










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Hepatitis C virus (HCV) infection is a serious public health problem, with approximately 71 million people affected by chronic hepatitis C (CHC) worldwide1. Over time, chronic hepatitis C can progress to cirrhosis and liver cancer, representing an important cause of morbidity and mortality among infected individuals1,2.
The development of oral direct-acting antivirals (DAAs) in 2013 replaced treatment based on pegylated interferon (IFN) and ribavirin (RBV)3. This represented a major change in the management and healing perspectives of hepatitis C4, since in addition to greater efficacy and safety4,5, DAAs offer a simpler dosing regimen4,5, a shorter treatment duration and very good tolerance, with no contraindications for liver damage6. A total of 132,851 patients were treated in Spain, from 2015, when DAAs were introduced, up until July 2019. Therapeutic effectiveness was 95.7%7.
At present, the two pangenotypic regimens most commonly used in routine clinical practice for the treatment of chronic HCV infection are a combination of sofosbuvir/velpatasvir (SOF/VEL; NS5B polymerase inhibitor and NS5A replication complex inhibitor) and glecaprevir/pibrentasvir (GLE/PIB; NS3/4A protease inhibitor and NS5A inhibitor)3. The posology and method of administration of these regimens differ. The recommended dose of SOF/VEL is one tablet taken orally once a day with or without food for 12 weeks, while the recommended dose of GLE/PIB is three tablets taken orally once a day with food for 8 weeks.
A change has been observed in the profile of the HCV infected patient who receives treatment for the first time. In the past, only patients with advanced liver disease were treated8, while current patients are usually asymptomatic, with scant liver damage5,8, and not always associated with extrahepatic manifestations. These characteristics imply that the patients are less aware of their liver disease5,8.
The HCV patients are usually polymedicated as a result of their frequent associated comorbidities8,9; in effect, a high percentage receive one or more drugs9. The most common medications include those with actions upon the central nervous system and cardiovascular system10. This factor should be taken into account when starting treatment for hepatitis C infection, because of the potential risk of drug-drug interactions (DDIs)8.
Besides the proven efficacy of DAAs in treating hepatitis C infection3, other factors may determine patient dosing preferences and influence treatment persistence and adherence5,8. Taking patients' preferences into account for different treatments (e.g., for pain and functional or mental disorders) has been shown to provide benefits in terms of adherence and treatment outcomes11. It would therefore be helpful to know more about the treatment preferences of patients referred to the new pangenotypic DAAs for HCV. This study set out to evaluate the preferences of CHC patients who were pending the start of treatment, together with their demographic and diagnostic parameters. These data could lead to a better understanding of the value that patients place on new DAAs and may allow other key stakeholders (policymakers, payers, physicians) to take into account patient perspectives and contribute to shared decision making.
Material and method
A quantitative market research study was carried out in Spain. The study sample was obtained through hepatologists and infectious diseases (ID) specialists involved in treating HCV patients. Neutral recruitment methodology was used, ensuring objectivity and compliance with the inclusion criteria: patients over 18 years of age, diagnosed with chronic hepatitis C, treatment-naïve and pending treatment.
The task of the physician was to explain to the patient the possibility of conducting a survey and the methodology involved. To ensure objectivity in recruitment, physicians included the patients in the order in which they went to their consultations, without considering any other variable that might bias the sample. After checking that patients met the above mentioned eligibility criteria, patients were asked if they would participate in the study. Once consent was given, the physician gave the patient a form that described the purpose of the study, and the patient contact information was collected. After the informed consent was signed, a market research company (Amber Marketing Research) conducted the telephone interview.
The questionnaire used during the interview was designed by Amber and reviewed by Gilead (sponsor). The design of the questionnaire was very simple, easy to do by phone and required no previous preparation. It consisted of 21 fixed items, divided into the following sections: demographic data (n=3), eligibility criteria (n=2), diagnostic data (n=11) and treatment preferences (n=5) (Table 1). The questions were both open-ended and closed. In the closed questions, the patient could choose different answers and was required to select the ones that fitted his/her situation or perception. In the open-ended questions, no answers were suggested, and the patient was free to answer as he/she considered appropriate. The interview lasted approximately 10 minutes. Two dosing options were considered in the question on patient preferences. These options described the two main treatments currently available on the market, based on objective characteristics and the Summary of Product Characteristics. Both treatments have the same price, and it is Price Reimbursed to all patients with no cost for the hospital patient. Therefore, questions regarding economic factors were not added. No brand names or active compounds were mentioned at any time.
