










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
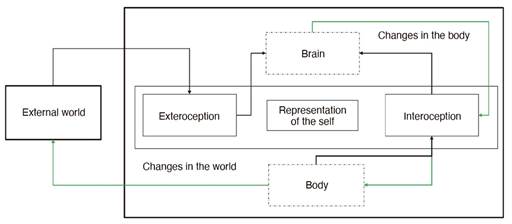
Cognitive neuroscience as an interdisciplinary approach has made enormous progress in understanding the neural basis of cognition and behavior in relation to the world. External stimuli, perceived and integrated by our nervous system, correspond to the exteroceptive system. But much of the sensory information processed by our system originates inside our body (interoception), which is not attributable to an external agent, thus generating two different sensory fields. It has also been accepted that interoception is the antonym of the external. In the sensory domain, that which is "external" encompasses the primary sensory systems of vision, hearing, smell, taste, and somatosensation (See Figure 1). The way these external perceptual processes have been defined has to some extent affected the functioning attributed to the interoceptive system, which can represent our internal world (Chen et al., 2021). Because of this, the label of "interoceptive" has yet to have an overarching concept (Ceunen, Vlaeyen, & Van Diest, 2016). The relevance of this issue is that a more inclusive meaning may involve this term across a spectrum of different areas of psychology and health. Within these areas, there is certainty of the existence of brain-body connections, along with the neural circuits underlying the dynamic interactions between the nervous and peripheral systems (Craig, 2002). However, a new review on this topic is occurring at a human/clinical research level. The present article considers current debates in interoception and aims to produce a broad overview of the research in this area, defining and delimiting its dimensions. It also seeks to review elements of interoceptive processing, measurement methods, to finally characterize the role of interoception in emotional processing.
Interoception: Characterization and Measurement
What is Interoception?
Interoception refers to the process by which we sense, integrate, and interpret information from signals originating from within the body, thus generating a global, moment-to-moment representation of the body's internal landscape at both conscious and unconscious levels (Khalsa et al. 2018). This mapping involves the integration of a relatively restricted set of information pathways associated with all the major biological systems that are involved in maintaining body homeostasis, including the cardiovascular (Oppenheimer & Cechetto, 2016), respiratory (Von Leupoldt et al., 2010), gastrointestinal, genitourinary, nociceptive, chemosensory, osmotic, thermoregulatory, visceral, immune, and autonomic systems (Craig, 2009). This interoceptive information is communicated through a set of distinct neural and humoral (i.e., transmitted via the blood) pathways with different signaling modes, which the brain represents, integrates, and prioritizes.
In turn, there is also a kind of communication between different physical axes and representations or dynamic maps of the internal state of the body that are generated not only at different anatomical and psychological levels, but also on different time scales. Therefore, there should be an integration of the different sensory information, as is the case with the exteroceptive systems. With this conceptual framework, it is possible to study interoception based on physiological body responses and representation at the brain level to the metacognitive perception of interoception associated with the conscious perception of internal signals (Quadt et al., 2018).
Interoception Complexity Levels
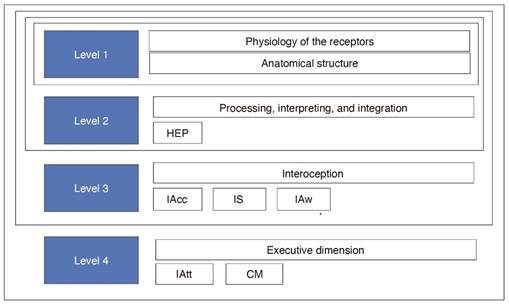
Interoceptive Signals and Sensory Processes. A first level of interoceptive complexity refers to the physiology of the receptors, regarding the transduction mechanism of the transmission of afferent signals from the internal organs (viscera) to the central nervous system and how this afferent information is represented and processed at the level of the central nervous system (Vaitl, 1996). Sensory information from different body organs and different types of visceroceptors converge in the nucleus of the solitary tract (NST) and its main target is the parabrachial nucleus (PB) (Craig, 2003). The PB is the main site of integration for all homeostatic afferent activity and is therefore essential for the maintenance of cardiovascular, respiratory, energy (food and glucose), and fluid (electrolytes and water) balances (Saper, 2002). Moreover, the PB projects to the periaqueductal gray matter (PAG; the mesencephalic homeostatic motor center) and the hypothalamus (the diencephalic homeostatic motor center), which guide goal-directed autonomic, neuroendocrine, and behavioral activity (Craig, 2003). In this sense, there is a neuroanatomical basis, and the functioning of part of the interoception process depends on the development and indemnity of these functional areas.
