










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
HC is very common amongst inmates inside and outside Spain1. The prevalence of infection in Spain dropped from 4.3% in 2018 to 1.1% in 2019, thanks to treatment with direct-acting antivirals2, which are highly effective for inmates and non-inmates alike3.
Therapy with direct-acting antiviral drugs is a cost effective strategy that reduces transmission and increases survival amongst inmates, while also reducing liver complications and the costs of managing the disease4. Treating all inmates with HC would practically eliminate infection, but this is not an easy process given the special characteristics of this population (time in prison, transfers, etc.). If these characteristics are not taken into account, then some patients may not be treated, others may not receive treatment promptly or may have it interrupted.
Strategies have been designed to optimise treatment: a) increase detection; b) ensure referral to specialist services; and c) simplify evaluation and therefore minimise loss of patients. The latter measures require simplification in calculating the level of fibrosis, usually measured with TE. This technique quantifies the elasticity of the liver, and shows liver rigidity or fibrosis. TE is very effective and has some important advantages (fast, painless, bloodless and free of side effects), but although it is simple to use, it does require trained personnel5 and not all medical services have this system available.
In the case of Spanish prisons, the FibroScan®, (TE apparatus) service is rotated between centres, and so is available, but with the limitation of availability that depends on a rotation schedule, which does not always coincide with the time in prison of inmates with HC. This means that studies are sometimes left incomplete and treatment is not prescribed. TE can sometimes be replaced by biochemical parameters, such as APRI and FIB-4, which allow fibrosis to simply calculated in a matter of minutes. Reliability increases when the two methods are combined, especially in extreme cases (low level of fibrosis or cirrhosis)6. Our objective in this study is to determine the concordance between TE and the APRI and FIB-4 NIM in inmates with chronic HC and without advanced fibrosis.
Material y method
Observational and retrospective study of inmates with chronic HC at the prisons of Brians 1 and Brians 2, treated by the two primary healthcare teams of Sant Esteve Sesrovires in 2019.
The inclusion criteria were as follows: a) diagnosed with chronic HC (persistently high HCV ribonucleic acid [RNA]); and b) received a TE fibrosis test in 2019.
The following inmates were excluded: a) ones who did not have the necessary parameters for calculating APRI and FIB-4; b) who presented results of TE with a success rate or ratio of under 75%; and c) who presented an interquartile range (ratio between the number of valid measurements and the total number of measurements) of under 10%. The result of the TE was expressed in units of kPa.
The TE fibrosis calculation was compared to the APRI and FIB-4 combined method. The analytical study for the NIM could not exceed six months from the date of the TE. The following variables were gathered: age, sex, background, drug use and form of consumption, HCV RNA, viral genotype, HIV infection and direct-action antiviral treatment prescription.
The levels of fibrosis 0, 1, 2, 3 and 4 and a TE result of <7.5 kPa, 7.5-9 kPa, 9.1-12.5 kPa, 12.6-14 kPa and ≥14 kPa, respectively, were considered. It was estimated that there was no advanced liver disease if the TE outcome was ≤12.5 kPa. Although the cut-off point habitually used to establish a fibrosis at stage 3 or higher is 9.5 kPa, we used the cut-off point of 12.5 kPa recommended by Foucher J. et al.7, which has a positive predictive value of 90%. However, the cases that presented a cut-off point between 9.5 kPa and 12.5 kPa were checked to see if there was a discordance between the TE and the NIM.
The following were considered in the case of the NIM: F0-F1: APRI <0.5 or FIB-4 ≤1.45; F2: APRI 0.6-1.5 and FIB-4 1.46-3.25; and F3-F4: APRI >1.5 and FIB-4 >3.25. This scale was based on the meta-analysis of Lin ZH. et al.8, who investigated the diagnostic capacity of the APRI in 40 studies on 8,739 patients with chronic HC, which found that an <0.5 algorithm value reliably ruled out the presence of significant fibrosis.
A >3.25 cut-off point was used for the FIB-to detect advanced fibrosis (≥F3), since this cut-off showed a positive predictive value of 65% and a specificity of 97% in these cases9. The combination of APRI and FIB-4 was finally chosen given that it is believed to enable the intermediate results to be more effectively classified10.