Table 1. Questionnaire administered to patients diagnosed with hepatitis C infection and still not undergoing treatment.
| Question | Answer | |
|---|---|---|
| Diagnosis of the disease | ||
| Q1 | Before you were told you had hepatitis C, did you go to the doctor to ask about hepatitis C? That is, did you suspect you could have hepatitis C and went to the doctor because of that, or did the doctor suggest detection tests? | - I went to the doctor to ask about hepatitis C. - The diagnosis was given after evaluation by the doctor. |
| Q2 | Now we are going to talk about the time when you were told you had hepatitis C. How long have you known that you have hepatitis C? | (Years/months/days). |
| Q3 | Which doctor found out you had hepatitis C? | - Family doctor (general practitioner). - Hepatologist. - Specialist in infectious diseases. - Emergency. - Others (specify). |
| Q4 | When the doctor told you that you had hepatitis C, what explanations did he/she give? | (Spontaneous) |
| Q5 | Did the doctor who found out that you had hepatitis C talk to you about the different treatment options available? | 1. Yes. 2. No. |
| Q6 | (Only if Q5 = 1) What did the doctor tell you about the different treatment options available? | (Spontaneous) |
| Q7 | (Only if Q5 = 1) Did the doctor give you the possibility of choosing from different treatment options? | - Yes, he/she explained the different alternatives and allowed me to choose. - No, he/she directly prescribed the option he/she considered best for me. |
| Q8 | Did the doctor tell you which treatment for hepatitis C you would start receiving? | 1. Yes. 2. No. |
| Q9 | (Only if Q8 = 1) What treatment for hepatitis C will you start receiving? If you do not remember the name, please tell us what he/she told you about the treatment you will start receiving. | (Spontaneous). |
| Q10 | Why did you not start the treatment after the visit when you were told you had hepatitis C? | (Spontaneous). |
| Q11 | Approximately how long will it take from when you were told that you have hepatitis C to when you start the treatment? | (Months/days). |
| Preferences when choosing treatment | ||
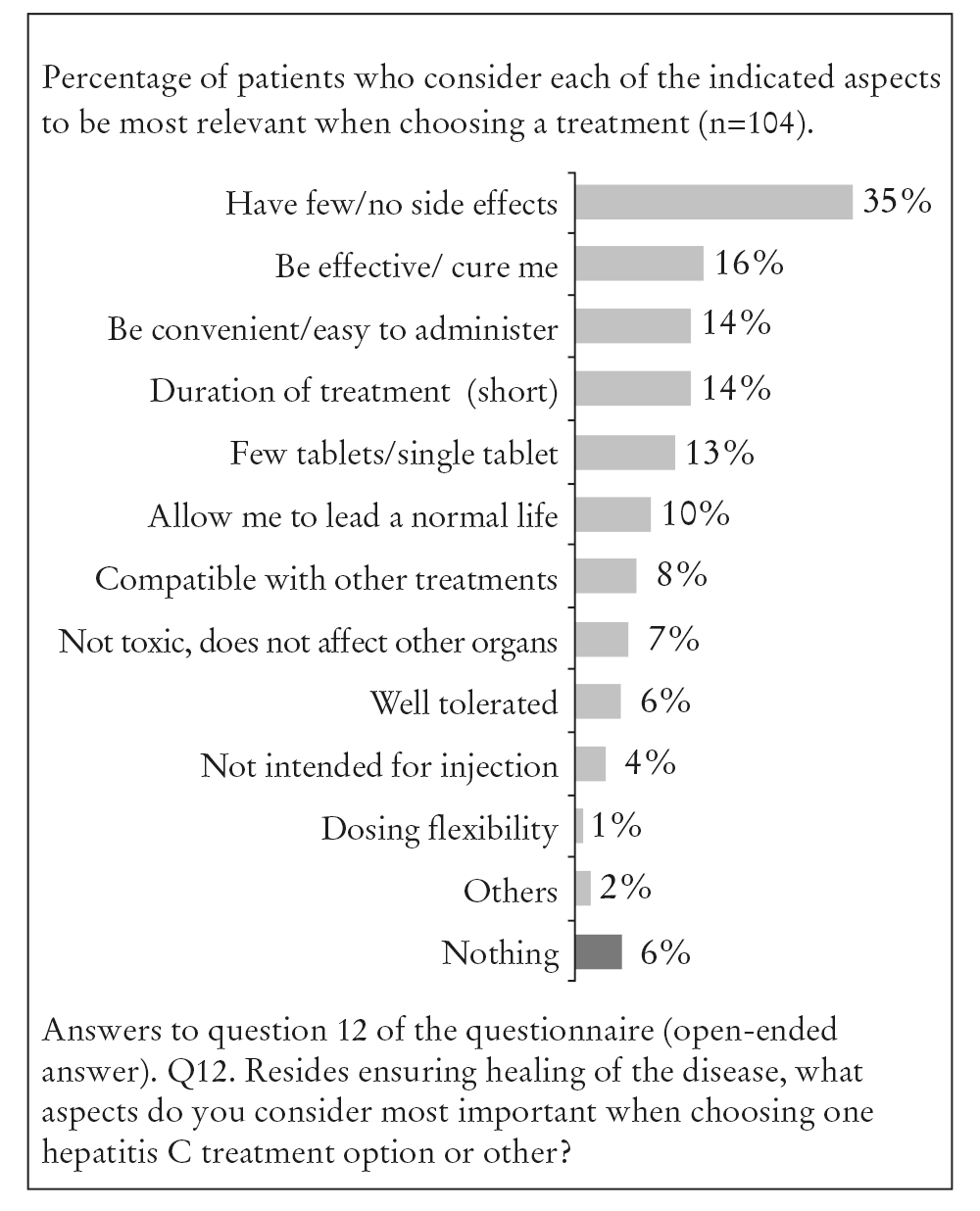
| Q12 | Besides ensuring that the disease is cured, what factors aspects do you consider most important when choosing one hepatitis C treatment option or another? | (Spontaneous) |
| Q13 | How important do you think the following factors are when choosing one hepatitis C treatment option or another? | Please use a scale from 1 to 10, where 1 is “Not at all important” and 10 is “Very important.” |
| Q13.1 | If you could only choose one, which of the above factors would be most important for you when choosing one hepatitis C treatment option or other? | 1. Duration of treatment (weeks/months you need to take the medication). 2. Number of tablets you need to take daily . 3. Flexibility in taking the medication with or without food. 4. Compatibility with other treatments you may be receiving. 5. Possibility of taking the medication any time of day. - Tablet size. |