Processing, Interpretation, and Integration. A second level of complexity, reflects the impact of visceral afferent signals and other forms of sensory processing on cognitive processing and behaviors. This level does not necessarily include a perceptual awareness of interoceptive signals (Quadt et al., 2018). This dimension has been measured, for example, through cardiac synchronization experiments, where, it is possible to test, for example, an interaction and integration of sensory information, where interoceptive cues can modulate threat appraisal or even racially biased behavior in a context-dependent way (Azevedo et al., 2017).
From the Unconscious to the Conscious. A third level of complexity, refers more directly to the perception of interoceptive signals; the base model is the one proposed by Garfinkel and Critchley (2013) known as the tripartite model of interoception, which alludes to the psychological dimension and is composed of three facets of interoceptive ability, interoceptive accuracy understood as the accuracy with which one perceives one's internal state, interoceptive sensitivity as the subjective report of interoceptive cues, and interoceptive meta-awareness, understood as the correspondence between the above measures. These three dimensions have been measured through cardiac detection tasks (Quadt et al., 2018). Following this description, several variants of the model have been proposed (Khalsa et al., 2018; Murphy, Catmur & Bird, 2019), among these, a recent model stands out that posits the need to distinguish between interoceptive accuracy and attention towards interoceptive information (Murphy et al., 2019). From this, a 2x2 dimensional structure of interoception is proposed that reflects both what is measured (accuracy versus attention) and how it is measured (objective performance versus self-report) (Murphy et al., 2019). In this sense, Garfinkel and Critchley's (2013) tripartite model can be understood as the degree to which measures of accuracy and sensitivity (self-report) correlate with each other in both the objective and self-report dimensions (See Figure 2).
Interoception Measurement
Experimental Tasks. In general, it is recognized that the measurement of interoception represents a great challenge (Quigley et al., 2021) for two reasons; firstly, because of the difficulty of directly measuring and/or manipulating interoceptive signals in humans due to the fact that interoceptive afferences are fine, and they are diffusely dispersed, and secondly, there is a sort of multisensory integration in interoceptive modalities, consequently, although interoceptive signals are dissociated from each other they can also be associated with each other.
Interoceptive signals arise from four systems: cardiovascular, respiratory, gastrointestinal, and urogenital. Among these, the cardiovascular has emerged as the main focus of study of the interaction between viscera and brain (Critchley & Harrison, 2013), especially because of bidirectional connections between these two (Tsakiris, 2017). Most studies on interoception perception, based on the perceptual accuracy of internal signals, have been carried out by performance in heartbeat counting tasks. In this type of procedure, participants are asked to count their heartbeat, without any physical aid, over a series of intervals (Schandry, 1981). The measure of interoceptive sensitivity is considered as the difference between the objective measurement and the participant estimation. While this task is easy to implement, its validity has been repeatedly questioned. First, approximately 40% of normal individuals cannot consciously perceive their heartbeat (Khalsa et al., 2009), therefore, these measurements may not be suitable for quantifying interoceptive sensitivity in all individuals. Furthermore, heartbeat can also be perceived through the exteroceptive (such as chest wall vibration, among others), which may affect the degree to which heartbeats are perceived via the interoceptive pathway (Brewer, Murphy, & Bird, 2021).