If the TE did not detect fibrosis compatible with ALD, the TE concordance compared to NIM was determined with the index k = Po-Pe/1-Pe, where Po is the proportion of the concordance observed on a per unit basis, and Pe is the proportion of concordance expected by pure chance. The margins established by Landis y Koch (Table 1)11 were used to evaluate the degree of concordance.
Table 1. Distribution and strength of concordance for categorical data10.
| k value | Strength of concordance |
|---|---|
| < 0,20 | Poor |
| 0,21-0,40 | Weak |
| 0,41-0,60 | Moderate |
| 0,61-0,80 | Good |
| 0,81-1,00 | Very good |
Note: k: kappa.
The study was carried out in accordance with the international ethical recommendations (Helsinki Declaration and Oviedo Convention) and the laws of best clinical practice. Personal data was processed in accordance with Organic Law 3/2018 of 5 December, on the Protection of Personal Data and Guarantees of Digital Rights, and European General Data Protection Regulation 2016/679. The study is retrospective and observational in nature and therefore the patients could not be informed or asked to sign the relevant informed consent document, Conventional clinical practice could not be altered either. The study was approved by the Prison Health Programme of the Catalan Health Institute.
Results
107 cases were included, 82 of which could be evaluated. The other 25 were excluded for not having undergone an analysis in the previous six months or for not possessing any of the analytical parameters that enabled the APRI and/or FIB-4 to be calculated or because they did not meet the reliability criteria described in the materials and methods section.
The average age was 42 years (SD: ±3.2). 79 were men (96.4%). 51.2% were Spanish and 39% were co-infected with the human immunodeficiency virus. The majority (59.7%) were genotype 1. Of these, 45.1% were exclusively genotype 1 and 14.6% were mixed genotypes (genotype 1 plus one other).
As regards drug use, 70 (85.4%) presented a background of IDU, 6 (7.3%) declared that they consumed drugs non-intravenously, and another 6 (7.3%) did not consume illegal drugs.
Only 8 of the persons studied (9.8%) presented ALD according to the TE results. There were 8 discordant results while 2 of them corresponded to cases between 9.5 and 12.5 kPa, which the NIM graded as F3. There was no discordance between both methods in low stages (F0-F1) or in cirrhotic cases (F4). Figure 1 shows the cases analysed according to the level of fibrosis. In the 74 cases that did not present ALD, the concordance between TE and NIM via the k index was 0.78.
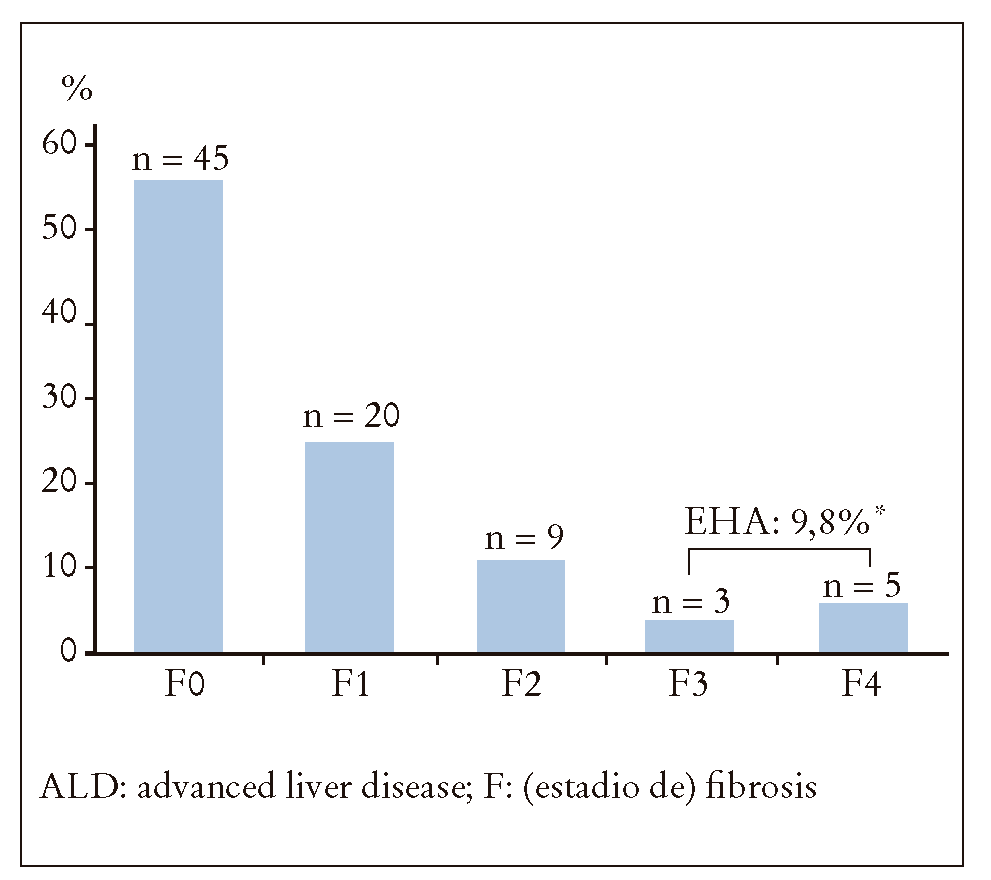
Figure 1. Distribution of cases analysed according to level of fibrosis. There were two cases measured between 9.5 and 12.5 kilopascals that could have been considered as stage 3 fibrosis under other measurement criteria. With such a method, cases with advanced liver disease would have been 10 (12.2%)*.