| Q14 | Now I am going to describe two treatments alternative with different characteristics: • Option 1: treatment that consists of three large tablets a day in a single dose. The tablets should not be crushed or chewed, and always must be taken at the same time of day and after a large meal, for 8 weeks. • Option 2: treatment that consists of a single large tablet a day. The tablet should not be crushed or chewed, and can be taken any time of day and without food, for 12 weeks. If the doctor were to give you the option of choosing between these two treatment alternatives, and assuming that both treatments offer the same chance of curing the disease, which would you prefer? | - Option 1 - Option 2 |
| Q15 | Why? | (Spontaneous) |
Note. Items refer to diagnosis and treatment preferences (n = 104).
The fieldwork and analysis of results was carried out exclusively by Amber, and the participants' confidentiality was assured at all times.
A descriptive analysis was performed and so a sensitivity analysis was not required. The open-ended questions were categorised according to similarity in order to quantify similarity. The study was carried out under strict confidentiality standards. Accordingly, neither the interviewers or physician nor the participating patients were informed about the sponsor (Gilead Sciences) of the study or about the companies to which each of the proposed dosing alternatives belonged.
In Spain, this type of study (market research) does not require the approval of Research Ethics Committees (RECs). All subjects provided informed consent to participate in the study.
The research was conducted in accordance with Spanish Organic Law 15/1999 on Personal Data Protection and the relevant industry guidelines, including Aedemo and ESOMAR.
Results
The study was conducted between November 2018 and January 2019. A total of 104 patients from 21 centers in 7 different Spanish regions (Autonomous Communities) were included; 64% were males (n=67). The mean patient age was 49 years (median: 50 years; interquartile range (IQR): 14.25) (males: 48 years; females: 49 years), and 54% of the patients (n=56) were ≥ 50 years of age.
Most patients (85%; n=88) were diagnosed after the physician carried out an active search strategy. The diagnosis was established by the primary care physician (PCP) in 42% of cases. The diagnosis for the other patients was established by hepatologists (26%), ID specialists (17%) internal medicine specialists (6%), gynecologists (3%) and physicians of the Emergency Department (6%). The diagnosis of hepatitis C was established in an average of 7.3 ± 9.7 years before the survey, less than one year in 44% of cases (n=46) (mean 4 months; range: 1-11 months) and over 5 years in 35% of cases (n=36) (mean 19 years; range: 6-35 years).