Although the cardiac tests described above are the most commonly used measures to explicitly assess interoceptive ability, the idea of assessing more interoceptive domains that are less explicit than cardiac signals is highlighted. However, it must be noted that every existing task that assesses interoceptive accuracy will have its own limitations regardless of the modality.
Interoception in Mental Health
The starting point of this section is that atypical interoception is associated with impairments in different psychological processes, and furthermore, these impairments are points of convergence that characterize a wide range of conditions in the field of psychopathology (Barrett & Simmons, 2015; Murphy et al., 2017; Khalsa et al., 2018). Below, we seek to set out an overview around the role of interoception in emotional processing.
The Role of Interoception in Emotional Processing
Conscious emotional experience is closely linked to changes in bodily sensations. Moreover, emotional experience must be, by its nature, physiological (Pace-Schott et al., 2019). By way of summary, early theorists of interoception associated it with emotional processes, suggesting that emotions were the result of physiological reactions to events in the environment (James, 1884). Subsequently, Damasio (1994) proposed that physiological reactions and their emotional responses together result in somatic markers that can inform future decision making. Along with this, the literature addresses the issue that interoceptive and emotional processes share underlying neural substrates. Moreover, emotional impairments accompany most mental disorders (Quadt et al., 2018) acting as a possible pathway linking interoception to mental health.
Neuroimaging studies support the notion that interoception and emotion are intertwined (Wiens, 2005; Herbert & Pollatos, 2012), likewise, both processes are carried out in overlapping brain structures such as the insula and the anterior cingulate cortex (Craig, 2008). Along these lines, Craig (2002) suggests that interoception should be redefined to reflect both the physiological condition of the body, as well as the perception of the body's response to different stimuli and their impact on one's emotional experience. This suggests that greater accuracy in the perception of the body's signals may facilitate the regulation of emotional responses, as ongoing bodily changes can be more accurately detected.
There is now evidence that interoceptive responses are associated with immediate discrete emotions (Verdejo-Garcia & Bechara, 2009; Critchley & Garfinkel, 2017). For example, interoceptive accuracy may constitute a positive precondition for effective self-regulation of emotion-driven behavior in healthy individuals (Füstös et al., 2013). Recent research has suggested that there is an association between a person's sensitivity to their own heartbeat and the intensity of the emotion they experience (Herbert, Pollatos, Schandry, 2007; Pollatos, Traut-Mattausch, Schroeder, & Schandry, 2007).
Furthermore, interoceptive awareness plays a role in many higher-order skills such as memory, learning, decision making, and emotion processing. Therefore, a deficit in this measure could increase difficulties in identifying emotions, which in turn, may impact the risk of difficulties in emotional regulation (Critchley & Garfinkel, 2017; Kever et al.,. 2015). Accordingly, several studies (Pollatos, Gramann, & Schandry, 2007; Füstös et al., 2013) conducted in general population have found that a deficit in interoceptive awareness is associated with higher levels of alexithymia—defined as a deficit in the cognitive processing of emotion and the inability to mentally represent emotions, limiting the ability of emotional regulation through cognitive processes (Jakubczyk et al. 2020)—along with lower differentiation in the emotions of others (Terasawa et al., 2014) and less empathy (Grynberg & Pollatos, 2015), among other things. In addition, other studies have reported that measures of heartbeat perception accuracy correlate positively with measures of affective traits, such as a tendency toward general anxiety (Pollatos et al., 2009, Stewart et al., 2001). The evidence as a whole supports the notion that the monitoring and central representation of bodily signals play a critical role in emotion.
