, 44, 45]. The other reasons for late presentations were well analyzed in an exhaustive study by Alegbeleye BJ [45] and Naeder et al. [7]. These factors include poverty, long-distance to care centers, scarce infrastructure, and poor health-seeking behavior," [46, 47, 48]. "This delay in presentation and surgical intervention frequently results in the relatively poor surgical outcome and prolong hospital stay" [46, 47, 48].
In a related development, Ayandipo et al. [2] in their study reported a comorbidity rate of 17.0%, while Mabula and Chalya [3] submitted a comorbidity rate of 16.8%; both rates are comparable to our finding of 22.0%. We equally observed that hypertension ranked highest in our review, similar to what was obtained by Ayandipo et al. but opposed to a chronic chest infection in Mabula and Chalya study [2, 3].
Complete inguinoscrotal hernia remains relatively common in our setting, therefore present in most of our patients. Meanwhile, the pick-up rate for incisional hernia is 5.8%, similar to 6-10% reported in the western countries [2, 19], but relatively higher than the estimated (1-4%) rates reported by other works of literature in Africa [2, 10, 49]. From our report, complications following obstetric and gynecologic surgical procedures are responsible for most incisional hernia in our series, this concurred with reports submitted by authors from south-western Nigeria [2, 50]. The umbilical hernia rate of 3.2% was within the 3-15% range quoted by other authors in sub-Saharan Africa [2, 32, 51].
Furthermore, in this series, the entire cases were managed by open herniorrhaphy technique, which is similar to other reports in developing countries [6, 10, 30, 39]. The bulk of reports emanating from the sub-Sahara Africa suggest that the most frequently adopted procedure for inguinal hernia repair technique across the continent has been Bassini [30, 52]. Nonetheless, another author found Nylon darning as the predominant method of repair [30, 53]. Besides, this Nylon darning is relatively tension free because the posterior wall is repaired without forcefully opposing the tissues [30, 53]. Surprisingly, several reports supported the claim that the darning technique has the advantage of a short learning curve, particularly when compared to other popular non-prosthetic methods of repair [30, 54]. For this reason, it is frequently performed by Surgical Doctors in training.
In addition to the previous, no laparoscopic repair was performed in this study, which is similar to other studies in most surgical facilities in our developing countries [6, 10, 30, 39]. Laparoscopic repair of external abdominal wall hernias, in general, is gaining momentum amongst General Surgeons worldwide. Evidence-based best practices in western countries suggest the superiority of Laparoscopic repair for treating inguinal hernias with the following range of benefits i)reduced morbidity, ii) shorter hospital stay, iii) accelerated recovery, and iv) earlier return to work [55, 56, 57, 58]. It is envisaged that as the facilities and requisite expertise are gradually made available, therefore, as soon .this modality of hernia repair may become feasible in our locality [55, 56, 57, 58].
Taking a critical look at the mode of anesthesia for herniorrhaphy is related to a) the physiological state of the patient, b) size of the hernia, and c) the extent of the perceived procedure, d) whether the procedure is day-case or not. [55, 56, 57]. Interestingly, day-case herniorrhaphy is generally adjudged as safe, feasible, and effective in our settings. Besides, they are usually associated with earlier ambulation when dealing with the uncomplicated average-sized hernia in a physiologically fit individual [55, 56, 57, 58].
Moreover, in our series, the most frequently used anesthesia was spinal anesthesia, which was closely followed by general anesthesia. In any case, reflecting the resultant treatment of very large and complicated hernias, that is, in contrast to the exclusive use of local anesthesia with sedation in a series of 98 hernia repairs by McFarlane [55-58] working on small, uncomplicated inguinal hernias[57, 58].
In our series, the bowel resection rate was 12.8%, which is relatively lower than the estimated 21% reported by Ajao in Ibadan [57] and 15.9% reported in Bugando, Tanzania [2, 3]. The implication of this is that patients present relatively earlier now than in the preceding decades. Besides, the need for bowel resection is related to the time interval between the onset of acute symptoms and hospital presentation [2, 3]. The complication rate of 8.6% in this study is in concordance with other estimates of the range 4.2% to 12% in other series [59, 60]. The complication rate was significantly higher in an emergency than elective herniorrhaphy.
Moreover, our finding of the median duration of hospital stay of 5.5 days is lower than the 7-9 days reported in other series [3, 6, 10]. The sole predictor of length of hospital stay was only emergency surgery, which implies that good outcome in hernia surgery is predicated on early elective patient presentation. There was no record of death related to herniorrhaphy in our study, which is a significant improvement when compared with other studies that reported a mortality rate in the range of 1-14% [6, 60].
CONCLUSION
The external abdominal wall hernia repair remains a significant burden to surgeons with attendant morbidity and mortality in our locality. Males were more commonly affected, and Bassini herniorrhaphy and modifications were the method of choice in the majority of cases operated. It advocated that early presentation and elective herniorrhaphy be encouraged to eliminate the risk associated with this condition.
Interestingly, Lichtenstein tension-free repair appears to be a choice technique among the open method of repair due to a significantly low recurrence rate. The adoption of newer modalities of care should be considered standard. However, in resource-constrained settings like ours in Cameroon, the goal should be to perform a skillful and technically effective technique. Also, it is critical to ensure adequate anesthesia for optimal post-operative pain control, coupled with minimal morbidity.