The reasons for not starting treatment are reported in Table 2. The estimated mean time to treatment initiation after diagnosis was 15 months (IQR: 116 months; range: 1-360 months). A total of 3.6% (n=3) started treatment in the first month after diagnosis, and 24.1% (n=20) in the first three months after diagnosis. Seventy percent of the study participants were informed by their doctor about the treatment they were going to receive.
Table 2. Reasons why the patients diagnosed with hepatitis C infection had not yet started treatment
| Reason | % patients (n) |
|---|---|
| Other health problems/comorbidities | 31% (32) |
| I have other health problems; it's not the right moment | 27% (28) |
| Incompatibility with other treatments | 11% (11) |
| Currently asymptomatic | 17% (18) |
| Awaiting the latest tests (laboratory tests, viral load, etc.) | 16% (17) |
| They just told me I had to wait | 10% (10) |
| I'm waiting for a second opinion (specialist) | 6% (6) |
| Personal decision | 6% (6) |
| I'm starting soon | 6% (6) |
| The treatment has not arrived | 6% (6) |
| Others | 4% (4) |
| Doesn't know | 7% (7) |
Note. Popen-ended question (n = 104 patients).
Alongside treatment efficacy when selecting treatment with DAAs, the patients mentioned side effects (35%), ease of administration (14%), treatment duration (14%) and the number of tablets (13%) (Figures 1 and 2).

The responses to the two treatment options in the questionnaire (Q14-Table 1) showed that 72% of the patients preferred one single large tablet a day that is not crushed or chewed and can be taken at any time of day with or without food for 12 weeks (Option 2), while 28% of the patients preferred three large tablets a day in a single dose, without crushing or chewing, and always taken at the same time of day after a large meal for 8 weeks (Option 1) (Figure 3). The preference for option 2 was statistically significant (estimated by 95% confidence intervals). This preference was independent of patient age according to the chi-square statistic (< 50 years [n=48]: 69% and ≥ 50 years [n=56]: 75%; p=q=0.5)- and was driven by multiple characteristics such as being a single tablet (41%), convenience (36%), time flexibility (33%), and not having to take the medication with food (24%) (Figure 3).The main reason for choosing option 1 was the shorter duration of treatment (83%).

Discussion
The aim of this study was to determine patient preferences for treatment with the new DAAs of treatment naïve patients with CHC. This factor, which depends on each individual patient, should be taken into account when selecting an HCV treatment, since it might have a positive impact on adherence and clinical outcomes. The general characteristics of the study population were similar to those recently described in a very large series of hepatitis C patients in Spain10. In both cases, males were the predominant gender, and patients over 50 years of age predominated over those under 50 years of age.
In most cases (42%), the initial diagnosis of hepatitis C was made by PC physicians, which would confirm the key role of these professionals in the active identification of patients (through adequate screening)12.
Over 35% of the interviewees in our study would choose a therapeutic option with fewer adverse events (AEs). This observation is consistent with the data from another recent report on direct antiviral preferences, in which patients with hepatitis C were surveyed from existing market research databases (Welzel et al.)13. Despite the fact that protease inhibitor (PI)-based regimens show a higher frequency of AEs14, mainly gastrointestinal side effects (diarrhea, nausea, vomiting) and metabolic complications, no increase in serious AEs has been observed with DAA treatment in clinical trials or real life studies. The most commonly reported ones are insomnia, nausea and headache15-17.
For the patients in the study by Welzel et al.13, the most important characteristics for hepatitis C treatment were: great efficacy, lesser risk of specific AEs (nausea, diarrhea or headache) and duration (the most relevant dosing characteristic). The study13 showed that 60% of the patients had already been treated or were receiving treatment at the time (approximately 50% were cured). In our study, the patients had not yet received treatment for hepatitis C infection, which is a key difference between both studies, as currently the majority of the patients are treatment-naïve patients with different dosing preferences to the ones that are treatment-experienced.
The number of tablets was an important attribute for the patients in our study when assessing the therapeutic regimen. However, in the study of Welzel et al.13, taking a greater number of tablets had no significant impact. This could be explained by the different profiles of the patients included in the two studies: treatment-naïve patients representing the current situation, versus treatment-experienced patients, including regimens such as interferon (31%)13, which is currently a less frequent profile.
It has been shown before that the number of DAA tablets in patients with hepatitis C, with a high pill-burden, is associated with poorer adherence8,18. Single-tablet regimens result in improved adherence8 and also simplify consultation19, making it possible to shorten the average visiting times (doctor, nurse, pharmacist)19.