Low Dysregulatory Interoceptive Processing
Some research (Brewer, Cook, & Bird, 2016; Shah, Hall, Catmur, & Bird, 2016) has examined the relationship between interoceptive ability and alexithymia, a subclinical construct, traditionally characterized by difficulties in identifying and describing one's own emotions. Currently, evidence suggests that alexithymia may be associated with difficulties in perceiving some non-affective interoceptive cues, such as one's own heart rate. Thus, it is possible that the impairment experienced by people with alexithymia is common to all interoceptive aspects (Murphy, Catmur, & Bird, 2018). In short, this condition would be most clearly characterized as a general failure in interoception (Brewer, Cook, & Bird, 2016).
Low interoception has also been associated with social, sensory, and self-representational symptoms in autistic disorder (ASD) (Quattrocki & Friston, 2014). While the authors surmise that an early pathophysiology in the oxytocin system could disrupt the assimilation of interoceptive cues and exteroceptive cues within generative models of the "self," their empirical evidence supporting this theory speaks to abnormal interoceptive processing and consequent failures in social-emotional learning in ASD. The latter is a pervasive developmental disorder encompassing a group of neurodevelopmental disorders characterized by profound social and verbal communication deficits, stereotyped motor behaviors, restricted interests, and cognitive abnormalities (Quattrocki & Friston, 2014; Fernandez & Scherer, 2017). However, the literature in this regard is inconclusive (Brewer, Cook, & Bird, 2016).
Evidence of conceptual links between alexithymia and interoception has made it possible to assert that atypical interoception represents a central disturbance in psychiatric disorders (Brewer, Murphy, & Bird, 2021). This assertion has been based on the idea that interoceptive deficits appear to represent a "risk factor" for the development of severe mental disorders, however, several issues remain (Brewer et al, 2021), as not all studies are consistent with a relationship between alexithymia and interoceptive accuracy. For example, the results of one study (Nicholson, Williams, Carpenter, & Kallitsounaki, 2019) partly support theories that reference the importance of altered interoceptive processing in the development of ASD. However, while alterations in interoceptive accuracy may be present in children with ASD, as they grow older these difficulties resolve over time, and they may be absent in adulthood (not so the difficulties with mind reading and emotion processing, which remain altered throughout life in ASD).
Moreover, alterations in body awareness have also been implicated in depression. Some studies have revealed that individuals with major depressive disorder (MDD) show alterations related to the sensation, interpretation, and integration of internal body signals (Barrett, Quigley, & Hamilton, 2016, Eggart et al., 2019, Bonaz et al., 2021, Dunne, Flores, Gawande, & Schuman-Olivier, 2021. Empirical data on the relationship between depression and interoceptive processing have increased considerably in the last decade. Functional magnetic resonance imaging (fMRI) studies demonstrate that unmedicated MDD patients show reduced insula activation relative to healthy control volunteers while (a) attending to cardiac, stomach, and bladder sensations (Avery et al., 2014); (b) being exposed to appetizing food imagery (Simmons et al., 2016). Second, MDD has been linked to abnormal behavioral performance on heartbeat counting tasks (Eggart et al., 2019), however, this relationship may not be linear. One study (Dunn et al., 2007) examined the objective accuracy of heartbeat perception in control volunteers, moderately depressed volunteers, and a more severely depressed clinical sample. The moderately depressed participants demonstrated less accurate heartbeat perception than the control group of volunteers. However, contrary to expectations the more severely depressed clinical sample performed better than the moderately depressed sample and equivalent to the control volunteers.
Finally, it is possible to conclude that interoceptive dysfunctions can affect the whole system and are involved in the expression of psychological and physical symptoms in the different acquired and neurological disorders addressed.
High Dysregulatory Interoceptive Processing
Another interesting case to review would be associated with an increased attention to internal stimuli to the detriment of external stimuli. In this line, different studies have investigated the relationship between interoception and anxiety (Pollatos, Traut-Mattausch, Schroeder, & Schandry, 2007; Paulus & Stein, 2010; Paulus, 2013; Büttiker, Weissenberger, Ptacek, & Stefano, 2021). Anxiety is an emotional state associated with a cognitive component of increased attention to the threat to the individual's integrity, together with a complex sympathetic arousal response and different behaviors aimed at avoiding stimuli or contexts that predict a threat to the individual (Paulus, 2013).