In the year when the HCV study including TE was carried out, anti-HCV treatment was prescribed for 65 inmates (79.3%). 17 (20.7%) were not prescribed said therapy.
Discussion
This study found that TE and the combined use of APRI and FIB-4 in cases without ALD had good concordance. The usefulness of NIMs in predicting fibrosis has been widely studied and supported, even in published meta-analyses6,8,12. A study by Portilla et al.13 concluded that such indices were useful for identifying patients without advanced fibrosis (negative predictive value of 93% and 88%, respectively), which is precisely the population under study in the article. However, the results of the indices in the study by Portilla et al.13 were compared with the liver biopsy and not with the TE, which was the method we used and the one most widely used to measure liver fibrosis in patients with HC.
Cases without ALD are now very common (>90% of the cases analysed in this study fall without this group) and therefore the results of this study would have practical applications for many cases of HC, which we consider to be very important. Furthermore, the infected population was a group of prison inmates who were younger and more frequently infected as a result of IDU and generally with less years of infection on average than infected cases outside prison3, which has been associated with a lower prevalence of fibrosis9.
Another aspect to take into consideration is that both the TE and the NIM lose precision if they are used on cases with intermediate stages of fibrosis, but it has been suggested that in such situations the biomarkers may be more reliable and definitely have a much lower economic impact than TE10. In this study, there was a discordance of 9.7% between both methods, and this took place in intermediate stages and not in patients with low levels of fibrosis (F0-F1) or in cirrhotic patients (F4), as was observed in other studies6.
A limitation of this study is that it was carried out in a specific geographical area, and it may not be possible to extrapolate the socio-demographic characteristics and drug use patterns to other parts of Spain.
However, we feel that it is unlikely for the characteristics of IDUs to change significantly with regard to HCV infection from one area to another, regardless of their variable of prevalence between Spanish regions. Another possible limitation is that the "n" analysed (82 patients) is not very low but neither is it very high. However we believe that the homogeneity of the results obtained in the sample makes this detail less important.
It is also important to point out that the cut-off point used to determine ALD (12.5 kPa) has a high positive predictive value (90%), but also has a negative predictive value of 80%. There is therefore a risk of cases that may be ALD not being classified as such. However, this factor does not appear to have had a serious impact on the study, since there were only two cases (2.4%) that presented results between 9.5 and 12.5 kPa in which there were discrepancies between the NIM, which were classified as F3, and the TE, which was classified as F2.
Finally, this study suggests that the NIM are useful instruments for calculating fibrosis, and can very effectively substitute TE when there are availability issues for this test and there are cases of HC without ALD. This option is not so important for hospital units where TE is fully available. However, it can be vital for units outside the hospital setting, especially in resources such as drug dependency units14 or prison healthcare centres11, which often treat patients such as intravenous drug users where treatment is important for public health and should be prescribed promptly to prevent transmission.
Therefore the combined use of the APRI and FIB-4 in the prison setting is recommended for infected patients, where TE is not available; especially when the stay in prison is a short one and there is a high risk of transmission.