The aspects related to treatment comfort, such as flexibility in taking the medication with or without food and at any time of the day, were also positively appreciated by 13% and 9% of the patients, respectively. Both GLE and PIB show pH dependent dissolution in an aqueous medium, and it is important to take this drug combination with food in order to increase its solubility and bioavailability20. The mean systemic exposure to both drugs (GLE and PIB) has been shown to increase with food containing a moderate to high fat content21. For this reason, GLE/PIB should be administered with food.
In the case of the SOF/VEL combination, bioavailabity is not affected by food, the combination therefore can be taken with or without food.
The option of a single tablet for 12 weeks was the greatest preference (72%), regardless of age (< 50 or ≥ 50 years). The administration of a single tablet, time flexibility, convenience and not having to take the medication with food were salient features. The patients who chose three tablets for 8 weeks (28%) stated that the main reason for this choice was shorter treatment duration (83%). Seven percent of the patients who chose option 1 cited fewer tablets as the reason; reflecting misinterpretation of the question (SOF/VEL total number of tablets 84 in 12 weeks, GLE/PIB total number of tablets, 168 in 8 weeks).
Most of the patients included in our study had a recent diagnosis (under one year [47%]), but 35% had known about their disease for more than 5 years (mean 19 years; range: 6-35 years). The mean delay between diagnosis and the treatment initiation was 15 months. This is an important point, since the time between diagnosis and the start of treatment may be an indicator that should be considered when evaluating hepatitis C elimination plans.
The main reason for not yet starting treatment (31%) was the presence of comorbidities, which are common in the current patient profile. Another lesser reason was the absence of symptoms (17%), reflecting patient unawareness of the risk of disease progression. Treatment delay due to comorbidities is usually attributable to contraindications or interactions of DAAs with concomitant treatments22. Combinations of DAAs without protease inhibitors (PIs), such as SOF/VEL, exhibit fewer interactions than PI-based regimens (GLE/PIB), because their metabolism is not dependent upon cytochrome P45010. Furthermore, they have a better safety profile, particularly in patients with advanced liver disease. In relation to this, the United States FDA issued an alert warning in August 2019 about the possibility of serious liver damage with the use of DAAs including a PI such as GLE, grazoprevir and voxilaprevir, in patients with advanced liver disease or with risk factors such as alcohol abuse or hepatocarcinoma.
The main strength of our study is the fact that patients selected were treatment-naïve, which reduces the likelihood of answers conditioned by patients' previous experiences. Another strength is the method used to recruit the patients, where they are included by the specialists themselves rather than by existing panel members of market research firms. In addition, the fact that the two treatment options proposed in our study correspond to those currently available on the market (Spain) could imply a greater impact of these results on routine clinical practice and a better understanding of patient preferences for the attributes of new DAAs and may improve the efficiency in the shared decision-making process when managing these patients. It is important to note that there are very few published studies on the preferences of chronic hepatitis C patients when taking pangenotype DAAs.
There are several limitations to this study. One limitation is the possible misinterpretation of some questions, as reflected by the answers regarding the number of tablets in the GLE/PIB regimen, or the comment that a longer treatment makes it more effective. However, the percentage of such cases is very low and does not invalidate the overall results. Another limitation of the study is the fact that 7 out of every 10 respondents had already received some information about the treatments they were going to receive. This could influence patients' decisions regarding their preferences for one of the options. A further limitation could be lack of knowledge of the cultural level of the patients when interpreting the results - this data was not asked for in the patient interview. On some occasions there is a limitation in question Q14 of the questionnaire, where a large meal was mentioned when considering Option 1. Flexibility in taking the drug with or without food did not emerge in the top 3 leading considerations for choosing a treatment; hence it is unlikely that any characterization of the food requirement with the Option 1 product profile had a significant bearing on the overall preference elicitation.
In conclusion, the results of our study show that the majority of treatment naïve CHC patients prefer to be treated with one tablet for 12 weeks versus three tablets for 8 weeks. This reflects the great importance of dosing simplicity and flexibility, including the absence of any need to take the medication with food.
Despite the availability of highly effective DAAs that can cure hepatitis C and prevent its long-term consequences, there are still patients who have not started treatment after diagnosis. Messages that mentione these characteristics of the DAAs, along with the other advantages, such as a very good safety profile, need to be reinforced in ongoing physician training.
The results of our study indicate the importance of considering patient preferences in treatment decision making. This may have an impact on key aspects such as therapeutic adherence and persistence in current hepatitis C patients, improving clinical outcomes in CHC patients.