Empirical data indicate that (a) the perception of visceral cues (interoceptive awareness) plays an important role in the pathophysiology of anxiety disorders (Pollatos et al., 2007); (b) there is a positive relationship between interoceptive awareness and trait anxiety (Pollatos et al., 2007); (c) given that perceiving bodily states compatible with sympathetic arousal in the absence of external triggers can itself induce anxiety (Paulus, 2013), it is possible that miscommunications between the brain and the body represent a key component of anxiety, where bodily sensations may be under-, over-, or mis-interpreted (Paulus & Stein, 2010) (d) several anxiety disorders have been associated with altered breathing, breathing perception, and response to breathing manipulations (Paulus, 2013).
In this regard, one possible explanatory model posits that anxiety is the result of an increased anticipatory response to possible adverse consequences, which is manifested in increased processing of the anterior insular cortex. Specifically, when anxious individuals receive bodily signals, they cannot easily differentiate between those associated with possible aversive (or pleasant) consequences and those that are part of a constantly fluctuating interoceptive afferent (Paulus & Stein, 2010). Consistent with this model, studies in humans have suggested that the insular cortex plays a central role in the integration and representation of cardiorespiratory and other interoceptive signals (Craig, 2002; Cameron, 2009). Functional neuroimaging studies have revealed that the insula is a key viscerosensory region (Craig, 2009). Moreover, in clinical patients with anxiety disorders, such as panic disorder, specific phobia, social anxiety disorder, and generalized anxiety disorder, abnormal overactivity in the insula has been frequently reported (Brooks & Stein, 2015; Duval, Javanbakht, & Liberzon, 2015; Paulus & Stein, 2010).
The main conclusion is that increased attention to the body does not necessarily lead to an accurate perception of bodily signals. A second conclusion is that it may be associated with misperceptions of internal body states (Leonidou et al., 2020).
Conclusion
This paper has described, based on current research, how interoception has been defined and conceptualized in a non-systematic way. This has led to the widespread practice of extending the definition of interoceptive as the non-exteroceptive, associated purely with the processing of body signals and in a more reductionistic way to the physiological pathways involved. This is problematic, given that this concept is a multifaceted process that relies on different physiological pathways and operates at different levels both temporal and functional. This has led to difficulty in measuring interoceptive dimensions, which in addition to being empirically remote, capture phenomena that in practice have little relation to each other. This reflects a decrease in reliability and validity measurements in the interpretation of the results.
Secondly, beyond the limitations described above, it is possible to link interoception to typical and atypical emotional experience. Evidence was presented that atypical interoception was a common factor among the emotional disorders addressed, and the mechanisms that related it to the symptomatology in the psychopathologies described were also generally delimited. Although several questions are still pending, it is possible to conclude that it is highly likely that deficits in the interoceptive process represent a general risk factor for the development of different mental disorders in the emotional domain. In this sense, alterations or changes in abilities could predispose the development of different psychological disorders and/or function as a comorbid condition to the disorder (as in the case of alexithymia). Furthermore, the idea of a cognitive component associated with interoceptive attention to interoceptive signals is proposed, which could modulate certain symptoms present in anxious and somatic disorders.
Finally, it should be noted that interoception is presented as a bridge between the biological and the psychological, and is a convergence zone for understanding individual differences. Therefore, future empirical work should investigate the factors that determine which manifestations of psychopathology occur after atypical interoception, and whether different interoceptive domains and dimensions are associated with different clinical outcomes. Moreover, progress should be made in identifying interoceptive markers for diagnosis and prognosis, along with new targets for intervention, with the goal of advancing psychological, behavioral, and pharmacological treatments for the management of complex psychopathologies.

